Article Text

Abstract
Aim To evaluate the effectiveness of customised foot orthoses in chronic mid-portion Achilles tendinopathy.
Methods This was a participant-blinded, parallel-group randomised controlled trial at a single centre (La Trobe University, Melbourne, Australia). One hundred and forty participants aged 18–55 years with mid-portion Achilles tendinopathy were randomised to receive eccentric calf muscle exercises with either customised foot orthoses (intervention group) or sham foot orthoses (control group). Allocation to intervention was concealed. The Victorian Institute of Sports Assessment-Achilles (VISA-A) questionnaire was completed at baseline, then at 1, 3, 6 and 12 months, with 3 months being the primary end point. Differences between groups were analysed using intention to treat with analysis of covariance.
Results After randomisation into the customised foot orthoses group (n=67) or sham foot orthoses group (n=73), there was 70.7% follow-up of participants at 3 months. There were no significant differences between groups at any time point. At 3 months, the mean (SD) VISA-A score was 82.1 (16.3) and 79.2 (20.0) points for the customised and sham foot orthosis groups, respectively (adjusted mean difference (95% CI)=2.6 (−2.9 to 8.0), p=0.353). There were no clinically meaningful differences between groups in any of the secondary outcome measures.
Conclusions Customised foot orthoses, prescribed according to the protocol in this study, are no more effective than sham foot orthoses for reducing symptoms and improving function in people with mid-portion Achilles tendinopathy undergoing an eccentric calf muscle exercise programme.
Trial Registration Number Australian New Zealand Clinical Trials Registry: number ACTRN12609000829213.
- Achilles
- Podiatry
- Physiotherapy
- Soft tissue
- Eccentric
Statistics from Altmetric.com
Background
Mid-portion Achilles tendinopathy is a common, chronic disorder of the Achilles tendon characterised by pain and swelling within the mid-portion (2–6 cm proximal to the calcaneal insertion) of the tendon. In athletic populations, Achilles tendinopathy has a prevalence of up to 19%1–5 and a cumulative lifetime incidence of 24%.6 Achilles tendinopathy is also common in non-athletic people, as one-third of those with this condition are sedentary.7–10
Foot orthoses are a non-surgical intervention that have been recommended in clinical practice guidelines for the treatment of mid-portion Achilles tendinopathy.11 The biomechanical rationale for their use has not been fully established.12 Hypothesised mechanisms include that they (1) reduce the bending stress within the Achilles tendon by correcting abnormal eversion of the calcaneus in the presence of excessive foot pronation,13 (2) increase rearfoot movement variability14 and/or (3) improve activation of the triceps surae, vastus lateralis and gluteus medius musculature, and this results in reduced Achilles tendon strain.15 ,16
Preliminary evidence indicates that foot orthoses improve symptoms of individuals with Achilles tendinopathy.17–19 Mayer et al17 performed the only randomised controlled trial to date, which compared customised foot orthoses to a no-intervention control group in athletes with mid-portion Achilles tendinopathy. After 4 weeks, the customised foot orthosis group demonstrated a significantly greater improvement in pain scores. However, it is possible that the positive symptom-modifying effects of the foot orthoses in this study may have been overestimated since the study lacked key recommended clinical trial characteristics to minimise bias, including allocation concealment and participant blinding.20 Further, additional criticisms of previous trials in this area include the lack of use of disease-specific functional outcome measures20 ,21 and incomplete descriptions of the foot orthoses interventions used.20 Therefore, we conducted a robust randomised controlled trial to determine the effectiveness of customised foot orthoses in people with mid-portion Achilles tendinopathy.
Methods
Design
This was a participant-blinded, parallel-group randomised controlled trial using a sham control group with 1, 3, 6 and 12-month follow-ups. All clinical assessments were performed at a university clinic (La Trobe University, Melbourne, Australia). Musculoskeletal ultrasound assessments were performed at a radiology department of a private hospital (Southern Cross Medical Imaging, La Trobe University Medical Centre). All participants provided informed consent. The trial was registered with the Australian New Zealand Clinical Trials Registry (number ACTRN12609000829213). The trial protocol has been described elsewhere.22
Participants
The study was advertised in several Melbourne (Australia) newspapers, mail-outs to local medical and allied health professionals, internet websites, as well as posters displayed in community centres, sporting clubs and universities in Melbourne. The selection criteria defined eligible participants as those who: were aged 18–55 years; had symptoms in the mid-portion (2–6 cm proximal to the insertion) of the Achilles tendon of one or both lower limbs for at least 3 months duration; were literate in English and able to complete the Victorian Institute of Sports Assessment-Achilles (VISA-A) questionnaire;23 scored less than 80 on the VISA-A questionnaire; regularly used footwear that could accommodate customised foot orthoses (this was defined as using footwear that can accommodate foot orthoses for at least 90% of the time during weightbearing activities); and those who would be willing to not receive any physical therapy on the involved Achilles tendon(s) or trial of foot orthoses or bracing (other than those allocated in the current study) during the study period.
Exclusion criteria for participants in this study were: previous Achilles tendon surgery in the symptomatic lower limb(s); previous Achilles tendon rupture in the symptomatic lower limb(s); previous lower limb trauma that has caused structural imbalance (e.g. ankle fracture); osseous abnormality of the ankle (e.g. anterior or posterior tibiotalar osteophytes) in the symptomatic lower limb(s); inflammatory arthritis (e.g. ankylosing spondylitis); metabolic or endocrine disorders (e.g. type I or II diabetes); neurological disorders (e.g. Charcot-Marie-Tooth disease); previous breast cancer and/or use of oestrogen inhibitors; treatment with foot orthoses, heel lifts or eccentric calf muscle exercises within the previous 3 months; disorders of the Achilles tendon that were not mid-portion tendinopathy (such as paratendinitis and insertional Achilles tendon disorders); fluoroquinolone usage within the previous 2 years; injection of local anaesthetic, cortisone or other pharmaceutical agents into the symptomatic Achilles tendon(s) or surrounding area within the previous 3 months; injury or pathology of the feet, knees, hips and/or back or any condition that, in the opinion of the investigators, may have interfered with participation in the study.
Achilles tendinopathy was diagnosed from a clinical assessment using the criteria of: insidious onset of pain in the Achilles tendon region, which was aggravated by weightbearing activities and/or was worse in the morning and/or during the initial stages of weightbearing activities; and pain located 2–6 cm proximal to the Achilles tendon insertion. Grey-scale musculoskeletal ultrasound imaging of the Achilles tendon was performed by a qualified sonographer with a 13.5 MHz linear transducer (Siemens Anatares, Siemens, Germany) to confirm the diagnosis. Achilles tendinopathy was confirmed when the presence of local thickening (anterior–posterior) and/or irregular fibre orientation and/or irregular tendon structure with hypoechoic areas and/or vascularisation existed within the mid-portion of the Achilles tendon.22 If both Achilles tendons fulfilled the selection criteria, the most painful side was selected for the study.
Randomisation and blinding
Participants were randomised to one of two groups: an intervention group (customised foot orthoses) or a control group (sham foot orthoses). Both groups received a 12-week eccentric calf muscle exercise programme based on the method of Alfredson et al,24 as this was considered usual care.22 To maintain blinding, participants were advised that they would receive one of two types of ‘shoe inserts’ during the study. Allocation to either group was achieved using a computer-generated random number sequence that was generated and held by an external person not directly involved in the eligibility assessment, data collection or analysis. The allocations were concealed from the investigators enrolling participants in sequentially numbered opaque, sealed envelopes.25 Owing to the nature of the interventions, it was not possible to blind the staff administering the interventions.
Interventions
Data collection and the interventions were administered by three experienced qualified podiatrists (SEM, LAS and DRB). Participants were requested to refrain from receiving other forms of intervention. They were, however, advised to take 500 mg of paracetamol on an ad hoc basis if the tendon(s) were painful.
Standardised advice on the amount of activity allowed during the study was provided to participants. Participants were advised to continue their activities after receiving their allocated intervention; however, they were advised to keep their Achilles tendon pain under level 5 on a numerical rating scale (NRS), where 0 indicated no pain and 10 indicated worst pain imaginable, during the activity.26 This approach allows participants with Achilles tendinopathy to continue with some level of activity during rehabilitation and has shown equivalent outcomes to programmes that involve complete rest from the aggravating activity with no negative effects.26
Customised foot orthoses
Participants randomised to this group received customised foot orthoses for both feet. The basic contour of the shell of all of the customised foot orthoses was based on the description of the modified Root style of orthosis,36 and posted to vertical.36 All customised foot orthoses were manufactured from polypropylene with a 400 kg/m3 ethylene vinyl acetate (EVA) rearfoot post and a shell-length covering fabric (Nora Lunasoft SL 2 mm). The foot orthoses were customised using the information obtained from assessment of the foot posture of each foot (using the Foot Posture Index27) and the participants’ body mass (see online supplementary file 1). The style of foot orthosis has previously been shown to be most commonly prescribed in clinical practice.28
Sham foot orthoses
Participants randomised to this group received sham foot orthoses for both feet, which acted as a control. This intervention has been described in detail previously.22 The sham foot orthoses were manufactured from 4 mm thick EVA with a density of 90 kg/m3. They had an identical covering fabric and a similar shape to the customised foot orthoses however, they provided negligible mechanical support as the arch flattened on minimal compressive force. This form of device has been used as a sham condition in a previous trial,29 and a recent study30 has validated it as a credible sham.
Outcome measures
Outcome measures were performed at baseline, then at 1, 3, 6 and 12 months. The primary outcome measure was the VISA-A questionnaire.23 The VISA-A questionnaire contains 8 questions that cover 3 domains of pain, function and activity. Scores were summated to give a total score out of 100, where higher scores indicated less severe Achilles tendinopathy; so an active, asymptomatic person would theoretically score 100.23 The secondary outcome measures were: participant perception of treatment effectiveness using a 5-point Likert scale (dichotomised according to success, where ‘success’ was defined as marked or moderate improvement, which were the two best scores on this scale);31 level of physical activity in the previous week (7-day Physical Activity Recall Questionnaire)32; health-related quality of life (eight domains of the Short-Form-36 (version 2; SF-36) questionnaire33; and use of cointerventions (rescue medication, other treatments and footwear changes) to relieve pain at the Achilles tendon(s).
We also assessed the frequency of adverse events and adherence with the eccentric calf muscle exercise programme and foot orthoses.22 Adverse events (any events for which there is a known or plausible association with treatment and those for which there is none34) were recorded using a questionnaire that participants completed at 1, 3, 6 and 12 months. Adherence with the eccentric calf muscle exercise programme was measured by daily registration in a diary. Participants documented the number of repetitions and sets performed for each day of the exercise programme (12 weeks). From this, we calculated the total number of repetitions during the first 12 weeks. Adherence with the foot orthoses was assessed at 1, 3, 6 and 12 months. Participants provided information concerning the number of hours per day and number of days they have worn their foot orthoses during the previous week. From this, we calculated the total hours worn during the previous week at these time points.
Sample size
The sample size for the trial was determined using an a priori sample size calculation.22 The trial was powered to detect a clinically worthwhile difference in the primary outcome measure of the total score of the VISA-A questionnaire.23 One hundred and forty participants (i.e. 70 per group) provided greater than 80% power to detect an effect of 10 points on the VISA-A questionnaire, with the significance level set at p<0.05, an estimated SD of 20.0 and a drop-out rate of 10%.
Statistical analysis
If the participant had bilateral symptoms, data from the most painful side were recorded and analysed, to satisfy the assumption of independent data.35 Statistical analysis was performed using IBM SPSS (V.21.0) using the intention-to-treat principle.36 The exception to this was for the adverse events outcome measures, which were analysed as treated. Multiple imputation was used to replace missing data for continuous scaled outcome measures, using five iterations, with baseline scores, group allocation and age as predictors.37 The exceptions were the perception of treatment effectiveness and use of cointerventions, which were analysed as documented.
Differences between groups for the primary outcome measure (VISA-A questionnaire), and continuous scaled secondary outcome measures (physical activity and SF-36) that were normally distributed, were analysed at 1, 3, 6 and 12 months using analysis of covariance (ANCOVA) with baseline scores and intervention group entered as independent variables.38 The primary end point was 3 months, which was considered standard follow-up time.22 Independent t tests were used to evaluate differences between groups for adherence with the eccentric calf muscle exercise programme and foot orthoses.
We calculated the relative risk, absolute risk increase and number needed to treat or harm for the dichotomised measure of participant perception of treatment effectiveness; the frequency of adverse events; and participant reported use of cointerventions.39 For each measure, the 95% CI was reported as a measure of estimate uncertainty. In all analyses, p values <0.05 were considered statistically significant.
Sensitivity analysis was performed to determine the robustness of our study findings in the context of participant attrition. Differences between groups for the primary outcome measure (VISA-A questionnaire) were analysed at 3 months, our primary end point, using ANCOVA with baseline scores and intervention group entered as independent variables for the following conditions: (1) complete case analysis (including only those participants from whom measurements were recorded), (2) assuming that participants from whom outcome data were not available recorded a maximum possible score (i.e. 100 points) or (3) assuming participants from whom outcome data were not available recorded a minimum possible score (i.e. 0 points).40
Results
Study recruitment and follow-up
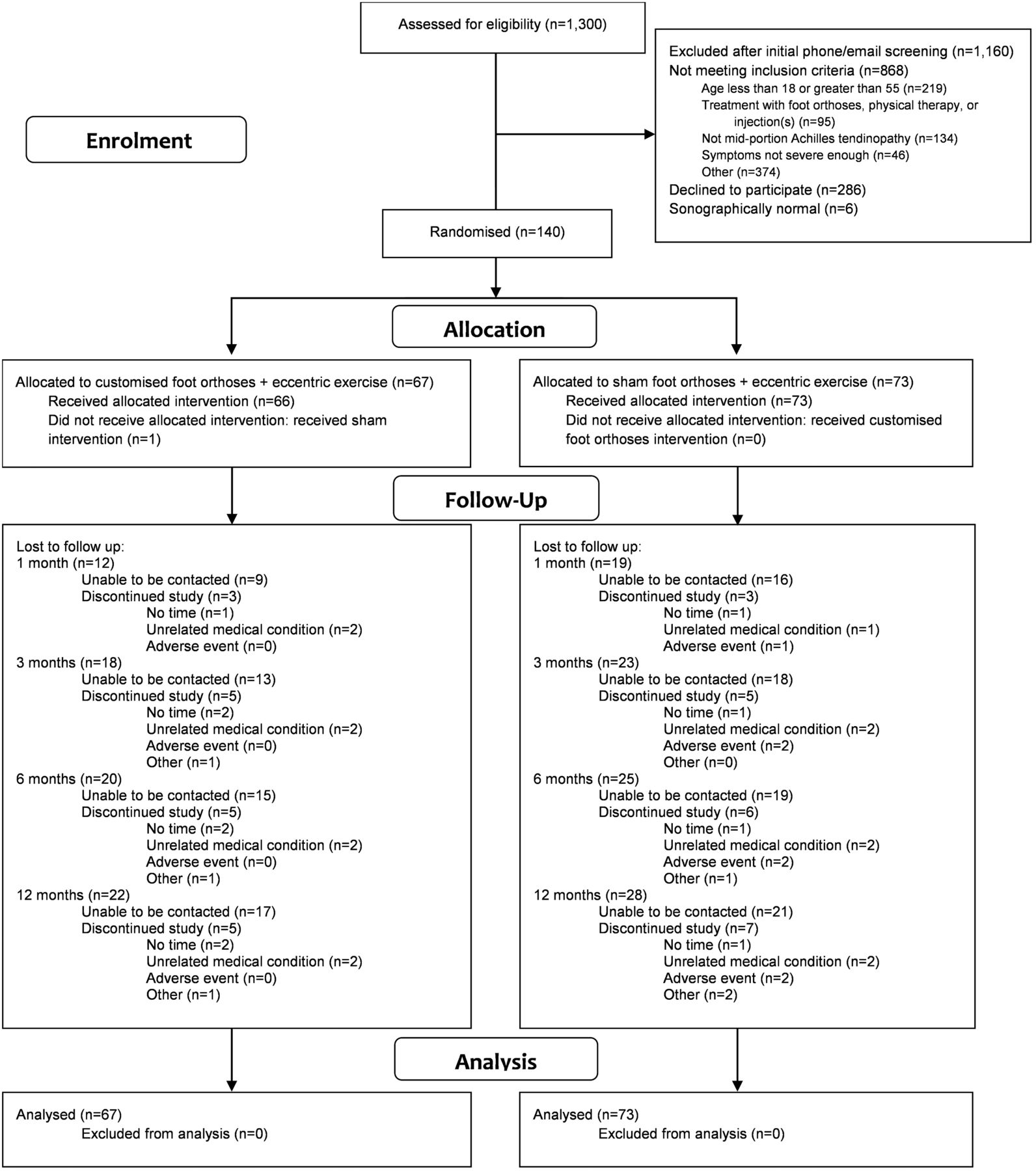
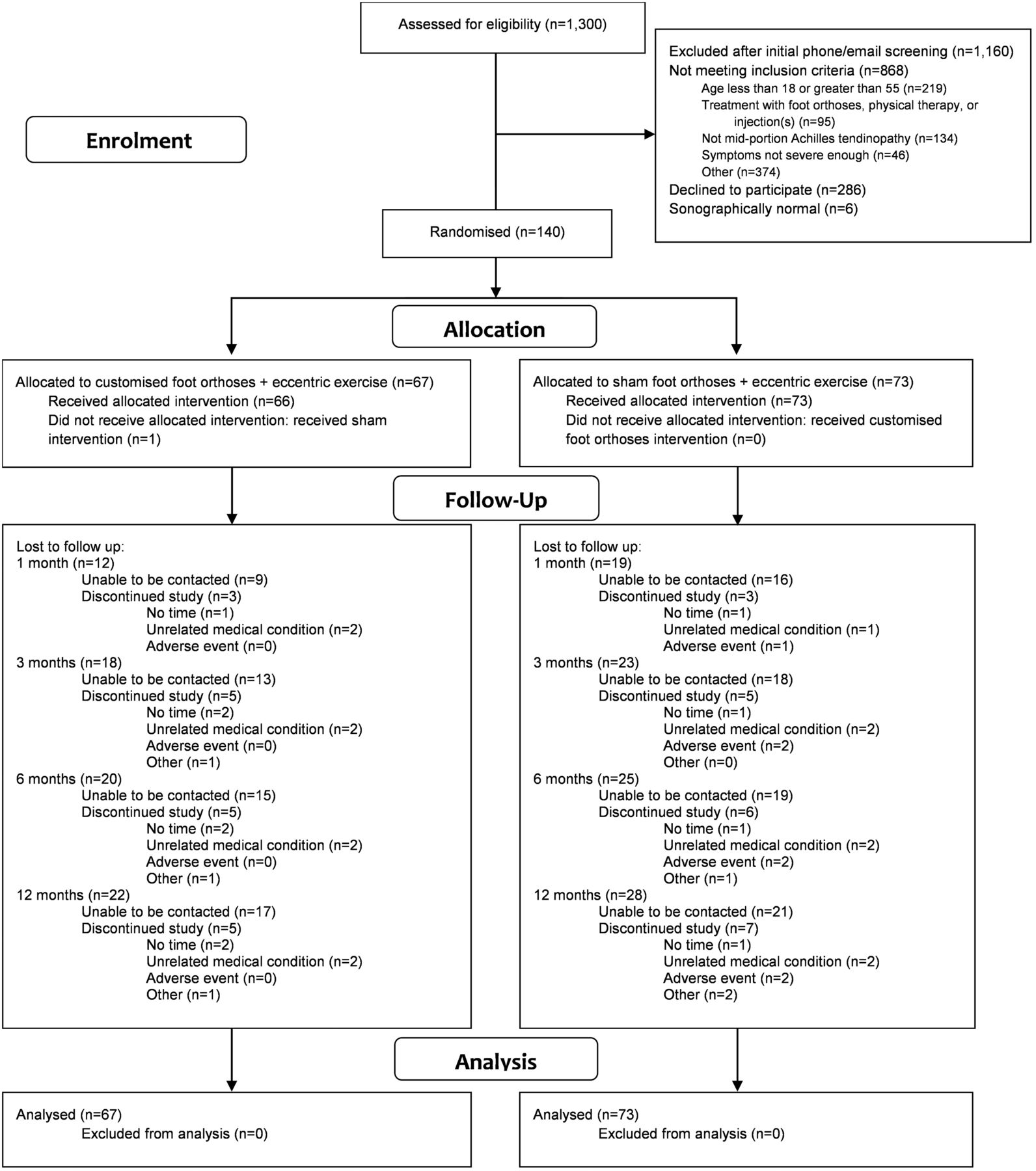
From July 2009 to June 2012, 1300 volunteers were screened and 140 were enrolled in the study (figure 1). Sixty-seven participants were allocated to the customised foot orthosis group, and 73 participants were allocated to the sham foot orthosis group. Baseline characteristics of the groups were well matched (table 1). One participant allocated to the customised foot orthosis group received sham orthoses in error. The trial was completed in June 2013, with 109 (77.9%) participants followed up at 1 month, 99 (70.7%) at 3 months, 95 (67.9%) at 6 months and 90 (64.3%) at 12 months.
Baseline characteristics of participants
{kind=link}
Flow of participants through the study.
Treatment effectiveness: primary outcome measure
Both groups displayed improvements in VISA-A questionnaire scores compared with baseline, but there were no statistically significant differences between the groups at any time point (table 2).
Mean scores and mean differences (95% CIs) between groups for the VISA-A score (adjusted for baseline score)
Treatment effectiveness: secondary outcome measures
There were no statistically significant differences between groups for the secondary outcome measures, participant perception of treatment effectiveness (table 3), level of physical activity in the previous week (see online supplementary file 2), or use of cointerventions (see online supplementary file 3). At 6 months, there was a statistically significant difference in favour of the sham foot orthoses for the general health domain of the SF-36 (adjusted mean difference (95% CI)=−4.7 (−8.1 to −1.3), p=0.007), but this difference is unlikely to be clinically meaningful (see online supplementary file 4).
Self-reported perception of treatment effectiveness expressed as event rate (%) for each group, absolute risk increase, relative risk and number needed to treat*
Adverse events
There were no statistically significant differences in the proportion of participants reporting adverse events (table 4). There were no serious (i.e. life-threatening, required hospitalisation, or resulted in persistent or significant disability or incapacity34) adverse events. The majority of adverse events were pain or soreness within lower limb or lower back, and the majority of these were within the feet. Overall, two participants, both from the sham foot orthosis group, withdrew from the study due to adverse events (one participant developed knee pain, the other developed a lower limb stress fracture; figure 1).
Frequency of self-reported adverse events expressed as event rate (%) for each group, absolute risk increase, relative risk and number needed to harm*
Participant adherence
Both groups reported performing approximately 57% of the total number of prescribed eccentric calf muscle exercise repetitions over the 12 weeks. The customised foot orthoses were reported to be worn for 48–58 h/week during the study. There were no statistically significant differences between groups in these variables (table 5).
Adherence with the eccentric calf muscle exercise programme and use of foot orthoses based on self-report*
Sensitivity analysis
Sensitivity analysis was performed due to the high participant attrition rate. There were no notable differences in participant characteristics between groups for the randomised participants (table 1) and the participants who provided 3-month outcomes (complete case analysis; see online supplementary file 5). Further, there were no statistically significant differences between groups at the 3-month time point when we performed complete case analysis or when missing data were replaced with the maximum or minimum possible score (see online supplementary file 5).
Discussion
This is the first participant-blinded randomised controlled trial to investigate the effectiveness of customised foot orthoses for the treatment of mid-portion Achilles tendinopathy. There were no statistically significant differences between the intervention groups (customised versus sham) in the primary outcome measure at any time point during the study. Further, the associated CI for each of these comparisons did not include the predefined clinically meaningful difference of 10 points in favour of treatment with the customised foot orthoses. These findings indicate that customised foot orthoses were no more effective than sham foot orthoses for the treatment of mid-portion Achilles tendinopathy in participants who also undertook an eccentric calf muscle exercise programme over a 12-month time period.
Rigorous study design and use of sham orthoses
Previous studies have reported that customised foot orthoses are beneficial for Achilles tendinopathy.17–19 However, two of these studies were a case series study design,18 ,19 and the only randomised controlled trial17 lacked key characteristics to minimise bias.
Unlike previous studies,17–19 we used rigorous randomised controlled trial methods, as well as a sham foot orthosis intervention to blind study participants allocated to the control group, and this is likely to explain the difference in results between previous studies and our study. This explanation is supported by a recent systematic review of the effectiveness of insoles for medial knee osteoarthritis, where beneficial effects of insoles were not observed when only high-quality trials that incorporated a sham control group (rather than a no-treatment control) were included in the analysis.41
Limitations
The findings of this study need to be interpreted in the context of three main limitations. First, there are no empirically supported guidelines for the prescription of customised foot orthoses, so the observed lack of effect of the customised foot orthoses may not be generalisable to alternative orthotic prescription protocols. However, the prescription used in our study was based on what is commonly used in clinical practice in Australia and New Zealand.28 Further, it is unknown if foot posture is predictive of treatment response to foot orthoses, so the inclusion of participants with all foot postures may have masked any treatment effects.
Second, although McCormick et al30 recently concluded that the sham foot orthoses manufactured from the same materials as in our study were a credible sham intervention (i.e. participants rated them as credible), their biomechanical analyses of these orthoses showed that they reduced plantar pressures at the heel, which suggests that they exert some mechanical effects. We did not conduct plantar pressure assessment (or any other biomechanical assessment such as kinematic analyses), so we cannot confirm this effect and influence in our participants. Nevertheless, the primary postulated effect of foot orthoses on Achilles tendinopathy relates to kinematic change and not redistribution of plantar pressures, so we doubt this would have had a significant effect.
Third, participant attrition was a major limitation of our study. However, we believe that this is unlikely to have biased the results as (1) the rate of attrition was very similar between groups, (2) the characteristics of participants who provided data at the 3-month time point were similar to those randomised at baseline and (3) the study results for differences between groups for our primary outcome measure did not change when we performed sensitivity analyses.
Participant attrition is unlikely to have caused our study to be underpowered. Our original sample size calculation estimated that the SD of the primary outcome measure (VISA-A) would be 20 points.22 However, in the current study the pooled SD at baseline was lower (i.e. 16.9 points). As a result, our study still provided at least 80% power to detect an effect of 10 points on the VISA-A questionnaire assuming a minimum sample size of 90 participants.
Additional clinical considerations
An important consideration of our study design is that we did not perform a head-to-head comparison of customised foot orthoses versus eccentric calf muscle exercise. Rather, we sought to determine if the foot orthoses would be effective in addition to participants performing an eccentric calf muscle exercise programme. We designed our trial this way because eccentric calf muscle exercises are a commonly recommended, inexpensive intervention for mid-portion Achilles tendinopathy,11 ,20 with foot orthoses frequently prescribed in addition to the exercises. Furthermore, this is the most commonly used study design in trials of other physical therapy interventions for Achilles tendinopathy.20
In conclusion, customised foot orthoses were no more effective than sham foot orthoses for reducing pain and improving function and activity in people with mid-portion Achilles tendinopathy undertaking an eccentric calf muscle programme. Thus, the addition of customised foot orthoses, administered according to the protocol used in this trial, is not recommended for mid-portion Achilles tendinopathy.
What are the new findings?
In clinical practice, foot orthoses are commonly prescribed for mid-portion Achilles tendinopathy. Evidence from high-quality randomised controlled trials has been lacking.
We found that customised foot orthoses provide no benefit for reducing pain and improving function in people with mid-portion Achilles tendinopathy undertaking an eccentric calf muscle exercise programme (part of guideline care).
Customised foot orthoses are not recommended for mid-portion Achilles tendinopathy in the setting of patients undertaking prescribed eccentric exercises.
How might it impact on clinical practice in the near future?
Provides evidence against clinicians prescribing customised foot orthoses for mid-portion Achilles tendinopathy.
Further strengthens the evidence for eccentric calf muscle exercise as the first-line treatment for mid-portion Achilles tendinopathy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online customised-foot-orthoses
- Data supplement 2 - Online PhysicalActivity
- Data supplement 3 - Online Co-interventions
- Data supplement 4 - Online SF36scores
- Data supplement 5 - Online Sensitivityanalysis
Footnotes
Contributors All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. SEM, KBL, TP, JLC and HBM were involved in study concept and design. SEM, LAS and DRB were involved in acquisition of data. SEM and HBM were involved in statistical analysis and interpretation of data. SEM was involved in drafting of the manuscript. LAS, DRB, KBL, TP, JLC and HBM were involved in critical revision of the manuscript for important intellectual content. SEM, KBL, JLC and HBM obtained funding.
Funding This study was funded by the Prescription Foot Orthotic Laboratory Association (PFOLA). Footwork Podiatric Laboratory Pty Ltd (Melbourne, Australia) donated the customised foot orthoses for this study.
Competing interests HBM is currently a National Health and Medical Research Council Senior Research Fellow (ID: 1020925). JLC was supported by the Australian Centre for Research into Sports Injury and its Prevention, which is one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee (IOC).
Ethics approval La Trobe University Human Ethics Committee, number UHEC 08-114.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Participant level data are available from the corresponding author at s.munteanu@latrobe.edu.au. Informed consent was not obtained but the presented data are anonymised and risk of identification is low.