Article Text

Abstract
Background Hamstring injuries occur frequently in field sports, yet longitudinal information to guide prevention programmes is missing.
Aim Investigate longitudinal hamstring injury rates and associated time loss in elite Gaelic football, while identifying subgroups of players at increased risk.
Methods 38 data sets from 15 elite male Gaelic football teams were received by the National Gaelic Athletic Association (GAA) Injury Surveillance Database between 2008 and 2015. Injury and exposure data were provided by the team's medical staff via an online platform.
Results 391 hamstring injuries were sustained accounting for 21% (95% CI 20.0% to 21.7%) of all injuries. Prevalence was 21% (95% CI 19.2% to 23.4%). Incidences were 2.2 (95% CI 1.9 to 2.4) per 1000 exposure hours, and 7.0 (95% CI 6.5 to 7.1) times greater in match play than in training. Typically each team sustained 9.0 (95% CI 7.0 to 11.0) hamstring injuries per season affecting the: bicep femoris belly (44%; 95% CI 39.4% to 48.7%); proximal musculotendinous junction (13%; 95% CI 9.8% to 16.3%); distal musculotendinous junction (12%; 95% CI 8.6% to 14.9%) and semimembranosis/semitendinosis belly (9%; 95% CI 6.3% to 11.7%). ∼36% (95% CI 31.5% to 41.0%) were recurrent injuries. Mean time loss was 26.0 (95% CI 21.1 to 33.0) days, which varied with age, injury type and seasonal cycle. Hamstring injuries accounted for 31% (95% CI 25.8% to 38.2%) of injury-related time loss. Previously injured players (rate ratio (RR)=3.3), players aged 18–20 years (IRR=2.3) or >30 years (RR=2.3), as well as defensive (IRR=2.0) and midfield players (RR=1.5), were most at risk of sustaining a hamstring injury. Comparisons of 2008–2011 with 2012–2015 seasons revealed a 2-fold increase in hamstring injury incidences. Between 2008 and 2015 training incidence increased 2.3-fold and match-play incidences increased 1.3-fold.
Conclusions Hamstring injuries are the most frequent injury in elite Gaelic football, with incidences increasing from 2008–2011 to 2012–2015. Tailoring risk management strategies to injury history, age and playing position may reduce the burden of hamstring injuries.
- Epidemiology
- Football
- Hamstring
Statistics from Altmetric.com
Introduction
Gaelic football match play consists of two 35 min periods separated by a 10 min half-time interval.1 Match play is characterised by intermittent bouts of multidirectional running as elite players reportedly cover 8889 m, with 18% at a high-speed pace (>17 km/hour).2 Two opposing teams of 14 outfield players and a goalkeeper play on a grass pitch 145 m long by 90 m wide.1 The aim is to outscore the opposition at H-shaped goal posts by kicking or striking a round ball over (1 point), or under (1 goal or 3 points) a crossbar. Shoulder-to-shoulder contact is permitted, but 67.8% of injuries are from non-contact mechanisms.1
As field sports are associated with exposure to potentially harmful events, highly susceptible players need to be identified so that injury risk management strategies can be implemented.3 The initial steps of this process involve investigating injury rates and risk factors.4 Hamstring injuries account for a large proportion of injuries in elite soccer (12%), rugby union (15%), Australian football (16%) and hurling (17%).5–8 Hamstring injuries are mostly non-contact in nature and recurrence is common.1 ,5 ,8 However, hamstring injury rates have yet to be investigated in Gaelic football.
Injury surveillance databases facilitate the monitoring of injury rates over consecutive seasons.9 The Gaelic Athletic Association (GAA) Medical, Scientific and Player Welfare Committee established the National GAA Injury Surveillance Database in 2007 to monitor injury incidences in elite Gaelic games. Previously it was reported that the injury incidence in elite Gaelic football was 9.5 per 1000 exposure hours.1 However, longitudinal injury trends have yet to be reported, particularly in relation to hamstring injuries. Likewise, the impact of hamstring injuries on time loss and future injury risk has yet to be investigated. Thus, we aimed to chart longitudinal hamstring injuries and associated time loss in elite Gaelic football. We also aimed to identify subgroups of elite players at increased risk of sustaining a hamstring injury.
Materials and methods
Fifteen elite male teams participated, which provided 38 season data sets. All teams were division 1 standard, and enrolled in the National GAA Injury Surveillance Database between 2008 and 2015 seasons. Injury and weekly exposure data were provided by team medical staff via an online platform customised to collect the desired data (table 1). As the elite competitive season starts in January and concludes in September, data collection began on 1 January each year with teams prospectively followed until elimination from competition. Data collection ceased for the off-season and restarted the following January. Player anonymity was maintained and data protection assured in accordance with ethical approval received from the University Research Ethics Committee.
Injury definitions
Definitions
Information packs regarding injury definitions and classifications (table 1) were distributed to participating teams and embedded onto the user interface of the online platform.10 Injury diagnosis was made by a medical doctor or chartered physiotherapist, and stratified as: hamstring bruising/haematoma; biceps femoris belly; distal musculotendinous junction; proximal musculotendinous junction; semimembranosis/semitendinosis belly; or unspecified hamstring region. An unspecified hamstring region was used where the precise location of the hamstring injury was not identified. Players were divided into subgroups based on age and playing position to facilitate calculation of injury incidences for specific subgroups. For the purposes of the current study, the season was divided into four cycles: preseason (weeks 1–7); competitive cycle 1 encompassing provincial shield and National League (weeks 8–16); mid-season (weeks 17–22); and competitive cycle 2 encompassing the Provincial-National Championship (weeks 23–34).
Data analysis
Data were entered into statistical analysis software (IBM SPSS Statistics V.20.0). Continuous variables are reported as mean with 95% CIs while team rates are reported as median with IQRs. Injury incidences are reported per 1000 exposure hours. Injury burden was calculated by multiplying mean time loss by the injury incidence to report days lost per 1000 exposure hours. Incidence rate ratios (IRR) were calculated to assess injury risk across age groups playing positions. In the current study, IRR was calculated by comparing an incidence rate for a specific subgroup of players relative to that for all other players (eg, 18–20 years old relative to all other players). The risk of sustaining another hamstring injury was calculated only for players registered over consecutive seasons using relative risk ratios (RR).
Results
A total of 391 hamstring injuries were sustained by 307 players (table 2). Approximately 21% (95% CI 19.2% to 23.4%) of enrolled players sustained a hamstring injury. Hamstring injuries accounted for 21% (95% CI 20.0% to 21.5%), 29% (95% CI 26.8% to 31.2%) and 28% (95% CI 25.6% to 30.7%) of total, training and match-play injuries, respectively.
Incidence and burden of hamstring injuries across eight seasons
Incidence
In total, 182 047 exposure hours were recorded. On average teams accumulated 4791 (95% CI 4395 to 5220) exposure hours per season, with a ratio of training to match-play hours of 7.6 (95% CI 7.1 to 8.0). Hamstring injury incidence per 1000 exposure hours was 2.2 (95% CI 1.9 to 2.4). Incidence was 7.0 (95% CI 6.5 to 7.1) times greater in match play when compared with training (table 2).
Team injury rate per season
Mean season duration was 31 weeks (95% CI 29.9 to 32.8). The mean number of players per elite Gaelic football team was 38.0 (IQR 33.0–39.0). Typically, 27.0 (IQR 20.0–29.0) players sustained 42.0 (IQR 33.0–51.0) injuries per season, which included 9.0 (IQR 7.0–12.0) hamstring injuries. Hamstring injuries were stratified as: biceps femoris belly (44.1%; 95% CI 39.4% to 48.7%); proximal musculotendinous junction (13.1%; 95% CI 9.8% to 16.3%); distal musculotendinous junction (11.9%; 95% CI 8.6% to 14.9%); semimembranosis/semitendinosis belly (8.9%; 95% CI 6.3% to 11.7%) and bruising (1.2%; 95% CI 0.0% to 2.3%). The locations of 21% (95% CI 17.0% to 24.5%) hamstring injuries were unspecified (ie, not precisely defined).
Injuries per seasonal cycle
Overall, 17% (95% CI 13.2% to 21.5%) of hamstring injuries occurred during preseason. Approximately 64% (95% CI 54.4% to 72.8%) of hamstring injuries occurred during competitive cycles, with 25% (95% CI 20.7% to 29.0%) and 39% (95% CI 33.7% to 43.8%) in competitive cycles 1 and 2, respectively. The remaining 19% (95% CI 15.3% to 23.1%) occurred during mid-season cycles.
Injury type
Acute (77.6%; 95% CI 73.4% to 81.6%) hamstring injuries were more prevalent than chronic (5.8%; 95% CI 3.7% to 8.2%), or overuse (15.9%; 95% CI 12.6% to 19.2%) cases (table 3). Overall, 73% (95% CI 69.2% to 77.6%) occurred during running. Most hamstring injuries were new (63.9%; 95% CI 59.0% to 68.5%) as opposed to recurrent (36.1%; 95% CI 31.5% to 41.0%). The proportion of recurrent hamstring injuries varied between sites (table 3). Overall, 39% (95% CI 28.2% to 44.7%) of recurrent hamstring injuries were sustained within 8 weeks of return to play.
Hamstring injury type
Quarter of play
Most hamstring injuries occurred during match play (49.1%; 95% CI 42.5% to 57.1%) and pitch training (45.9%; 95% CI 41.5% to 51.0%). Timing of injury was provided for 94% (n=367) of injuries. The proportion of hamstring injuries occurring in quarters 1–4 were 23% (95% CI 19.1% to 27.2%), 23% (95% CI 18.5% to 27.8%), 28% (95% CI 22.9% to 32.7%) and 26% (95% CI 21.5% to 30.8%), respectively.
Age groupings
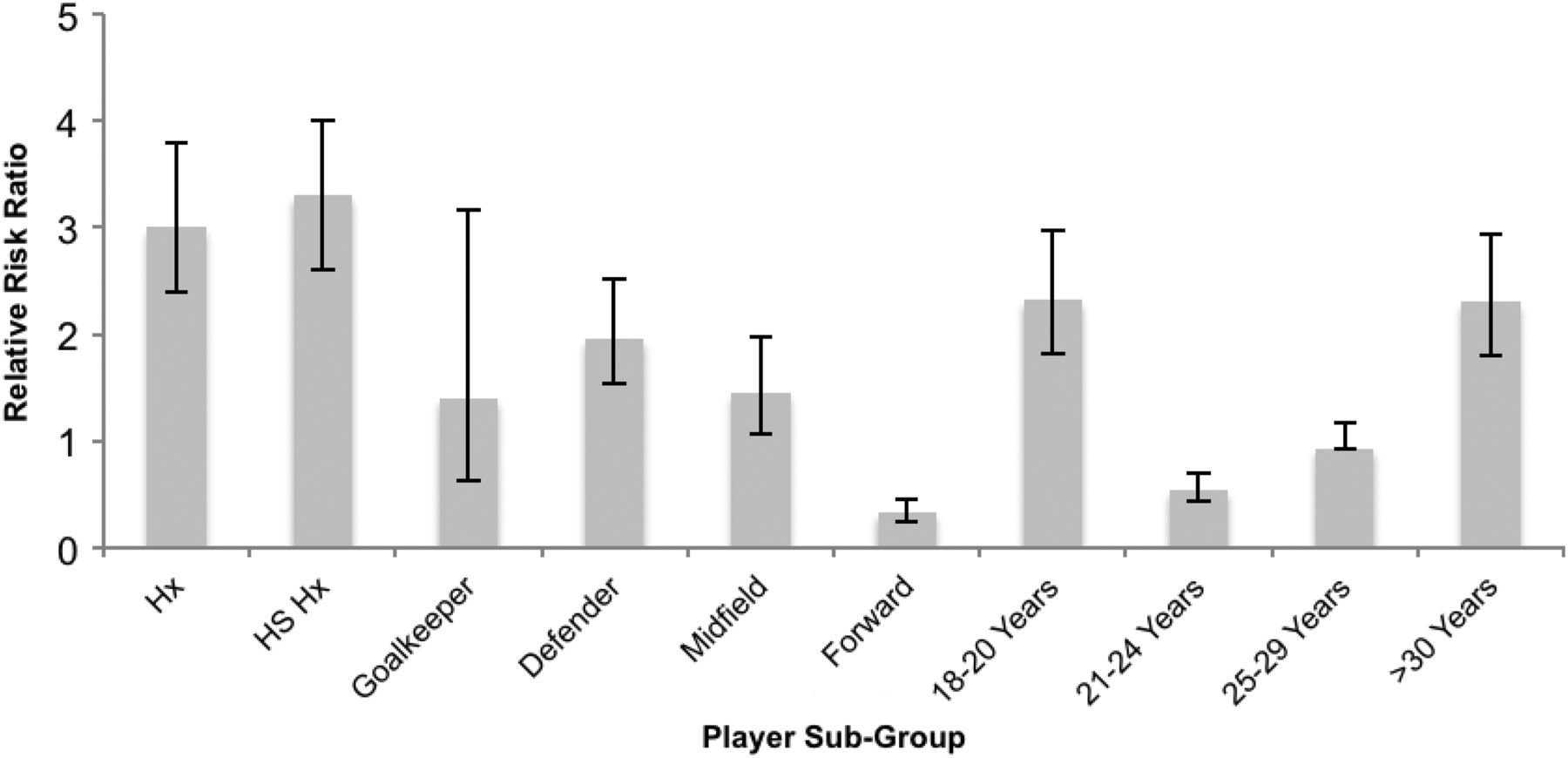
Hamstring injury incidence per 1000 exposure hours varied across age groups for 18–20 years (4.5; 95% CI 3.5 to 5.5), 21–24 years (1.5; 95% CI 1.2 to 1.8), 25–29 years (2.1; 95% CI 1.8 to 2.5) and >30 years (3.1; 95% CI 2.2 to 3.9). The IRR per age group, reflecting injury incidence relative to all other players, was the greatest for those aged 18–20 years (2.3; 95% CI 1.8 to 3.0) and >30 years (2.3; 95% CI 1.8 to 2.9; figure 1). Players aged 21–24 and 25–29 years had an IRR of 0.5 (95% CI 0.4 to 0.7) and 0.9 (95% CI 0.8 to 1.2), respectively.
{kind=link}
Risk ratio per player subgroup. Figure reveals risk ratio relative to all other players with corresponding 95% CI. Hx, history of previous injury; HS Hx, history of previous hamstring injury.
Prior injury and position of play
Compared with their uninjured counterparts, players with any previous injury were 3.0 (95% CI 2.4 to 3.8) times more likely to sustain a hamstring injury (figure 1). However, risk was even greater for players with a previous hamstring injury, compared with those without prior hamstring injury history (RR 3.3; 95% CI 2.6 to 4.0). In total, 44% of players with a previous hamstring injury sustained another. When the incidence rates were compared across positions, the hamstring injury IRR varied between goal keepers (RR 1.4; 0.63 to 3.17), defenders (IRR 1.96; 95% CI 1.53 to 2.51), midfielders (IRR 1.45; 95% CI 1.06 to 1.98) and forwards (RR 0.33; 0.24 to 0.45).
Initial prognosis versus actual severity
At the time of diagnosis practitioners believed that 62% (95% CI 57.2% to 67.0%), 36% (95% CI 31.2% to 40.7%) and 2% (95% CI 0.8% to 3.6%) would result in mild (1–7 days), moderate (8–28 days) and severe (>28 weeks) time loss, respectively. However, analysis of time-loss data revealed that 21% (95% CI 15.9% to 25.4%), 56% (95% CI 50.4% to 62.9%) and 23% (95% CI 18.2% to 28.0%) of hamstring injuries were actually mild, moderate and severe, respectively. A large proportion of mild (72%) and moderate (46%) hamstring injuries resulted in more time loss than predicted.
Time loss
On average, hamstring injuries resulted in 26.0 (95% CI 21.1 to 33.0) time-loss days from sport, equating to 299.0 (95% CI 211.0 to 438.9) days per team each season (table 2). This accounted for 31.1% (95% CI 25.8% to 38.2%) of injury-related time loss from sport each season. The number of days lost per 1000 exposure hours (ie, injury burden) was 57.2 (95% CI 40.1 to 79.2). Injury burden was 10.7 times (95% CI 8.8 to 11.4) greater for match play (213.4/1000 hours; 95% CI 140.6 to 305.3) than training injuries (20.0/1000 hours; 95% CI 16.0 to 26.7). Time loss differed in relation to injury type, sites, inciting activity, age and seasonal cycle (table 4).
Hamstring injury time-loss data
Variation across seasons
For the purpose of investigating variations across seasons, data were grouped into two periods of 2008–2011 or 2012–2015 seasons. Hamstring injury incidences increased twofold (1.9 vs 3.9 per 1000 hours) between these time periods. Training incidences increased 2.3-fold (1.0 vs 2.4) while match-play incidences increased 1.3-fold (9.7 vs 12.8). Over this period, the difference between match play and training incidences grew by 20%. Prevalence of hamstring injuries among all elite Gaelic football players increased by 45% (18.9% vs 27.4%) over the investigated periods. Between 2008 and 2011 elite Gaelic football teams typically sustained 9.0 hamstring injuries per season, however, between 2012 and 2015 this increased by 39% to 12.5 hamstring injuries.
Discussion
Hamstring strains are the most common injuries in elite Gaelic football accounting for 21% of injuries and 31% of injury-related time loss. Although 21% of registered elite players experienced at least one hamstring injury per season over the investigated period, prevalence increased by 45% from 2008/2011 to 2012/2015 seasons. Prevalence in the current study is comparable to elite soccer (22%) but greater than elite rugby union (11%).5 ,11 Typically elite Gaelic football teams sustained 9.0 hamstring injuries per season, with increases observed in latter seasons. Such team rates are higher than reports in elite soccer (6.0), elite Australian football (6.0) or elite rugby union (7.5).7 ,10 ,12
Hamstring injuries are a growing problem
However, as season duration and accumulation of exposure hours vary between teams, the incidence rate per 1000 hours may be a more appropriate method of evaluating injury rates. The current study reported that for every 1000 hours of exposure, 2.2 (95% CI 1.9 to 2.4) hamstring injuries were sustained, and a twofold increase was observed between 2008/2011 (1.9/1000 hours) and 2012/2015 (3.9/1000 hours). Previous studies among subelite Gaelic footballers reported that hamstring injuries accounted for ∼12% of all injuries (1.6/1000 hours).13 Thus, hamstring injuries appear to be more frequent in elite Gaelic football than in subelite levels.
In comparison to training, hamstring injury incidence was seven times more frequent and the injury burden was 10.7 times greater in match play. Despite a greater increase in training incidence (2.3-fold) than match play (1.3-fold), the difference between match-play and training incidences grew by 20%. Such trends suggest that training demands increased in an injurious manner, and that deployed training methods offered less protection to players during match play. Essentially, when exposure is standardised to 1000 hours, both training and match-play activities were more injurious in 2012/2015 than in 2008/2011.
Considerations for managing injury risk
The current study revealed that most hamstring injuries in elite Gaelic football were acute (78%) and occurred while running (73%). Second, over one-third (36%) of hamstring injuries were recurrent in nature, with 39% recurring within 8 weeks of return to play. Thus, activities to prepare players for the running-based demands of Gaelic football should be investigated, particularly for players returning from injury. Recurrent hamstring injuries are also common in elite Australian football (20%), elite soccer (16–23%) and subelite soccer (12.5%).7 ,14 Thus, higher recurrence rates in elite Gaelic football when compared with other field sports suggests some rehabilitation programmes are limited in facilitating complete recovery. Factors leading to re-injury have been identified previously and should be addressed in training programmes.15
Third, a positional hamstring injury profile revealed that defenders (1.96; 95% CI 1.53 to 2.51) and midfielders (1.45; 95% CI 1.06 to 1.98) were more at risk than forwards (0.33; 95% CI 0.24 to 0.45). Such results may relate to the variation of physical demands across playing positions. For instance, high-speed distance (>17 km hour) is reportedly lower for forwards (18.2 m/min) than defenders (22.5 m/min) or midfielders (31.8 m/min).2 The large 95% CI IRR observed for goal keepers (1.4; 95% CI 0.63 to 3.17) may reflect a small sample size or unique physical–technical demands.
Fourth, IRR per age group, reflecting injury incidence relative to all other groups, was greatest for players aged 18–20 years (2.3) and >30 years (2.3), with lower risk in the middle age groups. This U-shaped trend indicates that risk is greatest for players transitioning in and out of elite Gaelic football teams. Age-related fitness differences have been observed during the Yo-Yo Intermittent Recovery Test (level 1) for subelite Gaelic footballers.16 Interestingly, players aged 18–20 years performed lower than their older counterparts.16 Thus, players may be at increased risk when adapting to increased demands associated with more strenuous or elite playing levels. Similarly, it could be speculated that accumulation of demands over many seasons increases the risk for players >30 years.
Additionally, considering the typical season duration was 31 (95% CI 29.9 to 32.8) weeks, 17% of all hamstring injuries occurred within the initial 7 weeks or 22% of the season. This suggests that demands of preseason activities were not particularly injury prone. However, deconditioning over the offseason may increase susceptibility to fatigue.17 In elite Australian football players with reduced preseason eccentric hamstring strength were 2.7 times (95% CI 1.3 to 5.5; p=0.006) more likely to sustain an injury than players above this threshold.18 However, elite AFL players with hamstring injury history demonstrated less eccentric strength development across preseason training, which may increase risk of recurrence.19 Thus, ineffective preseason training stimuli may impair readiness for competitive cycles, thereby increasing in season injury risk. Adverse responses may be more pronounced during congestive periods as hamstring injury rates were 1.3 times higher in elite soccer matches separated by ≤4 days' recovery compared with ≥6 days' recovery.20
Furthermore, biceps femoris belly (44%; 95% CI 39.4% to 48.7%) was the most frequently diagnosed hamstring injury site. In elite English soccer a similar proportion of biceps femoris (53%) injuries have been reported as opposed to semitendinosus (16%) or semimembranosus (13%).21 However, perhaps due to lack of confirmation from diagnostic tests, some cases are difficult to stratify as a specific site as marked by 21% being unspecified. The proportion of recurrent injuries at the proximal musculotendinous junction (54%; 95% CI 40.7% to 66.7%) and semimembranosis/semitendinosis belly (42%; 95% CI 25.0% to 58.3%) were more common than at other sites. In elite European soccer players, recurrence rates following 8 weeks of return to play differ between biceps femoris (18%) and semitendinosus/semimembranosis (2%), questioning whether accelerated rehabilitation programmes are safe or effective for all hamstring injuries.22 The injury type of specific sites suggests that certain activities may progressively adversely overload different sites and may require different treatment or risk management strategies following return to play (table 3). We note that several randomised control trials showed efficacy in reducing hamstring injury rates, but that only 14% of elite soccer teams used these programmes.23 ,24 The injury prevention practices of elite Gaelic football teams remains to be investigated.
Guiding prognosis and clinical decision-making
Typically, hamstring injuries resulted in 26.0 (95% CI 21.1 to 33.0) time-loss days from sport. Time loss was greater for injuries with proximal musculoskeletal junction involvement, incited via match play, when recurrent, when sustained in preseason, and among players aged 25–29 years. Thus, various entities associated with different injury types result in distinct time-loss patterns, indicating that modified programmes may be required for various types of hamstring injuries.25 The current study also found differences between estimated time loss at diagnosis when compared with actual time-loss data. Such results highlight difficulties with gauging the complex interplay between the many variables influencing time loss. Practitioners should consider prognostic factors identified by the current study when estimating time loss.
Impact of hamstring injuries
The impact of hamstring injuries may be best appreciated by considering time loss from sport and reinjury rates.26 The current study reported that elite Gaelic football teams typically sustained 9.0 (IQR 7.0–12.0) hamstring injuries per season resulting in 299.0 (95% CI 211.0 to 438.9) time-loss days. Additionally, time loss varied for injury type (new or recurrent, training or match play) and player profile (eg, age, injury history). Beyond guiding prognosis, such data reveal that hamstring injuries reduce opportunities for player development and performance.
Compared with uninjured players, players with any previous injury or previous hamstring injury had similar RR of sustaining a future hamstring injury (3.0 vs 3.3). In elite soccer, previous hamstring strains increases risk of future injury threefold to sevenfold.27 Thus, injury risk is influenced by previous injury, even when injury types differ, implying that certain players will inherently have different subsequent injury rates. Mitigating factors include responses to injury such as neural inhibition, selective atrophy, reduced fascicle length, eccentric strength deficits and increased susceptibility to fatigue.28–31 As return to play decision-making often centres on whether practitioners believe that the athlete has an acceptable level of risk of future injury, identifying persisting maladaptations may be advantageous in reducing recurrent injury rates.31
What are the findings?
Typically each elite Gaelic football team sustained 9.0 (7.0 to 11.0) hamstring injuries per season, or 2.2 (1.9 to 2.4) hamstring injuries per 1000 exposure hours. Hamstring injury incidences are 7.0 (6.5 to 6.9) times greater in match play than in training.
Comparisons of 2008–2011 with 2012–2015 seasons revealed a twofold increase in hamstring injury incidences per 1000 hours.
Hamstring injury severity, as measured by time loss from sport, varies in relation to age, injury type, injury history and seasonal cycle.
How might it impact on clinical practice in the future?
These data may guide practitioners in monitoring hamstring injury rates while identifying specific injuries to be targeted during prevention programmes.
Our study also identifies players at increased risk of hamstring injury based on their injury history, age and playing position.
Time-loss data may provide a perspective for clinicians trying to guide prognosis.
Acknowledgments
This work was supported by an unrestricted educational grant from the Medical, Scientific and Player Welfare Committee of the Gaelic Athletic Association. It would not have been possible without the support of the participating teams.
References
Footnotes
Twitter Follow Mark Roe @markroecoach
Contributors MR, CB and JCM develop the idea for the manuscript. JCM and CB developed the data collect system. MR, CB and CG analysed the data. All authors contributed to the writing, revision and final approval of the manuscript.
Competing interests None declared.
Ethics approval University College Dublin, Human Subjects Research Ethics Committee and University Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Summary data from the injury database can be accessed by contacting the corresponding author.