Article Text

Abstract
Design Single-blind randomised clinical trial.
Objective To compare the effects of three 8-week rehabilitation programmes on symptoms and functional limitations of runners with patellofemoral pain (PFP).
Methods Sixty-nine runners with PFP were randomly assigned to one of three intervention groups: (1) education on symptoms management and training modifications (education); (2) exercise programme in addition to education (exercises); (3) gait retraining in addition to education (gait retraining). Symptoms and functional limitations were assessed at baseline (T0), and after 4, 8 and 20 weeks (T4, T8 and T20) using the Knee Outcome Survey of the Activities of Daily Living Scale (KOS-ADLS) and visual analogue scales (VASs) for usual pain, worst pain and pain during running. Lower limb kinematics and kinetics during running, and isometric strength were also evaluated at T0 and T8. The effects of rehabilitation programmes were assessed using two-way analysis of variance.
Results No significant group × time interactions (p<0.447) were found for KOS-ADLS and VASs. All three groups showed similar improvements at T4, T8 and T20 compared with T0 (p<0.05). Only the exercises group increased knee extension strength following rehabilitation (group × time: p<0.001) and only the gait retraining group (group × time: p<0.001) increased step rate (+7.0%) and decreased average vertical loading rate (−25.4%).
Conclusion Even though gait retraining and exercises improved their targeted mechanisms, their addition to education did not provide additional benefits on symptoms and functional limitations. Appropriate education on symptoms and management of training loads should be included as a primary component of treatment in runners with PFP.
Trial registration number ClinicalTrials.gov (NCT02352909).
- Knee pain
- Running
- Exercise
Statistics from Altmetric.com
Background
Recreational running is a popular activity known to provide significant physiological1 2 and psychological3 4 health benefits. However, up to 79% of runners develop running-related injuries.5 Patellofemoral pain (PFP) ranks among the most common conditions,6 and is defined as pain around or behind the patella aggravated by activities that load the patellofemoral joint (PFJ).7
Education on managing training loads has long been suggested as a main component for treating PFP,8–10 and the latest international consensus statement recommended that research on education interventions be conducted.11 Specifically in runners, PFP is often observed following recent increases in running mileage or speed.12 13 Thus, education on how to avoid training loads that exceed the zone of tissues’ capacity to adapt is likely to contribute to treatment outcomes.14
Exercises have also been advocated to alleviate symptoms and functional limitations of individuals with PFP,11 15 and systematic reviews specifically highlighted the benefits of combining exercises targeting proximal and quadriceps strengthening.16 17 Such exercises are likely to help runners with PFP in sustaining repeated lower limb impacts. While mechanisms leading to such clinical success remain unclear, exercises could potentially increase tissues’ capacity to sustain mechanical load, thus improving long-term outcomes.18
Gait retraining represents another research focus in runners with PFP and aims at modulating forces acting on the PFJ.19 It has been suggested that transitioning from a rearfoot to a forefoot strike pattern can help decrease symptoms and increase functional scores.20 21 In addition, several studies have suggested that increasing step rate can reduce PFJ reaction forces.22–24 Thus, modifications in step rate and foot strike pattern may represent valuable interventions in runners with PFP.
Multimodal interventions are recommended to reduce pain in adults with PFP.11 Yet, the relative contribution of treatment components to clinical outcomes needs to be explored to optimise clinical management. To date, no study has compared different rehabilitation approaches in runners with PFP. The objective of this randomised clinical trial (RCT) was to compare the effects of three rehabilitation programmes (education, education and exercises, and education and gait retraining) on symptoms and functional limitations of runners with PFP. The programmes’ effects on isometric strength and running mechanics were also compared. We hypothesised that all three approaches would be efficient in decreasing symptoms and improving function, but that both the exercises and gait retraining groups would experience greater improvements than the education group, with faster improvements in the gait retraining group secondary to decreased PFJ forces during running. This RCT was registered on ClinicalTrials.gov (NCT02352909) and the study protocol has been published.25
Methods
Participants
Participants were recruited using advertisements within the running community of Quebec City. They had to: (1) be aged 18 to 45 years; (2) report a minimal weekly running distance of 15 km; (3) present with PFP for at least 3 months; (4) experience minimum pain levels of 3/10 on a visual analogue scale (VAS) during running and during three tasks among stairs, kneeling, squatting and resisted knee extension7 and (5) score a maximum of 85/100 on the Knee Outcome Survey of the Activities of Daily Living Scale (KOS-ADLS; the primary outcome).26 Runners were excluded if they presented with: (1) symptoms onset following an acute trauma; (2) symptoms believed to originate from patellar tendon27 or menisci28; (3) concurrent lower limb injuries; (4) past history of patellar dislocation or lower limb surgery and (5) presence of rheumatoid, neurological or degenerative diseases. The Quebec Rehabilitation Institute research ethics committee approved the study.
Study design
A single-blind (evaluator only) parallel-group RCT was conducted. Evaluations were performed at baseline (T0) and at week 4 (T4), 8 (T8) and 20 (T20). At T0, data on demographics, symptomatology, running habits, isometric strength and running mechanics were collected at the research centre. Then, all participants attended five physiotherapy sessions (weeks 1, 2, 3, 5 and 7) in a private clinic during an 8-week period. Runners were allocated to either (1) an intervention that only included education on load management and training modifications according to symptoms (education); (2) the addition of an exercise programme to the education component (exercises); (3) the addition of gait retraining to the education component (gait retraining). Symptoms and functional limitations outcomes were assessed at all time points. Isometric strength and running mechanics were assessed at T0 and T8.
Randomisation and blinding
A scientist not involved in data collection generated randomisation lists using a random number generator (block randomisation; block size of 3–12). Randomisation was stratified according to sex (male/female) and foot strike pattern (rearfoot/non-rearfoot). Group allocations were concealed in sequentially numbered sealed opaque envelopes, which were opened by one member of the research team not involved in data collection following baseline assessment. Given the impossibility of blinding runners to their treatment allocation, precautions were taken to ensure they were unaware of the other treatment groups. Participants were instructed not to reveal the content of their programme to the evaluator. The same evaluator performed all assessments, and blinding was assessed using a question about group allocation following final assessment.
Interventions
Each runner took part in one of three rehabilitation programmes supervised by independent physiotherapists (n=6) who attended a standardisation session. Frequent reviews of protocols were made with clinicians throughout the study. Runners received written instructions pertaining to their assigned programme, and all components of the allocated programme were addressed at every physiotherapy session. Self-declared compliance to all received instructions (0%–100%; including training modifications, exercises and gait modifications) was evaluated after the programmes.
Education group: Runners received education on load management and were instructed to self-modify running training according to symptoms. They were asked to increase the frequency of their weekly trainings, to decrease each session’s duration and speed and to avoid downhill and stairs running. Run–walk intervals were allowed. Runners were instructed to maintain PFP level at no more than 2/10 during running. Furthermore, pain had to return to pretraining levels within 60 min post-training, without increases in symptoms the following morning. Individualised weekly programmes, which could be modified by runners depending on symptoms, were designed by the treating physiotherapists and progressed based on the evolution of symptoms. Gradually, running distance was increased according to symptoms, before adding speed and hills.29 This specific intervention was provided to all groups. The education group received no other instructions.
Exercises group: In addition to the education component, runners were asked to perform a standardised home exercise programme aimed at improving strength, capacity to sustain mechanical load and dynamic control of the lower limbs. The personalised programme included four phases of 2 weeks and gradually progressed through higher difficulty under physiotherapist guidance. Three to four exercises were performed three times per week (maximum 20 min/session), and one exercise (lower limb control) was performed daily (Supplementary file 1).
Gait retraining group: Together with education, runners received personalised advice on running gait modifications. Runners were asked to increase step rate by 7.5%–10%.22 30 If deemed necessary by the physiotherapist (no significant reduction of impact orrunner unable to increase step rate), runners were also asked to run softer31 and to adopt a non-rearfoot strike pattern.20 21 Participants had a 10-minute treadmill session with physiotherapist feedback at every visit to the clinic.
Outcomes
The French version of the KOS-ADLS (MDC90=8.3 points; MCID=13.6 points) was used as the primary outcome to evaluate symptoms and functional limitations experienced during daily activities.26 32 A score of 100% denotes the absence of symptoms and functional limitations. Knee pain was also assessed using visual analogue scales for usual pain (VAS-U), worst pain (VAS-W) and pain during running (VAS-R).33 Participants were provided with a global positioning system-enabled Garmin Forerunner 15 watch, which allowed to monitor weekly running mileage using an online platform (Garmin Connect).
Maximum voluntary isometric contractions were assessed for knee extensors and hip external rotators, abductors and extensors using a Medup handheld dynamometer (Atlas-Medic, Quebec City, Canada) as per validated methods.34 The peak force value (kilograms) from three trials was normalised to bodyweight.35 36
Mechanics of the affected limb during running were evaluated using kinetic and kinematic data. Rigid triads of retroreflective markers were placed bilaterally on the lateral part of the foot, shank and thigh, and on the lumbosacral and cervicothoracic junctions.37 Single markers were temporarily placed on specific anatomical landmarks for calibration.37 Kinematic data were collected at 200 Hz (VICON Motion Systems, California, USA). Following a 5-minute warm-up at preferred running speed between 8 and 10 km/h, kinetic data were collected during 3 min from the instrumented treadmill (Bertec, Columbus, Ohio, USA) at 1000 Hz and down sampled to synchronise with kinematic data. Using custom MatLab programs (MathWorks, Massachusetts, USA), marker trajectories and ground reaction forces were filtered using zero-lag fourth-order low-pass 12 and 30 Hz Butterworth filters, respectively. The stance phase was determined by a 20 N threshold of vertical ground reaction force. PFJ contact forces were estimated based on a previously reported algorithm38 that considers knee flexion angle, net knee extension moment and quadriceps moment arm.39 To calculate average PFJ loading rate and average vertical loading rate, the mean slope from 20% to 80% of the interval between foot strike and first force peak was considered.40
Sample size
Sample size was calculated based on expected changes in KOS-ADLS scores. Using a similar 8-week multimodal intervention, a previous study29 reported increases in KOS-ADLS scores from 71.7±12.9 to 89.5±11.9. Considering similar score changes in our primary outcome, α=0.05, power=90% and MCID=13.6%, 20 runners were needed in each group (G*Power 3.1.7). Adding an anticipated attrition rate of 15%, 23 runners per group were recruited.
Statistical analyses
Baseline demographic data were compared using one-way analysis of variance (ANOVA) and χ2 tests. Group comparisons were adjusted for confounding variables using an analysis of covariance (ANCOVA) model when baseline characteristics were different across groups. Intention-to-treat and per-protocol analyses were used for symptoms and function outcomes (KOS-ADLS, VASs and running mileage). To ensure appropriate insight on mechanisms underlying changes in symptoms and function, only runners who completed T8 evaluation were considered for isometric strength and running mechanics. Repeated-measures ANOVAs (group × time) were used to compare the effects of the rehabilitation programmes on primary and secondary outcomes, and effect sizes were reported (η2). Bonferroni adjustments for multiple comparisons were used for all outcomes; therefore, results showing p-values <0.017 (0.05/3) were considered statistically significant.
Results
Participants
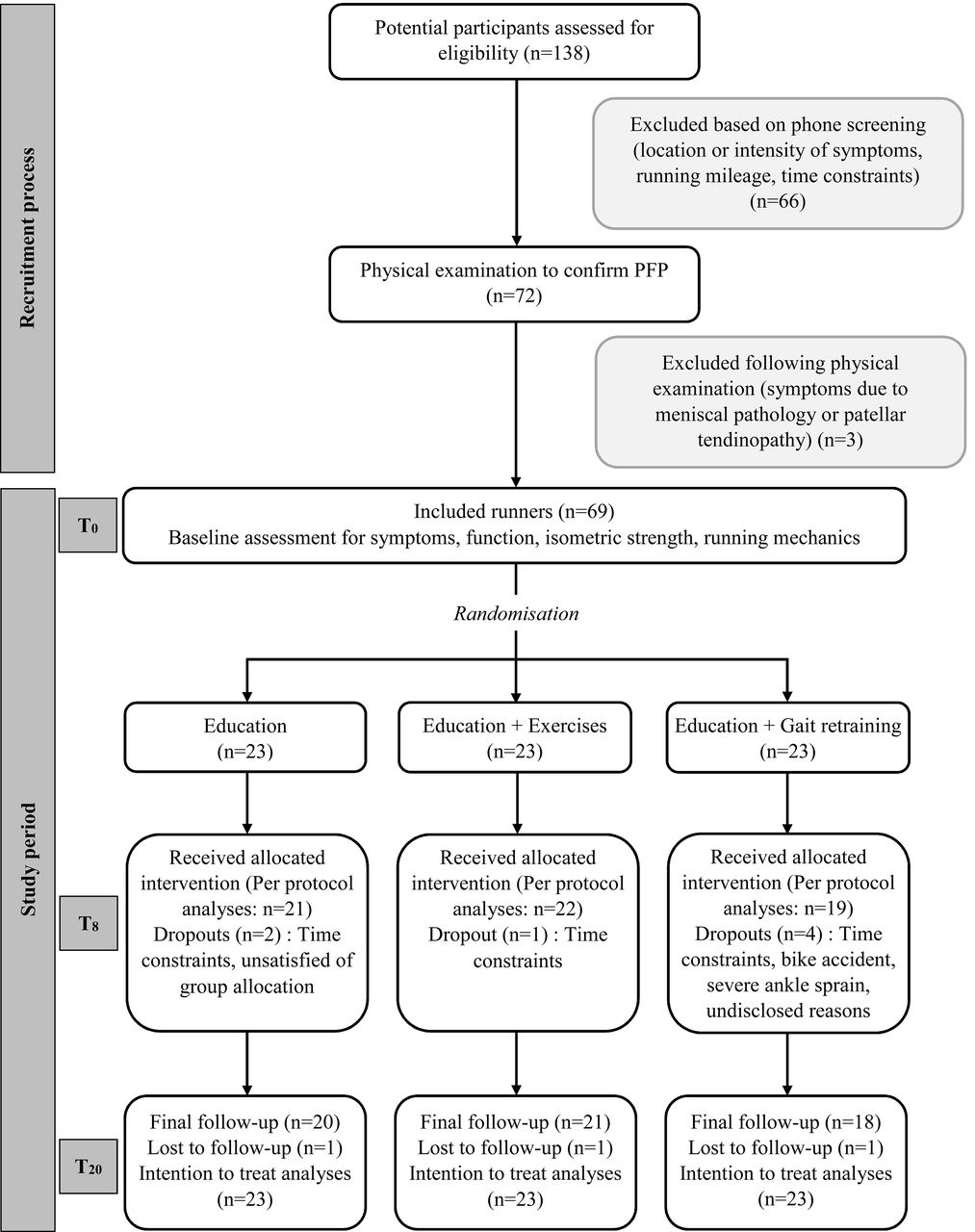
Between July 2014 and December 2015, 69 runners (table 1) were recruited from 138 potential candidates and randomly assigned to one of the three intervention groups (figure 1). Seven participants dropped out of the study before T8 (follow-up rate=89.9%), and three additional runners failed to return their follow-up questionnaires at T20 (follow-up rate=85.5%). During the course of the study, 19 appointments (all by dropouts) were missed at the physiotherapy clinic (attendance rate=94.5%). At T8, self-declared compliance to instructions (training modifications, exercises and gait modifications) averaged 88.9% and was not different between groups (p=0.652). No participant declared implementing additional therapeutics (eg, medications and manual therapy). The evaluator declared knowing group allocation for two runners who mistakenly revealed their programme.
Baseline participants characteristics (n=69)

Flow of participants through study.
Between T0 and T8, five new injuries (running or non-running related) were reported by participants. One minor injury, a calf strain secondary to running gait modifications was related to the study protocol (gait retraining group). That injury was successfully managed through reductions in running mileage during <2 weeks. All other injuries were deemed minor, non-running related and managed in a similar fashion (reductions in running mileage).
A significant between-group difference was found for age (p=0.031) and a trend was found for duration of symptoms (p=0.076); therefore, both variables were included as covariates (ANCOVA). However, due to their lack of influence on all outcomes (p>0.05), age and duration of symptoms were not further considered in the final statistical models.
Symptoms and functional outcomes
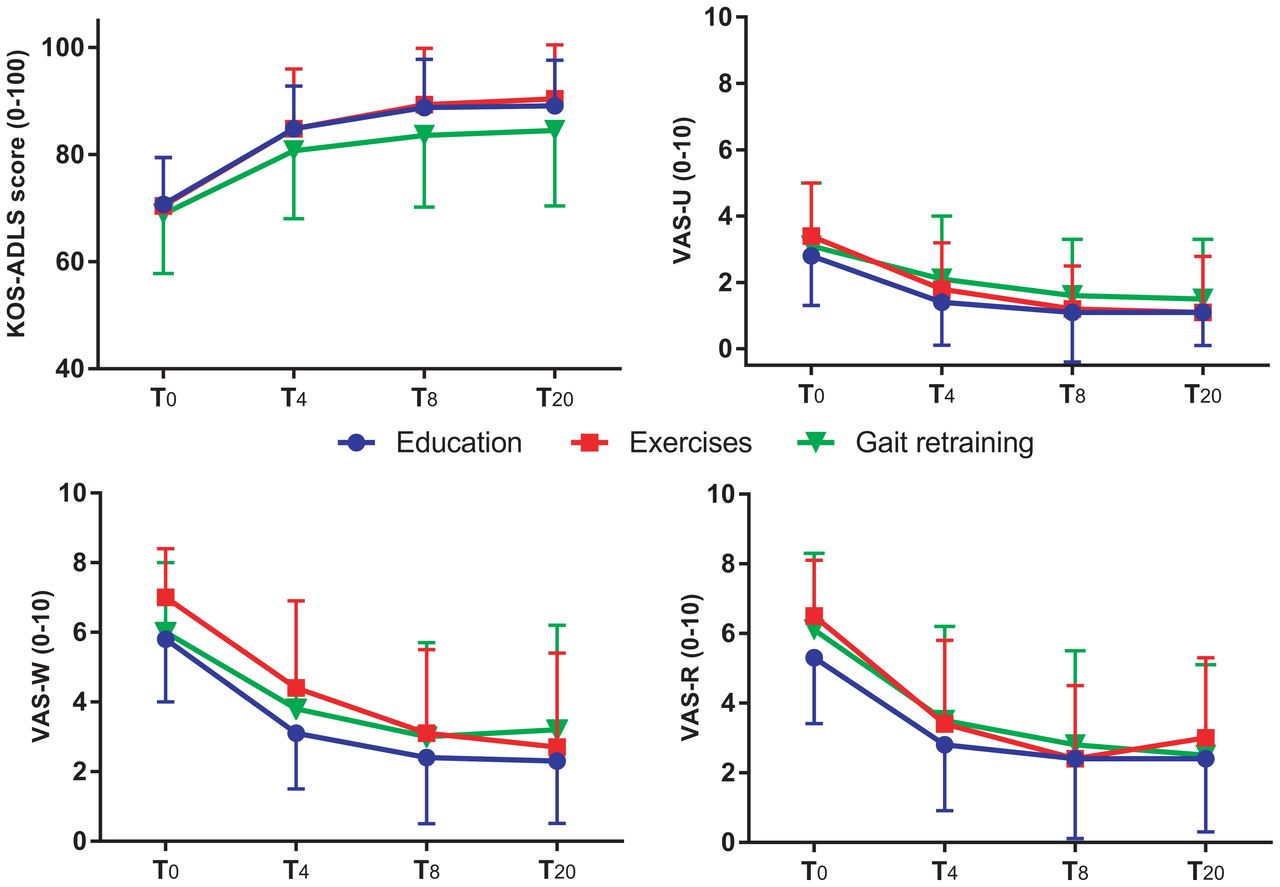
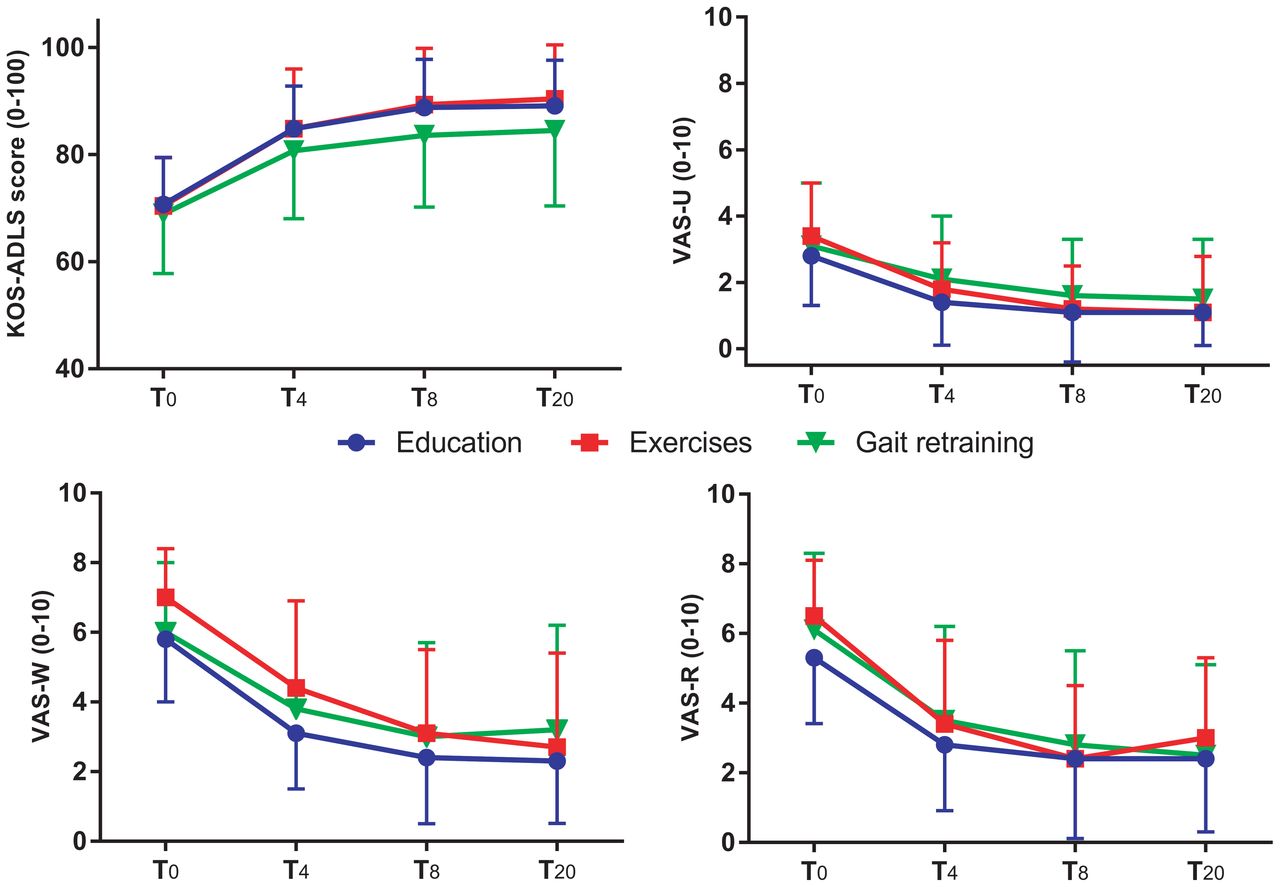
Intention-to-treat and per-protocol analyses showed no statistically significant group × time interaction (p≥0.71) for KOS-ADLS. However, all three groups experienced significant improvements (time effect; p<0.05) in mean scores at T4, T8 and T20 compared with T0 (tables 2 and 3, figure 2). Mean KOS-ADLS change scores reached the MCID at T4 for the education and exercises groups, and at T8 for the gait retraining group. Improvements were maintained between T8 and T20 for all groups (tables 2 and 3).
{kind=link}
{kind=link}
Mean group scores to KOS-ADLS and VASs. Error bars show SD.
Group scores for symptoms and function outcomes presented as mean±SD
Treatment effects on symptoms and function outcomes
Similarly, no significant group × time interaction effects were found for VASs (p≥0.43; table 3). All three groups exhibited significant changes with baseline values at T4, T8 and T20, and improvements in pain scores were maintained between T8 and T20 (time effect; p<0.05; tables 2 and 3, figure 2).
As for running distance, no group × time interaction effect was found (p=0.649). A significant time effect (p<0.001) revealed that participants ran significantly more at T8 compared with T0 (table 3). However, weekly distance decreased between T8 and T20 (p=0.018). Values at T20 were not significantly different from T0 (tables 2 and 3).
Isometric strength
A significant group × time interaction was found for knee extension strength (p<0.001); post-hoc analyses showed that the exercises group was the only one in which knee extensors isometric strength increased significantly compared with baseline (p<0.001) (table 4). Significant time effects for hip external rotators (p=0.015) and abductors (p=0.001) strength were also observed.
Treatment effects on lower limb isometric strength and running mechanics
Running mechanics
A significant group × time interaction effect (p=0.001) was found for step rate (table 4). Only the gait retraining group significantly increased step rate between T0 and T8 (+7.0%, p<0.001). Similarly, a significant group × time interaction effect (p=0.001) was observed for average vertical loading rate during running, with only the gait retraining group displaying a significant decrease (−25.4%, p<0.001) (table 4). No significant group × time interaction effects were found for PFJ peak force (p=0.127) or PFJ average loading rate (p=0.263), even though reductions in PFJ average loading rate were found for gait retraining (−12.5%, p=0.027), and values of PFJ peak force at T8 were lower in the gait retraining group than in the education group (−12.3%, p=0.024; table 4).
Discussion
This is the first RCT comparing commonly advocated rehabilitation approaches in runners with PFP. Our first hypothesis regarding significant benefits in all groups was confirmed. However, contrary to our second hypothesis, adding exercises or gait retraining did not provide additional benefits compared with education alone, and the gait retraining group did not exhibit faster improvements than other groups. Similar changes in KOS-ADLS and VASs suggest that education alone may be as efficient in decreasing symptoms and functional limitations of runners with PFP as education combined with exercises or gait retraining.
Education has emerged as an important treatment component in individuals with PFP.10 18 In runners, appropriate management of training loads may represent a key aspect, as training errors often contribute to symptoms onset.13 41 In this study, participants’ understanding of appropriate training modifications according to symptoms was ensured through repeated physiotherapist guidance and feedback, using detailed explanations on adaptation and modifiable running schedules. Indeed, moderate repetitive loading is known to help maintain healthy articular cartilage,42 while increased training frequency could represent a protective factor against injury.43 Decreasing running speed, avoiding hills and splitting total weekly distance into more frequent but shorter sessions may have allowed runners to maintain PFJ loads within the envelope of function14 and ultimately experience durable improvements in symptoms. It could also be hypothesised that decreasing running speed may achieve the same purpose as gait retraining approaches aiming for transient decreases in PFJ forces. Indeed, reducing speed decreases knee moments in a similar fashion as imposing a forefoot strike pattern, although without increasing ankle moments.44
While gait retraining did not provide additional or faster benefits on symptoms and functional limitations over education alone, the gait retraining group increased their step rate by an average of 7.0%, a slightly lower value than the 7.5%–10% increase suggested by previous studies.22 30 Yet, average vertical loading rate and PFJ average loading rate were significantly reduced. The approach used in this study was preferred over the frontal plane kinematics retraining approach.45 46 When using the frontal plane approach with females displaying excessive hip adduction, both Willy et al 46 and Noehren et al 45 attributed benefits to decreased peak angles during stance; yet, the latter study reported a concurrent decrease in average vertical loading rate, suggesting that other mechanisms may have contributed to clinical success. Interestingly, previous studies on gait retraining20 21 45 46 have all used the same ‘faded-feedback protocol’, constraining runners to eight running sessions over 2 weeks (week 1: 78 min; week 2: 117 min). In fact, such standardised protocol imposed a reduced training regimen to study participants (baseline average=23.3–32.8 km). Therefore, it cannot be excluded that, similar to the current study, modulation of training loads contributed to clinical success.
Only one single-group cohort study reported beneficial effects of an exercise programme in runners with PFP,47 which targeted hip abductors strengthening. In addition to the exercises used in that study, our programme followed the latest recommendations of combining hip and knee exercises.11 15–17 48 The interaction effect found for knee extension strength shows that exercises led to increased strength, but without additional benefits on symptoms and function. Thus, strength increase is potentially not a moderator of clinical improvement. However, it is possible that exercises may provide longer-term benefits by increasing tissues’ capacity to sustain loads, which likely represents an important outcome in runners.
Our results highlight the importance of education and management of training loads according to symptoms, which should be addressed by sports medicine practitioners to decrease symptoms and empower runners with self-management strategies. These results should not discourage clinicians from prescribing gait retraining and exercises if judged necessary to target specific mechanisms, but rather emphasise the central role of appropriate education. Clinicians and future studies should consider individual pain response when issuing recommendations on training loads in runners with PFP, instead of replicating generic parameters such as the number or duration of sessions.
Our design did not include a ‘no treatment’ group. Therefore, spontaneous resolution of symptoms cannot be excluded. However, given the 3-month minimum duration of symptoms for inclusion, attributing symptoms improvements to time is rather unlikely. A placebo effect secondary to the clinician-patient interaction is possible, but must be considered as an integral part of the clinical context. Also, while a larger sample may have provided additional insights on changes in strength or running mechanics, our results suggest that such effects would likely be small and not clinically relevant. It remains unknown if the addition of gait retraining or exercises could provide additional benefits over time. Further research is needed to compare longer term effects of such rehabilitation programmes. Lastly, the higher number of dropouts in the gait retraining group may be seen as a limitation, and the use of intention-to-treat analyses could have undermined the effects of such intervention. Yet, similar findings were observed with per-protocol analyses, and changes in running mechanics were observed as expected in that group.
Conclusion
Results from this study did not provide evidence that exercises or gait retraining offer additional benefits in reducing symptoms of runners with PFP over education alone. Neither increased knee extensors strength in the exercises group nor increased step rate and decreased average vertical loading rate in the gait retraining group were translated into improved outcomes. Therefore, clinical interventions in runners with PFP should include appropriate education on symptoms and management of training loads as a primary component of treatment.
What are the findings?
Education on appropriate management of training loads according to symptoms is a vital component when treating runners with PFP.
All three programmes (education; education and exercises,and education and gait retraining) were effective in improving symptoms and functional limitations of runners with PFP.
Changes in targeted mechanisms (isometric strength and running mechanics) were achieved but did not provide additional benefits on symptoms and function compared with education alone.
How might it impact on clinical practice in the future?
Sports medicine practitioners should consider education on appropriate management of training loads based on level of symptoms as a central treatment component for runners with PFP.
Exercises and gait retraining can be considered for their individual benefits as judged necessary.
Acknowledgments
The authors would like to thank all runners who participated to this study, Guy St-Vincent for his assistance in laboratory data collection as well as physiotherapists who provided the interventions (M.-L. Blanchette, L. Ethier, D. Laperrière, S. Martin, J. Picard-Arsenault and V. Voyer).
References
Footnotes
Contributors JFE, LJB, BD, PF, LM and JSR designed the study. JFE, LJB, BD, PF and JSR created the study protocol. LM is the statistician. BM contributed to laboratory data analysis. JFE and JSR directed the publication. All authors contributed to writing and approved the final version of the manuscript.
Funding JFE received scholarships from Canadian Institutes for Health Research (CIHR) and Fonds de recherche du Québec – Santé (FRQ-S). JSR was supported by a salary award from the CIHR and FRQ-S. This study was funded by the Réseau Provincial de Recherche en Adaptation/Réadaptation – Fonds de Recherche du Québec – Santé (REPAR/FRQ-S), Ordre Professionnel de la Physiothérapie du Québec (OPPQ), Physiotherapy Foundation of Canada (PFC) and Canadian Academy of Sport and Exercise Medicine (CASEM). The funding agencies had no role in the study design, analysis of results, writing of the manuscript or in the decision to submit for publication.
Competing interests None declared.
Ethics approval Quebec Rehabilitation Institute research ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.