Article Text

Abstract
Objectives Various definitions for concussion have been proposed, each having its strengths and weaknesses. We reviewed and compared current definitions and identified criteria necessary for an operational definition of sports-related concussion (SRC) in preparation of the 5th Concussion Consensus Conference (Berlin, Germany). We also assessed the role of biomechanical studies in informing an operational definition of SRC.
Design This is a systematic literature review.
Data sources Data sources include MEDLINE, Embase, Cumulative Index to Nursing and Allied Health Literature, Cochrane Central Register of Clinical Trials and SPORT Discus (accessed 14 September 2016).
Eligibility criteria for selecting studies Eligibility criteria were studies reporting (clinical) criteria for diagnosing SRC and studies containing SRC impact data.
Results Out of 1601 articles screened, 36 studies were included (2.2%), 14 reported on criteria for SRC definitions and 22 on biomechanical aspects of concussions. Six different operational definitions focusing on clinical findings and their dynamics were identified. Biomechanical studies were obtained almost exclusively on American football players. Angular and linear head accelerations linked to clinically confirmed concussions demonstrated considerable individual variation.
Summary/conclusions SRC is a traumatic brain injury that is defined as a complex pathophysiological process affecting the brain, induced by biomechanical forces with several common features that help define its nature. Limitations identified include that the current criteria for diagnosing SRC are clinically oriented and that there is no gold/standard to assess their diagnostic properties. A future, more valid definition of SRC would better identify concussed players by demonstrating high predictive positive/negative values. Currently, the use of helmet-based systems to study the biomechanics of SRC is limited to few collision sports. New approaches need to be developed to provide objective markers for SRC.
- head injury
- definition
- sports
- systematic review
- biomechanics.
Statistics from Altmetric.com
Introduction
Sports-related concussion (SRC) is a well-recognised clinical entity. However, its pathophysiological basis remains poorly understood. In the broadest clinical sense, concussion is often defined as representing the immediate and transient symptoms of a mild traumatic brain injury (mTBI). Such operational definitions, however, do not give any insights into the underlying processes through which the brain is impaired, nor do they distinguish different grades of severity, nor reflect insights into the persistence of symptoms and/or abnormalities on specific investigational modalities.
Since the 1970s, clinicians and scientists have begun to distinguish SRC from other causes of concussion and mTBI, such as seen in motor vehicle crashes, etc. Although this seems like an arbitrary separation from other forms of TBI,1 2 it is largely driven by sporting bodies who see the need to have clear and practical guidelines to determine recovery and safe return to play for athletes suffering from SRC. In addition, sports participation can be viewed as research laboratories to study SRC and mTBI, given the detailed SRC phenotype data that are typically available in many sports.3 Having said that, it is critical to understand that the lessons derived from non-sporting mTBI research informs the understanding of SRC (and vice versa), and this arbitrary separation of sporting versus non-sporting TBI should not be viewed simply as a dichotomous or exclusive view of TBI.
Over the past 50 years, various definitions of concussion and mTBI have been proposed by individual authors, different research groups and international bodies. These definitions, however, do not necessarily concur with one another, although there are a number of common elements. The definitional differences make the understanding of injury epidemiology problematic and management challenging.4
This systematic review offers an overview of previous concussion definitions and on the role of biomechanical studies in this context. These were specific review questions given to this writing group by the Concussion in Sport Group (CISG). It aims at providing an updated operational definition of concussion and is part of a series of articles written in preparation of the 5th Concussion Consensus Conference held in October 2016 in Berlin, Germany.
Historical perspective
The clinical manifestations of concussion as a transient neurological syndrome due to head shaking (or ‘commotion’) without structural brain injury have been known since the 10th century AD, when the Persian physician, Rhazes, first defined the condition.5–7 Following pioneering experimental primate studies demonstrating the transient and functional nature of concussion, the term acceleration concussion was proposed as the generic descriptor that should be applied to all forms of traumatic brain injury.8 Implicit in this concept is that the term concussion should be synonymous with traumatic brain injury of all severities. A variation on this view holds that concussion refers to the mechanism of injury and motion of the brain within the skull rather than any clinical symptoms or pathology.9
Dating back to the 1930s, numerous anecdotal concussion severity-grading scales have been published reflecting the variety of prevailing theories in existence at the time.10 11 By 2001, there were approximately 45 published scales, none of which had been scientifically validated.12 13 Although not defining concussion per se, these scales broadly attempted to separate arbitrary levels of concussion severity based on clinical symptoms that would, in turn, inform management and return to play advice. These scales have been reviewed in detail elsewhere; however, it was the view of the CISG in 2001 that these should be abandoned and clinical measures of assessment and recovery be utilised to determine safe return to play.12
What do biomechanics tell us about the definition of SRC?
Studies examining biomechanics and head injury (including TBI) demonstrate broadly that impacts causing SRC are less severe than impacts causing cranial fractures, intracranial haemorrhages and diffuse axonal injury.14–18
Biomechanical studies of concussion demonstrate both differential effects on brain regions depending on the impact force, site of impact and bony architecture of the skull, as well as considerable intrinsic variation in tolerance to head impacts, which will depend on energy status and previous concussion and could be speculated to have a genetic basis also.19
Recent studies on SRC have reported head impact exposure patterns for specific sports, for example, American football, ice hockey and Australian football. Those studies report head impact characteristics including frequency, head kinematics, head impact location and injury outcome. To quantify head impacts, studies have used helmet-based systems, mouthguard/headband/skin sensors as well as videometric studies. The measured or estimated head kinematics provide a starting point to understanding brain tissue loading. Studies have aimed at identifying concussion thresholds for head acceleration (linear and angular).18 Within these studies, the use of instrumented helmets has provided information on head impact exposures, although there remains some debate regarding the accuracy and precision of these head kinematic measurements.
Biomechanical modelling demonstrates that brain loading patterns (stresses and strains) are not uniformly distributed due to factors including the brain geometry, brain tissue properties, bony architecture of the internal skull and connective tissue, for example, falx cerebri and tentorium cerebelli. This means that certain anatomical areas will have greater or lesser physiological or biochemical disturbance depending on the interplay of the external forces, the head’s overall kinematic responses and brain sensitivity, such that resultant clinical symptoms may vary from person to person.20–23
To which extent such measurements of head kinematic responses, for example, linear and angular head acceleration, may influence a definition of concussion has not been determined, and a complete biomechanical understanding of these injuries and related modelling to predict SRC remains a work in progress.24
Aims of the review
The aim of this review was to perform a systematic review of the literature as per the CISG protocol25 and specifically addresses the following two questions:
What are the critical clinical criteria for an operational definition of SRC?
Do the published biomechanical studies inform us about the definition of SRC?
As per the CISG process, the systematic review was presented at the 5th Concussion Consensus Conference in Berlin, Germany. The updated definition of SRC was developed from the literature review and informed by public discussions and was finalised by the scientific committee.
Materials and methods
The overall methodology of the CISG systematic review process has been outlined in a separate paper published accompanying this review.25
Data sources and searches
A literature search (MEDLINE, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Clinical Trials (CRCT) and SPORTDiscus) was performed (14 September 2016) to identify English-language articles reporting on clinical criteria of a definition of SRC (aim 1) or on original data of the biomechanics of SRC in humans (aim 2). The MEDLINE (OVID) search strategy was translated for each database and is reported in online supplementary file 1.
Supplementary file 1
Note that for aim 1 we only included manuscripts that made a significant contribution to the diagnostic criteria for SRC, that is, modified existing diagnostic criteria or presented new criteria. Manuscripts that referred to, discussed or compared existing definitions of SRC were not eligible. Whereas for aim 1 consensus papers and reviews were also considered, original contributions containing data on players with clinically confirmed SRC were eligible only for aim 2. The role of biomarkers in concussion was addressed in a separate review in this issue and therefore is not further investigated here.
A manual search of reference lists from eligible articles was performed. We did not seek to identify research abstracts from meeting proceedings or unpublished studies. Studies with five or more participants were eligible for aim 2. This review complies with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.26
Study selection
All identified articles were subject to title and abstract screening by two independent reviewers (AAT and NFD). Full-text screening was applied to all abstracts considered eligible by at least one reviewer. Articles were selected using predetermined criteria (for exclusion criteria, see online supplementary file 1). Discrepancies in selection status and reasons for exclusion were settled between the two reviewers by discussion and adjunction of a third reviewer (JD) if needed.
Data extraction and data synthesis
Data extraction was performed by AAT and confirmed by NFD. For aim 1, we extracted the key components of the concussion definition and how the definition was established. Data synthesis in these studies focused on the description of predefined key features (symptom onset and duration, mechanism, loss of consciousness (LOC), resolution of symptoms and neuroimaging), on the distinction between concussion and mTBI, and on the number of citations. In studies reporting on biomechanical aspects of SRC (aim 2), we extracted key aspects such as the investigated sports, recording devices used, acceleration values resulting in a concussion and concussion location, and determined the distribution of mean linear and rotational acceleration values and the mean (±1 SD) distribution of head impact location among studies.
Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) assessment of included studies
For included studies reporting original data on the biomechanics of concussion (aim 2), the risk of bias and applicability concerns were assessed by one reviewer (AAT). A second reviewer (NFD) confirmed ratings, and disagreements were resolved by discussion. We opted for the QUADAS-2 tailored study criteria, as they are widely used and recommended for the assessment of diagnostic accuracy studies.27 We did not restrict inclusion further based on QUADAS-2 results. Note that we did not apply QUADAS-2 to consensus/statement papers providing definitions of concussion (aim 1), as this was not appropriate for this sort of publications.
The QUADAS-2 tool consists of four core domains (patient selection, index test, reference standard and flow/timing).27 Risk of bias is assessed for all four domains, and applicability is assessed for the first three domains. Thus, seven items per study are assessed. For each item the risk of bias is identified as ‘high’, ‘low’ or ‘unclear’.
Results
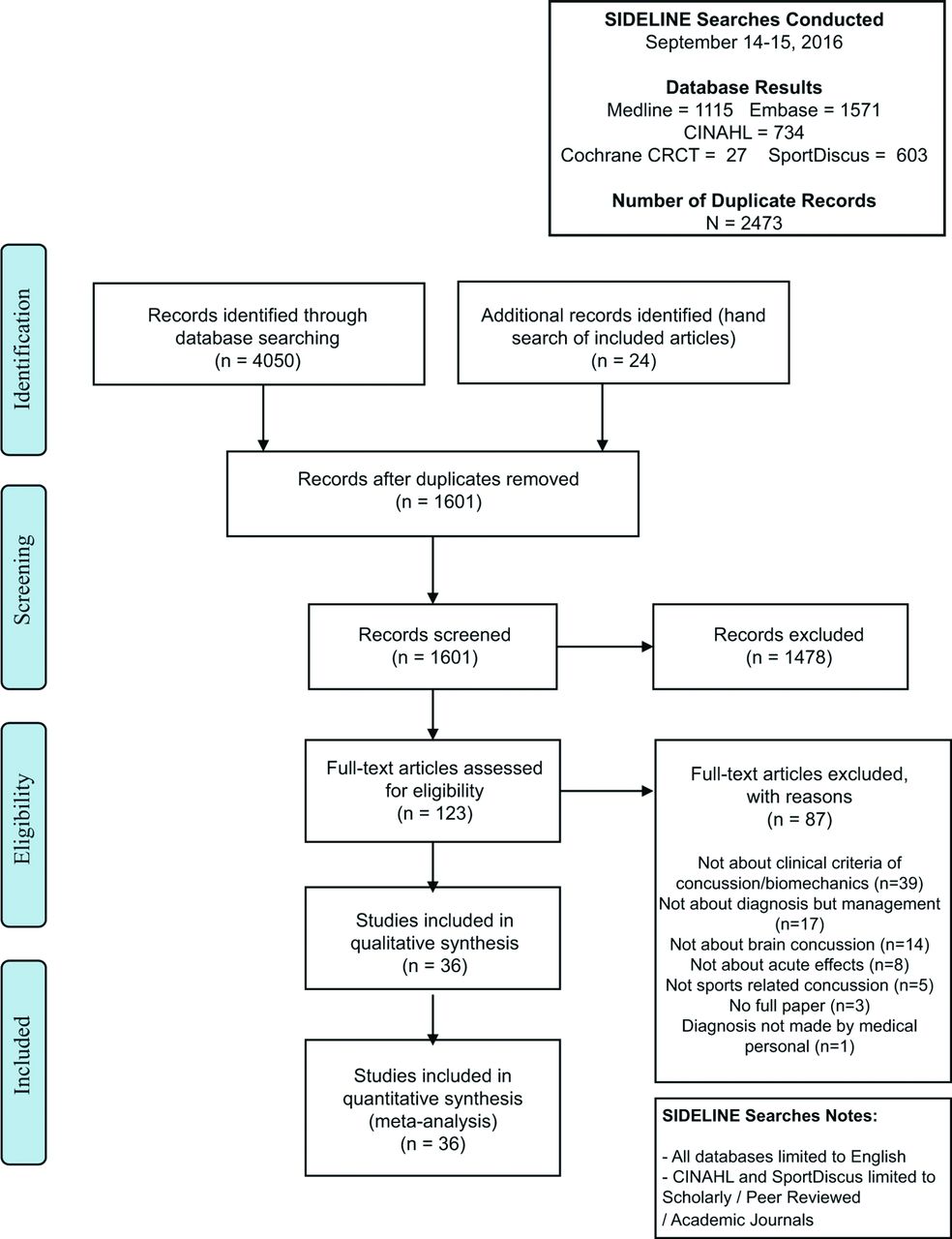
We identified 1601 citations for title/abstract screening and 123 articles for full-text screening. Eventually, 36 (2.2%) studies were included for quantitative synthesis (figure 1). Among the 36 studies included, we identified 14 manuscripts defining the term concussion according to our selection criteria (aim 1), whereas 22 manuscripts reported on biomechanical aspects of SRC (aim 2).
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart.
Aim 1: Studies reporting on concussion definitions
From the 14 manuscripts focusing on defining the term concussion (table 1), 12 studies from 6 different organisations (CISG, American Medical Society for Sports Medicine (AMSSM), National Athletic Trainers’ Association (NATA), American Academy of Neurology (AAN), Team Physician Consensus Group (joint statement by the American Academy of Family Physicians, the American Academy of Orthopaedic Surgeons, the American College of Sports Medicine, the AMSSM, the American Orthopaedic Society for Sports Medicine, and the American Osteopathic Academy of Sports Medicine) and Committee on Head Injury Nomenclature From the Congress of Neurological Surgeons) provided consensus-based operational definitions of concussion.12 28–37 One study provided original data on the implementation of a structured concussion assessment in a paediatric emergency department,38 and one study reviewed definitions of concussion as provided on websites.39
Overview of included studies providing definitions of concussion*
Comparison of the different consensus-based operational definitions identified
Key aspects of the six definitions included are provided in table 2. Although all but one definition37 were proposed or revised within the last 5 years and were restricted to SRC, they differed in the level of detail and the domains addressed.
Key components for identifying a concussion—comparison of different definitions*
Comparing the key elements characterising a concussion in the proposed consensus-based definitions showed both similarities and discrepancies for some items (table 2). Whereas in all definitions loss of consciousness (LOC) was considered optional for making the diagnosis, onset (immediate/rapid/within minutes), duration, mechanism of impairment and resolution were addressed only by some of the definitions (table 2).
The assessment of specific domains was described in four definitions. Clinical symptoms typically included physical, cognitive, emotional and sleep disturbances, whereas examination included physical signs and neurocognitive testing (for cognitive and neurobehavioural alterations). A statement regarding typical findings on standard structural neuroimaging was provided only by two groups (CISG and Team Physician Consensus).
The terms ‘concussion’ and ‘mTBI’ were handled differently in these consensus statements.30–33 36 Whereas concussion was considered a subset of TBI (CISG)30 or mTBI (AMSSM),31 concussion and mTBI were used synonymously by others (Team Physician Consensus statement, AAN consensus and NATA).32 33 36
Aim 2: Studies reporting on biomechanical aspects of concussion
Twenty-two manuscripts reporting on biomechanical aspects of SRC met our inclusion criteria. From two studies, the results were reported in more than one paper. For each study we considered only the most recent publication40 41 and did not include the others.22 24 42 From the remaining 19 manuscripts, key aspects were extracted (tables 3 and 4).
Overview of included original publications reporting on biomechanical aspects of concussion*
Key aspects of studies reporting on the biomechanics of concussion (only studies using HITS)
Risk of bias assessment (QUADAS-2)
Risk of bias and applicability concerns for patient selection were rated as ‘high’ in six studies as only a subset of identified concussions were included (online supplementary file 2). For index testing, all studies were considered ‘high’ risk of bias as the biomechanical data were analysed and interpreted with the knowledge of the results from the reference test. Eleven studies that were either directly funded by or had one/several co-author(s) who had a vested financial interest in the accelerometry system used were rated as ‘high’ risk for applicability concerns of the index test. Regarding the reference standard, we considered all 22 studies as ‘unclear’ risk of bias, as it remains unknown if all concussions were identified by the medical staff.
Supplementary file 2
Key findings of included studies
To quantify head impacts, 17/19 studies used helmet-based systems. The Head Impact Telemetry System (HITS) was used in 15 studies and instrumented mouthguards with 6 degrees-of-freedom (DOF) sensors were used in 2 studies. Video analysis was applied to a study cohort of rugby and Australian rules football players,21 providing more detailed analysis on a subset of players in a follow-up study.41 Different combinations of parameters were assessed in these studies. The methods by which concussions were diagnosed remained unclear in five studies, and only five studies adhered to published concussion consensus definitions.
The measured mean peak linear accelerations in concussed players (data from 13/15 studies using the HITS) ranged between 43.0 and 145.0 g. In between these boundaries, most studies reported mean peak linear acceleration values of approximately 100 g. For rotational acceleration, the mean peak values (n=9 studies) in concussed players ranged between 3620 and 7230 rad/s2 (table 4). Results from studies using instrumented mouthguards or video-based analyses demonstrated a similar range for peak linear accelerations, whereas peak rotational accelerations tended to be higher (table 4).
Eight HITS-based studies in American football players (and ice hockey players in one of those studies) reported the location of head impacts (n=308), with frontal impacts identified most frequently (n=151; 49%). In a single study on head impact location in Australian rules football and rugby based on video analysis,21 69% of the impacts were located on the side of the head. In a follow-up study including non-injured athletes, the proportion of impacts to the temporal region was significantly greater (p=0.05) for concussion cases compared with no-injury cases, 60% and 23%, respectively.41 It is important to recognise that structural TBI or cranial fractures did not occur in these studies, and the vast majority of head impacts recorded with the HIT system did not result in concussion; for example, approximately 0.02% of the impacts in Broglio et al 43 were associated with a diagnosis of concussion.
In summary, the reported peak linear and rotational acceleration values in players with clinically confirmed concussion showed large inter-individual variability, and cut-off values were proposed in a single study only. Noteworthy, all studies had a high risk of bias and a high risk for applicability concerns for at least one item, warranting caution in interpreting these studies.
Discussion
Our review identified six consensus-based definitions of SRC. Among the different organisations providing definitions, the consensus statements from the CISG were cited most frequently (with 1376 citations in Google Scholar for the 2009 consensus statement), followed by the statements from AAN, NATA and AMSSM (all around 500–700 citations) (table 5). Because the 1966 Statement of the Congress of Neurological Surgeons was issued prior to the recent popularity of this topic, the number of citations for this document must be interpreted with caution.
Number of citations for individual studies
On the basis of the highest number of citations, the consensus statements from the CISG can be considered the opinion leader, although it is acknowledged that earlier definitions largely predate the era of internet citations.12 28–30 These consensus-based definitions showed different levels of detail and weighted distinct domains differently. We demonstrated limitations even in those definitions that provided additional clarifying statements.30 36
Recommendations for a future operational definition of SRC
On the basis of this systematic review and consensus discussions, it is recommended that the key elements of a future clinical or operational definition of SRC ideally include some or all of the following elements:
Biomechanics—the injury is caused by quantified direct or indirect force(s) to the brain;
Physiology—a defined physiological disruption of brain function;
Clinical—a range of evolving clinical symptoms and signs including an alteration in cognitive functioning or mental state (eg, confusion, disorientation, slowed thinking) that may or may not involve transient LOC;
Neuroimaging—a defined abnormality on advanced imaging platforms reflecting the underlying physiological abnormalities and clinical features;
Fluid biomarkers and genetics—defined abnormalities reflecting the underlying physiological disruption or injury.
Despite many publications and definitional attempts, these considerations leave several issues unanswered; notably, does being dazed, seeing stars or feeling dizzy in the absence of altered mental state constitute either concussion or mTBI? The definition also does not explain how known concussion modifiers influence the clinical presentation.
Berlin consensus definition of SRCs
The 2016 Berlin Consensus Conference operational definition (‘Berlin definition’) is presented below. This definition is based on the systematic review of the literature presented here, as well as the consensus discussions during the plenary session by the conference participants and the expert panel.
Concussion is a traumatic brain injury induced by biomechanical forces. Several common features that may be used in clinically defining the nature of a concussive head injury include the following:
Concussion may be caused either by a direct blow to the head, face, neck or elsewhere on the body with an impulsive force transmitted to the head.
Concussion typically results in the rapid onset of short-lived impairment of neurological function that resolves spontaneously. However, in some cases, signs and symptoms evolve over a number of minutes to hours.
Concussion may result in neuropathological changes, but the acute clinical signs and symptoms largely reflect a functional disturbance rather than a structural injury and, as such, no abnormality is seen on standard structural neuroimaging studies.
Concussion results in a range of clinical signs and symptoms that may or may not involve LOC. Resolution of the clinical and cognitive features typically follows a sequential course. However, in some cases symptoms may be prolonged.
The clinical signs and symptoms of concussion cannot be explained by drug, alcohol, medication use, other injuries (such as cervical injuries, peripheral vestibular dysfunction, etc) or other comorbidities (eg, psychological factors or coexisting medical conditions).
Limitations and outlook
Our systematic review may have a potential publication bias and language bias as only published, English-language articles were considered. It is important to note that even if a healthcare professional is ‘skilled’, what reproducible and valid criteria do they use to make this ‘diagnosis’ of SRC? Thus, the major challenges in concussion diagnosis are the following:
There is no gold or reference standard measure of concussion.
There is marked variability in the diagnostic criteria, with no studies examining the measurement properties of the definitional criteria.
Given 1 and 2, there is likely a large amount of information bias inherent in all concussion studies because there is no validated case definition. Thus, information bias would be present in studies of risk, prevention, prognosis, intervention and long-term sequelae. This likely explains some of the variability of findings in these areas.
The challenge is to validate an operational definition of SRC based on clinical criteria until a ‘proven’ gold standard is discovered and validated. This is highlighted as a major area of research for the reasons outlined above. If an objective gold standard becomes available, the clinical criteria could then be tested against it to provide diagnostic metrics such as positive and negative predictive values and likelihood ratios. Another approach in the absence of an objective gold standard is to use the prognostic utility of a concussion definition. If it accurately predicts outcome, it could be a useful measure to identify and triage cases. Such a prediction rule would be more useful than a diagnosis based on unknown criteria.44
Currently, the investigation of biomechanical aspects of SRC focuses on high school/college collision sports where players wear helmets. In these studies peak linear acceleration values in concussed players averaged approximately 100 g. This is in good agreement with a recent systematic review.18 These impacts are less severe than head impacts resulting in structural head injury, for example, intracranial haemorrhages or contusions, diffuse axonal injury, and cranial fractures.15–17 45 Methodological limitations in these studies must be considered, such as helmet fit, not using consensus-based concussion definitions and not reporting whether the diagnosis was made by skilled medical personal or not. Furthermore, lack of duplicate risk of bias assessment in our systematic review should be considered as a limitation. Developments are occurring in mini-accelerometer devices that can be worn by athletes who do not wear a helmet. These devices offer opportunities for research and clinical practice. At present, there is no evidence that accelerometer devices or video-based observations of athletes can provide a 'diagnosis’ of concussion. Therefore, at present, head acceleration data should not be used in isolation to remove a player from play or allow a player to keep playing following a hit.
Conclusions
With regard to both aims addressed in this systematic review, newer technological advances may give important insights into the underlying pathophysiology and ultimately provide a platform to develop a clear definition in the future. It can be anticipated that, in the future, head injury and concussion may eventually be defined by the severity of clinical signs, as well as genetic, epigenetic, metabolomic, proteomic, advanced imaging findings and blood/cerebrospinal-fluid biomarkers.
What is already known?
Over the past 50 years, various definitions of sports-related concussion (SRC) and mild traumatic brain injury (mTBI) have been proposed by individual authors, different research groups and international bodies.
Currently, there is no gold or reference standard for SRC diagnosis, and the diagnostic properties of the various definitions have not been studied.
The different definitions of SRC do not concur with one another, and this variability has likely caused information or diagnostic misclassification bias in past studies on the management and prognosis of SRC.
What are the findings?
Among currently available consensus-based definitions of SRC, the consensus statement from the Concussion in Sport Group can be considered the opinion leader based on citation statistics.
These consensus-based definitions, however, showed different levels of detail and weighted distinct domains differently. Limitations even in those definitions that provided additional clarifying statements were demonstrated, including the overlap/distinction between SRC and mTBI.
Angular and linear head accelerations linked to clinically confirmed SRC demonstrated considerable individual variation.
The 2016 Berlin Consensus Conference operational definition (‘Berlin definition’) is presented.
References
Footnotes
Contributors PM conceived the study, drafted and critically reviewed the manuscript, and approved the final version of the manuscript.
NF-D performed the literature search, reviewed identified manuscripts and selected those matching inclusion criteria, edited and critically reviewed the manuscript, and approved the final version of the manuscript.
JD conceived the study, edited and critically reviewed the manuscript, and approved the final version of the manuscript. J
DC edited and critically reviewed the manuscript and approved the final version of the manuscript.
AM edited and critically reviewed the manuscript and approved the final version of the manuscript.
PEV edited and critically reviewed the manuscript and approved the final version of the manuscript.
RJE edited and critically reviewed the manuscript and approved the final version of the manuscript.
WM conceived the study, edited and critically reviewed the manuscript, and approved the final version of the manuscript.
AAT performed the literature search, reviewed identified manuscripts and selected those matching inclusion criteria, performed the statistical analysis, drafted and critically reviewed the manuscript, and approved the final version of the manuscript.
Competing interests PM is a co-investigator, collaborator or consultant on grants relating to mild TBI funded by several governmental organisations. He is directly employed by the National Health and Medical Research Council of Australia and is based at the Florey Institute of Neuroscience and Mental Health. He is co-chair of the Australian Centre for Research into Sports Injury and its Prevention (ACRISP), which is one of the International University Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee (IOC). He is co-chair of the International Concussion in Sport Group. He has a clinical and consulting practice in general and sports neurology. He receives book royalties from McGraw-Hill and was employed in an editorial capacity by the British Medical Journal Publishing Group from 2001 to 2008. He has been reimbursed by the government, professional scientific bodies and sporting bodies for travel costs related to presenting research on mild TBI and sports-related concussion at meetings, scientific conferences and symposiums. He received consultancy fees in 2010 from Axon Sports (USA) for the development of educational material (which was not renewed) and has received research funding since 2001 from CogState Inc. He has not received any research funding, salary or other monies from the Australian Football League, FIFA or the National Football League. The Australian Football League funds research at the Florey Institute under a legal memorandum and PM does not receive any money from this industry-funded research. PM is a cofounder and shareholder in two biomedical companies (involved in eHealth and compression garment technologies) but does not hold any individual shares in any company related to concussion or brain injury assessment or technology. He did not receive any form of financial support directly related to this manuscript. NF-D and JD report no conflicts of interest. AM is a self-employed consultant and holds honorary academic appointments. He has been funded as a consultant to undertake research and policy related work for government, sports federations and industry on the topic of safety and injury risk management, including concussion, head injury and helmets. He did not receive any form of financial support directly related to this manuscript. He reports no conflicts of interest. PEV is a neurologist and Chairman of the Steering Commitee of a trial in traumatic brain injury sponsored by EVER Neuro Pharma GmbH. He has been funded as a consultant for EVER Neuro Pharma. He did not receive any form of financial support directly related to this manuscript. He reports no conflicts of interest. JDC is an injury epidemiologist employed by the University Health Network, University of Toronto. He is a professor in the Division of Epidemiology and the Institute of Health Policy, Management and Evaluation at the Dalla Lana School of Public Health, University of Toronto. He has received funding from the Ontario Neurotrauma Foundation to undertake systematic reviews on mild traumatic brain injury and served on the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury, which received funding from various sources, including traffic insurance companies in North America and Europe. He was retained as an expert witness for the National Hockey League on November 30, 2016. He did not receive any form of financial support related to this manuscript, and has no other conflicts of interest to report. RJE is a consultant to the National Hockey League, Major League Soccer, US Soccer Federation and Princeton University. He receives financial remuneration for these consulting relationships. He has a clinical practice in sport neuropsychology and serves as an expert (neuropsychology and sport neuropsychology) in medico-legal cases involving traumatic brain injury. WM is the Medical Director of the National Hockey League. He has received research grant support through the University of Calgary from the Canadian Institutes of Health Research, Alberta Innovates Health Solutions, the International Football Association (FIFA), Alberta Children’s Hospital Research Institute and the Hotchkiss Brain Institute. He is the founding Chair of the Sport Injury Prevention Research Centre, which is one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee (IOC). He has a clinical consulting practice in sport medicine at the University of Calgary Sport Medicine Centre. He is an Expert Group member of the IOC Medical Commission and has received travel funding in that capacity.
Provenance and peer review Not commissioned; externally peer reviewed.