Article Text

Abstract
Background Running has been critical to human survival. Therefore, the high rate of injuries experienced by modern day runners is puzzling. Landing on the heel, as most modern day shod runners do, results in a distinct vertical impact force that has been shown to be associated with running-related injuries. However, these injury studies were retrospective in nature and do not establish cause and effect.
Objective To determine whether runners with high impacts are at greater risk for developing medically diagnosed injuries.
Methods 249 female runners underwent a gait analysis to measure vertical instantaneous loading rate, vertical average loading rate (VALR), vertical impact peak (VIP) and peak vertical force. Participants then recorded their mileage and any running-related injuries monthly in a web-based, database programme. Variables were first compared between the entire injured (INJ; n=144) and uninjured (n=105) groups. However, the focus of this study was on those injured runners seeking medical attention (n=103) and those who had never injured (n=21).
Results There were no differences between the entire group of injured and uninjured groups. However, all impact-related variables were higher in those with medically diagnosed injuries compared with those who had never been injured. (effect size (ES) 0.4–0.59). When VALR was >66.0 body weight (BW)/s, the odds of being DX_INJ were 2.72 (95% CI 1.0 to 7.4). Impact loading was associated with bony and soft-tissue injuries.
Conclusions Vertical average loading rate was lower in female runners classified as ‘never injured’ compared with those who had been injured and sought medical attention.
- Biomechanics
- Injuries
- Overuse
- Prospective
Statistics from Altmetric.com
Introduction
Endurance running is an important activity as it has been suggested to be critical to our evolutionary survival.1 Therefore, it may be considered one of the most natural ways to become and remain fit. Running is extremely popular with over 20 million Americans who run on a regular basis.2 We evolved to run barefoot which has been typically associated with a mid-foot or forefoot strike pattern.3 ,4 However, modern cushioned running shoes allow one to land comfortably on the heels. Thus, it is not surprising that up to 89% of shod runners today land with a rearfoot strike pattern.5 ,6
A rearfoot strike pattern has a characteristic impact transient in the vertical ground reaction force, not typically seen in a mid-foot or forefoot strike pattern (figure 1).7 This impact transient is associated with high rates of loading.8 It has been reported that the viscoelastic structures of the musculoskeletal system do not respond well to these impulsive loads. Radin et al9 noted that impulsive loads led to stress fractures in rabbit tibia. This research group also found that joint cartilage is also affected by impulsive loading.10 While there was no damage to bovine cartilage with slow repetitive loading, the addition of periodic impact loading led to rapid cartilage wear. These animal studies provide a basis for the association between high rates of loading and musculoskeletal injury.
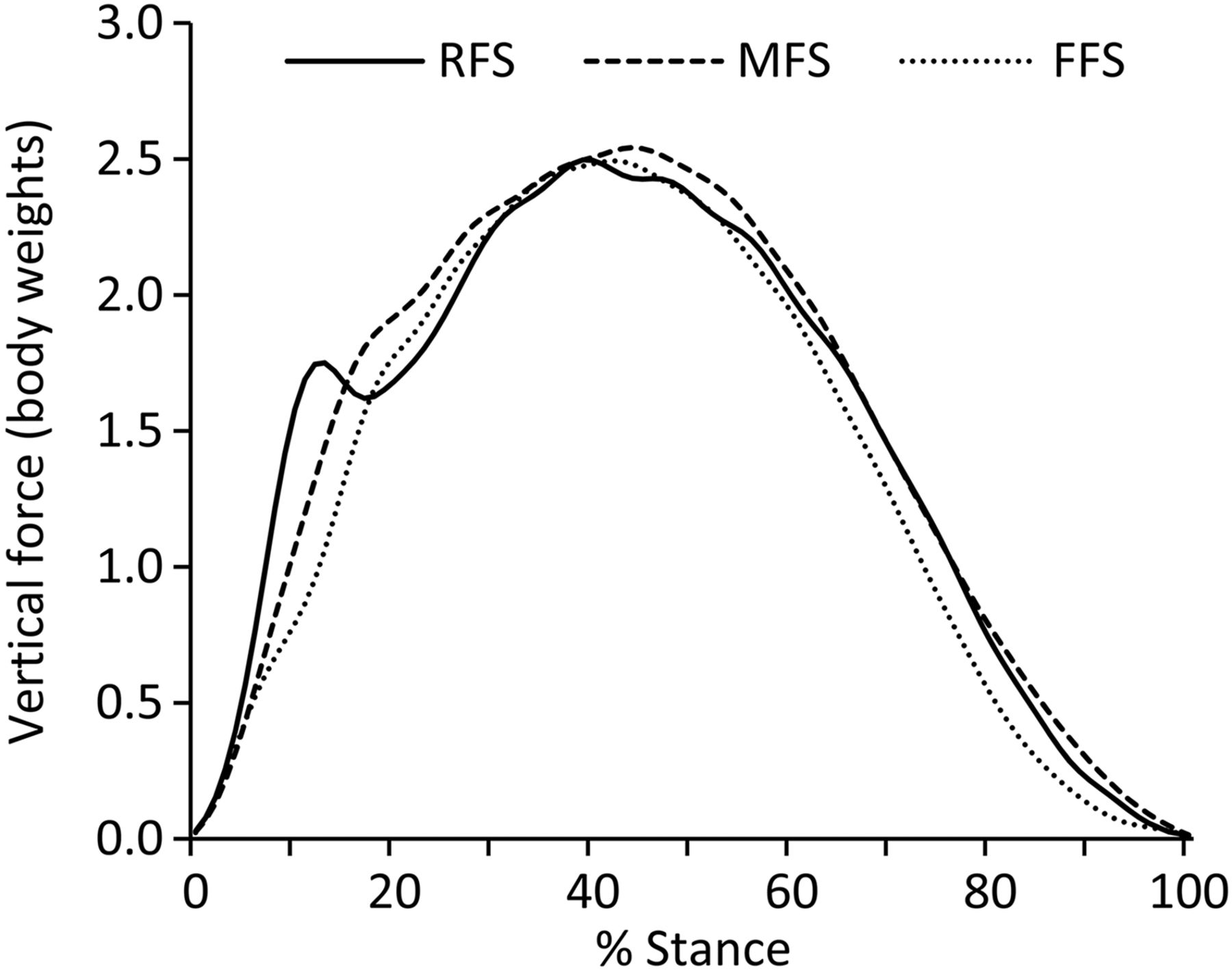
Vertical ground reaction force of a rearfoot (RFS), mid-foot (MFS) and forefoot strike (FFS) landing during running: Note the distinct impact peak associated with a rearfoot strike pattern that does not occur in the mid-foot or forefoot strike landing.
Increased impulsive loading in humans has also been associated with injury. Runners with a history of tibial stress fractures exhibited greater vertical rates of loading during the impact phase of stance than their healthy counterparts.8 Similar findings of increased vertical load rates, as well as increased vertical impact peaks (VIPs) were reported for runners with a history of plantar fasciitis.11 Interestingly, although peak vertical forces (FVs) are typically twice that of the impact peak, they did not distinguish between the injured from the uninjured group in either of these studies. Both of these studies were retrospective in nature. As a result, one cannot discern whether the increased load rates preceded the injury or if the injury caused a change in mechanics and resulted in an increase in the load rates. Therefore, prospective studies are needed to better estimate the relationship between increased vertical impact loading and injuries in runners.
We aimed to compare variables related to the impact peak of rearfoot strike runners who go on to develop a medically diagnosed running injury to those who have never been injured. It was hypothesised that runners who went on to develop a diagnosed running-related injury would have higher VIPs, vertical load rates, than those who did not become injured. We also sought to develop a prediction and calculate the odds of those who would go on to develop an injury based on their impact loading.
Methods
Participants
A sample of female recreational runners between the ages of 18 and 40 years, running a minimum of 20 miles per week were recruited from the local running community. Runners had to be injury free at the time of inclusion and for the previous 6 months. After providing informed consent, all potential runners were initially screened with video (120 frames per second) to determine their footstrike pattern as they ran across the laboratory at 3.7 ms. Only those who made initial contact with their heel bilaterally were invited to participate in the study (n=249). The study was approved by the local institutional ethics committee.
Data collection
All participants underwent a baseline instrumented gait analysis. Participants wore standard, neutral running shoes (Air Pegasus, Nike, Inc., Beaverton, Oregon, USA) during the screening and all subsequent data collections. They ran at 3.7 ms (±5%) across a force plate (Bertec Corp, Worthington, Ohio, USA) located in the centre of a 25 m runway. Ground reaction force data were sampled at 1080 Hz and filtered at a cut-off frequency of 50 Hz using a second order, recursive, Butterworth, low pass filter.
Data analysis
A custom programme written in LabVIEW (National Instruments, Austin, Texas, USA) was used to process the data. The outcome variables of interest were the vertical instantaneous load rate (VILR), vertical average load rate (VALR), VIP and FV (figure 2). A threshold of 10 N in the vertical ground reaction force was used to identify foot strike and toe off, thereby determining the stance phase. The FV was the maximum force on the vertical ground reaction force curve. The VIP was defined as the local maximum between foot strike and FV. This usually occurred within the first 50 ms. of stance phase). The VILR was calculated as the maximum slope of the vertical ground reaction force curve between successive data points in the region from 20% to 80% from foot strike to VIP. This was the most linear portion of the curve in the early part of stance. In cases where the VIP was missing from the vertical ground reaction force, the force value at 13% of stance was used.12 The VALR was the slope of the line through the 20% and 80% points. Aside from FV, all variables were associated with the impact phase of running. The ICCs for these force variables of interest fall between 0.93 and 0.95, with SEMs between 0.088 and 7.116.13 The discrete variables from each of five trials per participants were calculated, then averaged for each participant, and then averaged across groups.

Calculation of outcome variables: (A) vertical impact peak (VIP), vertical average load rate (VALR), vertical instantaneous load rate (VILR), Peak Vertical Force (FV).
Injury analysis
A custom developed web-based database programme was implemented so that each runner could report their monthly mileage (that they tracked weekly) and any running-related injuries that they experienced. While any pain experienced during running was recorded, we were most interested in those injuries that did not resolve on their own and led the runner to seek medical attention. This definition of injury is commonly used in the running literature.14–20 This database was used over a 2-year follow-up period. An automated reminder system was used to prompt the runner to log into the secure website and report their mileage and injuries each month. If the runner did not respond in 3 days, another reminder was sent. If no response was received after three additional days, the study coordinator contacted the participant directly. This system was designed to maximise participant compliance.
At the end of the 2-year period, the participants were first categorised into two groups: All those that were injured (INJ) versus all those who remained uninjured (UNINJ). Of the injured group, those who sought medical attention for their injury (by a physician, physical therapist, athletic trainer, etc) during the course of the study were defined as the diagnosed injured group (DX_INJ). Of the uninjured group, those who had never sustained a running injury prior to enrolling in this study were identified (NEV_INJ). The NEV_INJ have historically been a highly unstudied group.
Statistical analysis
Following removal of outliers, identified as outlier scores on a boxplot, data were tested for assumptions of normal distribution (Shapiro-Wilks, p>0.05) and homogeneity of variance (Levene's test, p>0.05). Where the assumptions were met, independent t tests (α<0.05) were performed (VIP, VALR, VILR, FV). Effect sizes were calculated using Cohen's d (Mean1–Mean2)/pooledSD) and interpreted as 0.2 small, 0.5 medium, >0.8 large. Where the assumptions were violated (age, miles), the outliers were retained and analysed using a Mann-Whitney U test. An effect size estimator r (Z/sqrt(N) and interpreted as 0.1 small, 0.3 medium, >0.5 large). The analyses were conducted on the entire sample between INJ and UNINJ, and between the DX_INJ and NEV_INJ. In addition, a post hoc analysis was conducted between the NEV_INJ group and a subgroup of the DX_INJ group who had not been previously injured (DX_INJ_NPI).
Based on the primary hypothesis to compare DX_INJ and NEV_INJ groups, all biomechanical variables, as well as mileage, for these groups were entered into a forward binary logistic regression. This regression provided a means to account for any shared variance and to identify the variables that best distinguished the injured from uninjured runners. This variable was then further analysed in a 2×2 contingency table containing the frequencies of the DX_INJ versus NEV_INJ groups compared to low versus high exposure of that variable. Based on previous literature,8 where the variables were calculated in the same way and for a similar sample of runners, the exposure was categorised as low or high for the values of the control group. For example, for VALR the exposure is low and high if below and above 66.0 body weight (BW)/s, respectively. From the logistics regression and this contingency table data, the odds of exposure and significance were calculated using χ2.
The injury type and location were presented for all injuries. To assess which injuries were most often associated with high-impact loading, the distribution of injuries that were associated with the 10 highest values for each impact variable were counted. These frequency counts are of the injuries, for which some participants had more than one, and not a count of the participants. All other descriptive statistics are presented as means±SD. All statistical analyses were conducted in SPSS Statistics V.19 (IBM, Armonk, New York, USA).
Results
Use of the custom web-based, database system, resulted in an overall reporting compliance rate of 91%. Of the 249 runners followed, 144 (58%) sustained an injury, including 103 who sought medical attention (DX_INJ group) and 41 who did not (figure 3). Of the 105 (42%) runners who remained uninjured (UNINJ) during the study, 21 (8%) had never been injured (NEV_INJ). The participants in each of the groups (INJ, UNINJ, DX_INJ, and NEV_INJ) were well matched for age (table 1). The INJ and UNINJ groups ran similar mileage. However, the NEV-INJ group ran seven miles per week less than the DX_INJ group.
Demographics of the analysed groups

Definition of the injured and uninjured groups: The diagnosed injured group (DX_INJ) (n=103) was comprised of runners who sought medical treatment for their injuries. The never-injured (NEV_INJ) group (n=21) had never sustained a running-related injury. *Primary comparison of interest.
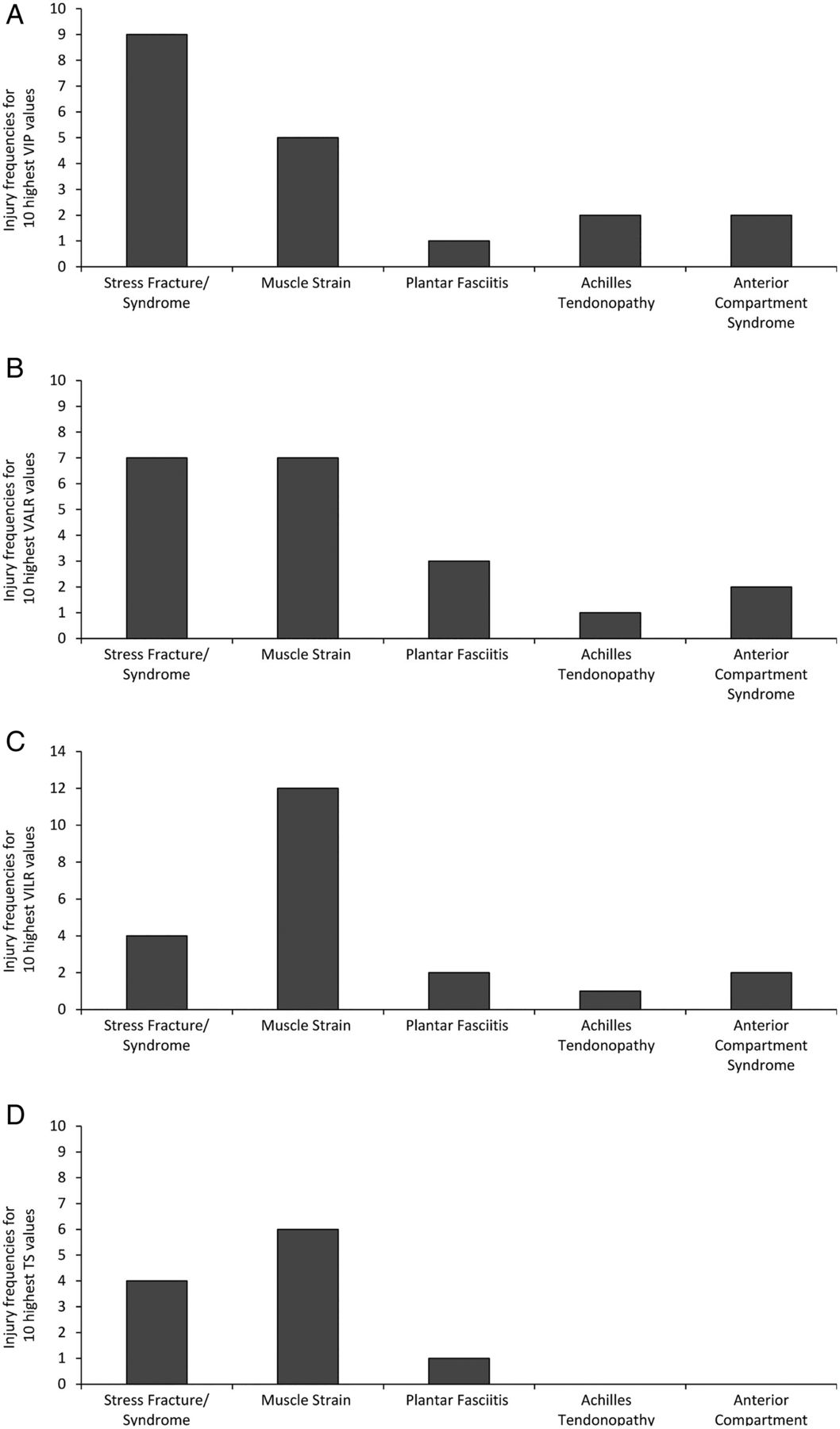
There were 239 injuries that were medically treated over the 2-year period. The type and location of these diagnosed injuries are presented in table 2. Muscular strains and tendinitis were the most common types of injuries (41.6% of the total) and most injuries occurred from the knee distally (65.3%). The 10 highest values for each impact variable were associated with a variety of, and often several injuries (figure 4). However, stress fractures/syndromes and muscle strains were the injuries most commonly associated with high-impact loading across each of the variables.
Number of injuries (n=239) by type and location for the INJ group

Distribution of injuries associated with the 10 highest values of each of the variables of interest: Bony injuries (ie, stress fractures/syndromes) as well as soft tissue injuries (ie, muscle strains) were associated with high-impact loading. This suggests that impact loading plays a role in a wide range of running injuries. Note: the 10 individuals with the highest values of each variable may have had more than one injury so that the total number of injuries exceeds 10; the highest 10 values may be associated with different participants for each of the variables.
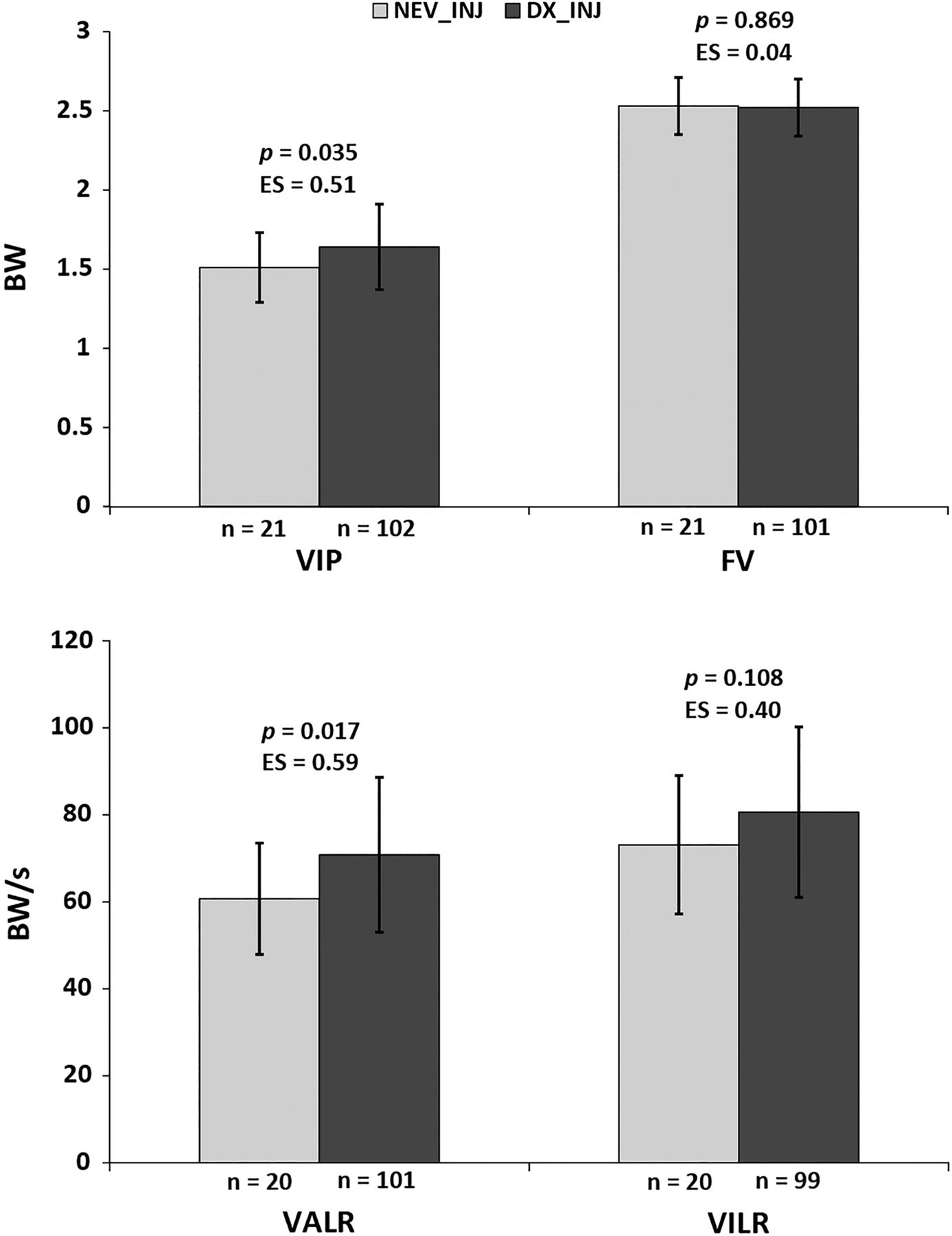
The comparison of the biomechanical variables between the groups is seen in table 3 and figure 5. No differences were noted in any of the variables when assessing the entire group of INJ versus UNINJ (table 3). However, when assessing the subgroups of interest, which is those who have never been injured (no prospective nor retrospective injuries, NEV_INJ) versus those who had medically diagnosed injuries (DX_INJ), results were quite different. Aside from FV which is not an impact variable, VIP and VALR were significantly lower in the NEV_INJ group. As having a previous injury is a risk factor for a future injury,21 we were also interested in controlling for this factor by comparing the NEV_INJ to DX_INJ_NPI (table 4). All three impact variables were significantly higher in this subgroup of injured runners, despite these injured runners never being previously injured.
Comparison of entire group
Comparison of the never injured with those medically diagnosed with their first injury

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of force variables between primary groups of interest: Note that, compared with the never injured group (NEV_INJ), VIP and VALR were significantly greater in injured group who sought medical attention (DX_INJ). These were associated with large effect sizes. VILR was not statistically greater in the medically diagnosed injury group, but the effect size approached a medium effect. FV, peak vertical force; VALR, vertical average load rate; VILR, vertical instantaneous load rate VIP, vertical impact peak.
To account for the often high shared variance between biomechanical variables, the logistic regression analysis revealed that VALR alone significantly distinguishing between the DX_INJ and NEV_INJ groups. The exposure to the VALR criterion was statistically significant (NEV_INJ low n=13; NEV_INJ high n=7; DX_INJ low 41; DX_INJ high n=60; p=0.045) with odds of the DX_INJ group being 2.72 (95% CI 1.0 to 7.4) times more likely than the NEV_INJ group to be injured based on exposure to a VALR greater than 66.0 BW/s. Consequently, VILR, VIP, FV and mileage did not make a significant contribution to predicting injury that had not already been accounted for by VALR alone.
Discussion
The purpose of this prospective observational study was to examine whether high-impact loading was associated with running-related injuries. The central hypothesis was that the impact transient associated with rearfoot striking is related to injury. When assessing the entire injured versus uninjured groups, no differences were found. However, when comparing those who sought medical treatment for their injuries to the group of runners who had never sustained an injury, all impact-related variables (besides the peak vertical ground reaction force) were higher in the injured groups studied.
Injuries
The incidence of injuries in our study was generally consistent with other prospective cohorts. In a systematic review of these studies, between 19.4 and 92.4% of individuals sustain lower extremity injuries during running.22 There was a large range in the length of time for following injuries, from between 1 day at a race event to 18 months. When assessing the studies with a 6–18 month follow-up, the incidence ranged between 31.6% and 84.9% for an average of 54%. This is consistent with the 58% of the runners in our study who sustained a prospective injury. The distribution of injuries were similar to those in one of the largest cohorts studied (2002 runners) by Taunton et al.23 Consistent with these authors, the majority of injuries (65.3%) in our study were located from the knee distally. However, in Taunton et al's study, the knee was the most common site for injuries, compared with the foot and ankle noted in our study. The types of injuries were also similar to those in their study. Our distribution was skewed towards musculotendon and stress fracture/syndrome injuries compared with patellofemoral pain and iliotibial band syndrome reported by Taunton et al.23 However, a recent systematic review by Lopes et al24 revealed that injuries with the highest prevalence were medial tibial stress syndrome, Achilles tendinitis and plantar fasciitis. These injuries closely match the top two locations of injuries of the foot/ankle and lower leg found in our study.
Impact loading
As hypothesised, impact loading was greatest in the injured runners seeking medical attention and lowest in the never-injured group. As the strongest risk factor for an injury is a previous injury,21 we also compared the never-injured group to the subset of those in the medically diagnosed group who had not been previously injured. Impact variables were still higher in the injured group. This appears to suggest that the presence of a previous injury in this group did not influence these results. It would have been interesting to assess impact loading of those with recurrent injuries. Unfortunately, we were not able to determine if an injury reported for multiple months in a row were separate recurrences of the injury, or a single injury that had not resolved.
Load rates have been associated with injuries for some time. Along with studies by Radin et al9 ,10 in the 1970s, Burr et al25 also noted that rabbits experienced tibiae stress fractures when they underwent repetitive, impulsive loading. This is not surprising as our entire musculoskeletal system is comprised of viscoelastic structures that are sensitive to rates of loading. These high load rates occur early in stance during the eccentric phase of muscular activity. These muscles are lengthening under load during this time and help to attenuate the forces of impact. Therefore, it might be speculated that greater rates of loading of force might increase the strain rate experienced by the muscles as well, further exposing them to injury.
Despite the fact that the magnitude of FV is twice the magnitude of the impact peak, FV was not an important predictor of who went on to develop an injury. Additionally, the FV has not, to date, differentiated between injured and uninjured runners. This may be because FV is preceded by a more gradual rise in the force, or lower rate of loading. This was further supported by the systematic review of Zadpoor and Nikooyan,26 who concluded that peak forces may be less important than rate of loading in the development of tibial stress fractures in runners.
Study importance
This study's uniqueness is underscored by the fact that comparisons of injured runners were made to runners who had never been injured. Gaining insight into the mechanics of this understudied group further enhances our understanding of how to remain injury free. The importance of this work is further increased by the fact that all types of running injuries were included in the analysis. On average, vertical impact loading was increased in those who developed any running injury requiring medical attention. On further analysis, it appears that bony and soft tissue injuries were associated with high-impact loading. This is further supported by the association of high impacts in runners with tibial stress fractures (bony) as well as plantar fasciitis (soft tissue). Interestingly, iliotibial band syndrome was not associated with the highest values of any of the force variables, suggesting that it may be more strongly associated with malalignment as suggested by Noehren et al27 and Ferber et al.28 While it is clearly recognised that running injuries may have many mechanical causes, these results suggest that vertical impact loading may be one important global indicator for the development of an injury.
While a number of biomechanical variables were significantly greater in the DX_INJ group, VALR was the most important variable in predicting the development of an injury. Mileage was also greater in the injured group, but it, also, was not the most important variable in predicting injury. It has been reported that running over 40 miles/week is a significant risk factor for running injuries in men, but not women.29 Additionally, the mean mileage in the DX_INJ group was 25% below the reported criterion value. Therefore, based on these results, reducing load rates associated with impacts is likely to result in the most effective means of reducing injury risk. Based on previous reports, adopting a mid-foot or forefoot strike pattern will significantly reduce these impacts and rates of loading.3 ,6 Adopting these changes in footstrike patterns have been shown to mitigate injuries in runners. For example, Diebal et al30 demonstrated that slowly transitioning runners with anterior compartment syndrome from a rearfoot strike to forefoot striker pattern completely relieved their symptoms. Additionally, they reduced their intracompartmental pressures to normal, allowing them to resume their preinjury running levels. In a case series of runners with chronic anterior knee pain, Cheung et al31 demonstrated a resolution of pain and improvement in function following a gait retraining programme to transition them from rearfoot to slight forefoot strikers. To further support the benefit of a forefoot strike pattern, a recent retrospective study of the Harvard track team revealed that forefoot strikers were injured at about half the rate of their rearfoot counterparts.32 However, prospective studies of injury patterns in mid-foot and forefoot strike runners are clearly needed to further validate these findings.
In summary, the results of this study imply that an increase in impact loading in rearfoot strike runners amplifies the risk of developing a running-related injury requiring medical attention. Additional studies examining the effect of reducing these impacts, through transitioning to a mid-foot/forefoot strike pattern, on running injuries are underway.
What are the findings?
This is the first prospective study to indicate that runners who land ‘hard’, with increased, vertical impact peaks and vertical load rates, have an increased risk for injuries requiring medical attention.
Increased impacts at landing increased the risk of bony and soft tissue injuries.
Runners who have never been injured had the lowest impact loading of all studied groups.
Vertical average loading rate was the strongest predictor of injury risk.
How might it impact on clinical practice in the future?
These prospective data suggest that runners in our clinics who present with hard landings should be considered at increased risk for running-related injuries.
Reducing vertical impact loading in these runners may result in a reduction of running-related injuries.
Gait retraining interventions, such as focusing on transitioning to a forefoot strike pattern, has been previously shown to reduce injuries in runners and should be considered as a treatment for impact-related running injuries.
Acknowledgments
The authors thank our volunteer runners whose compliance in the 2-year follow-up stage of this study was critical to this work. The authors also thank Reed Ferber and Clare Milner who oversaw the majority of the collection of these data.
References
Footnotes
Correction notice This paper has been amended since it was published Online First. The first word of the title has been changed from “Reduced” to “Greater”. Also, in the Abstract, Conclusion the wording has been changed from “We found a VALR...” to “Vertical average loading rate was lower...”
Twitter Follow Irene Davis at @IreneSDavis
Contributors ISD was involved in the development of the research design and oversaw the entire research project. She is primarily responsible for the writing of the manuscript. BJB was involved in the analysis of the data and was involved in the writing and final approval of the manuscript. DRM was involved in the statistical analysis of the data and was involved in the writing and final approval of the manuscript.
Funding US Department of Defense grant DAMD17-00-1-0515.
Competing interests None declared.
Ethics approval University of Delaware.
Provenance and peer review Not commissioned; externally peer reviewed.