Article Text

Abstract
Low energy availability (EA) is suspected to be the underlying cause of both the Female Athlete Triad and the more recently defined syndrome, Relative Energy Deficiency in Sport (RED-S). The International Olympic Committee (IOC) defined RED-S as a syndrome of health and performance impairments resulting from an energy deficit. While the importance of adequate EA is generally accepted, few studies have attempted to understand whether low EA is associated with the health and performance consequences posited by the IOC.
Objective The purpose of this cross-sectional study was to examine the association of low EA with RED-S health and performance consequences in a large clinical population of female athletes.
Methods One thousand female athletes (15–30 years) completed an online questionnaire and were classified as having low or adequate EA. The associations between low EA and the health and performance factors listed in the RED-S models were evaluated using chi-squared test and the odds ratios were evaluated using binomial logistic regression (p<0.05).
Results Athletes with low EA were more likely to be classified as having increased risk of menstrual dysfunction, poor bone health, metabolic issues, haematological detriments, psychological disorders, cardiovascular impairment and gastrointestinal dysfunction than those with adequate EA. Performance variables associated with low EA included decreased training response, impaired judgement, decreased coordination, decreased concentration, irritability, depression and decreased endurance performance.
Conclusion These findings demonstrate that low EA measured using self-report questionnaires is strongly associated with many health and performance consequences proposed by the RED-S models.
- relative energy deficiency
- female athlete triad
Statistics from Altmetric.com
Introduction
The importance of proper fueling for sport has been emphasised as a cornerstone of athletic health and performance for decades. In 1992, the American College of Sports Medicine (ACSM) introduced the term Female Athlete Triad to describe a phenomenon in physically active women with disordered eating (DE) (with or without an eating disorder (ED)), amenorrhea and osteoporosis.1 2 As more research on the topic emerged, the ACSM revised the Triad model to reflect a continuum along three spectra.3 An athlete could present on any point along each spectrum, from having optimal energy availability (EA), eumenorrhea and optimal bone health, to having low EA (with or without an ED), functional hypothalamic amenorrhea and osteoporosis.3 Mounting scientific evidence supports that the underlying cause of Triad is low EA (the amount of dietary energy remaining after exercise and available for other physiological functions, such as growth, muscle recovery and homeostasis).3 4
In 2014, the International Olympic Committee (IOC) defined a new syndrome, Relative Energy Deficiency in Sport (RED-S), expanding the Triad concept to encompass wide-ranging effects of energy deficits on physiological functioning, performance and general health of athletes.5 Athletes in prolonged states of low EA are at increased risk of infection, illness, fatigue and nutrient deficiencies.6–8 Low EA may pose serious consequences to the musculoskeletal and endocrine systems beyond those in the Triad model. Detriments to the gastrointestinal, renal and cardiovascular systems may also occur.3 9–11 Psychological impairments may be the result of, or contribute to, low EA.12 13 Additionally, low EA may negatively affect athletic performance.14 15 RED-S describes the central importance of EA on health and performance aspects of athletes of both sexes.5
Despite consensus on the importance of EA, the evidence for the health and performance consequences of low EA has been drawn from limited studies, most with small samples. Thus, the IOC has encouraged more research in the field.5 16–18 The purpose of this study was to evaluate the association of low EA with the health and performance RED-S outcomes in a large clinical population of female athletes. We hypothesised that the prevalence of the various RED-S consequences would be greater in adolescent and young adult female athletes with low EA than in those with adequate EA.
Methods
Participant selection
Patients presenting to the Division of Sports Medicine at Boston Children’s Hospital (a large tertiary care centre), for any medical condition related to participation in sport, were invited to participate. Female athletes (ages 15–30 years) who averaged ≥4 hours of self-reported physical activity per week for 6 months prior to participation were recruited. Exclusion criteria included non-athletes, males and athletes unable to participate in sport for the prior 6 months or more due to injury. Potential study participants were identified on the day of clinic visit. Recruitment occurred in the waiting room and the questionnaire was administered on an iPad (Apple Inc., Cupertino, CA).
Survey development
We developed an online questionnaire to assess elements of the potential physiological and performance decrements associated with low EA. The survey included 133 questions pertaining to our hypothesis: 48 independent questions and 85 sub-questions. Questions addressed general health, illness, injury, sports performance and Triad/RED-S risk factors. Response formats included multiple choice, yes/no polar responses, Likert-type scales and open-ended answers, allowing for diversity in responses. Branching logic was used to address follow-up questions to positive responses where appropriate. Because no validated or standard measure for RED-S has been developed, our group built this survey based on validated and/or standard questionnaires for each topic as available. Otherwise, health and performance consequences were assessed with questions we developed. The survey was reviewed by sports medicine physicians, endocrinologists, paediatricians, sports scientists and collegiate athletes for content validity prior to study initiation.
Low energy availability
Three measures were used to assess ED/DE, which served as a surrogate for low EA: Brief Eating Disorder in Athletes Questionnaire (BEDA-Q),19 Eating Disorder Screen for Primary Care (ESP)20 and self-reported current or past history of ED or DE (SR). BEDA-Q has been validated in female athletes to screen for ED (sensitivity=82.1%, 95% CI 76.6% to 87.6%; specificity=84.6%, 95% CI 79.4% to 89.8%) and is composed of nine questions with a weighted equation score ≥0.27 ruling in an ED.19 ESP consists of four questions: ≥3 abnormal responses classifies an individual as increased risk for an ED (likelihood ratio (95% CI)=11 (6.4–18)).20 Low EA was determined by a positive response to one or more of the three ED/DE screens.
Health consequences of RED-S
Questions were formulated to address limited aspects of each of the 10 RED-S health consequences proposed by the IOC.5 Menstrual function was considered abnormal if athletes reported primary amenorrhea (menarche >age 15.0)21 and/or a history of ≤9 periods per year.4 Bone health was considered impaired if the athlete listed ≥2 bone stress injuries, ≥1 high-risk bone stress injury (femoral neck, sacrum, pelvis)22 23 or reported a dual-energy x-ray absorptiometry Z-score <-1.3 Endocrine function was assessed by asking whether the participant ever had abnormal thyroid function test results. Metabolic abnormality was evaluated by asking whether the participant had a known low resting metabolic rate. Haematological health was assessed by asking whether the participant had a history of anaemia, low haemoglobin, iron or ferritin, and/or abnormal bruising. Positive responses in these categories classified the athlete as increased risk. Growth and development was evaluated based on self-reported adherence to normal growth curves in childhood; a negative response indicated increased risk. Impaired psychological functioning was recorded if the respondent reported seeing a mental health professional. Cardiovascular risk was assessed by adapting the heart health questions from the Preparticipation Examination – Fourth Edition:24 positive responses to ≥3 of seven questions classified the athlete as increased risk. Gastrointestinal health was evaluated with questions from the Low Energy Availability in Females Questionnaire (LEAF-Q)25 and the Faecal Incontinence Questionnaire.26 A combination of positive responses with frequency cutoffs was considered increased risk.
Performance effects of RED-S
The RED-S model proposes 10 potential performance effects arising from low EA.5 All were queried in each athlete, except for decreased glycogen stores and decreased muscle strength, which are difficult to quantify via self-report. An athlete with ≥3 separate injuries resulting in missed sports participation (practice or competition) in the past year was considered to have increased injury risk. The remaining potential performance effects (decreased training response, impaired judgement, decreased coordination, decreased concentration, irritability and depression ) were assessed with single yes/no questions.
Final survey tool
The resulting questionnaire was formatted into the HIPAA-compliant REDCap online survey platform.27 The study was approved by the Boston Children’s Hospital Institutional Review Board. Participants ≥18 years old and parents of those <18 years old provided informed consent. Participants <18 years old assented to the study.
Statistical analysis
All data were analysed using IBM SPSS Statistics for Macintosh (Version 21.0, Armonk, NY: IBM Corp). Data were analysed descriptively to evaluate questionnaire variables. Independent-sample t-tests were used to determine whether body mass index (BMI) and age differed between those with and without low EA. Each RED-S health and performance outcome was dichotomised for analysis. Chi-squared tests were used to determine whether the prevalence of each RED-S element differed between EA groups. Binomial logistic regression was used to evaluate the association between low EA and the health and performance factors associated with RED-S independently. We estimated the odds ratio (OR) for each health and performance consequence in separate regression models when low EA was present.
Patient involvement
Because RED-S is a fairly new concept, we wanted to assess the prevalence of low EA and potential RED-S health and performance consequences in our patient population. By doing this, we hoped this would allow us to better address our patients’ various health needs. We discussed our survey goals and piloted the survey with patients and used their feedback to improve the final survey.
Results
Of the 1478 patients screened to participate, 1184 were eligible. Of these, 43 declined to participate and 141 did not complete the full questionnaire. One thousand patients began the survey and completed all questions, yielding a response rate of 84.5%; only completed surveys were analysed. Descriptive characteristics of each EA group are displayed in table 1. Participants were primarily Caucasian (92.7%) and the average age was 18.92 years (SD ±3.34). Mean BMI was in the normal range for both groups, but mean BMI and age were slightly higher in the low versus adequate EA group (P<0.0001).
Descriptive characteristics
Low energy availability
Using each ED/DE screen (SR, BEDA-Q and ESP) as a surrogate for low EA, 20.1% of participants were identified by SR, 39.1% by BEDA-Q and 12.3% by ESP as having low EA. A combination of two of three measures for low EA resulted in SR and/or BEDA-Q, SR and/or ESP, and BEDA-Q and/or ESP identifying 46.6%, 24.0% and 41.4% of participants as low EA, respectively (figure 1). Using the conglomerate definition of low EA (positive response to ≥1 of the 3 ED/DE screens), the athletes were split into populations with low EA (n=473, 47.3%) and adequate EA (n=527, 52.7%).
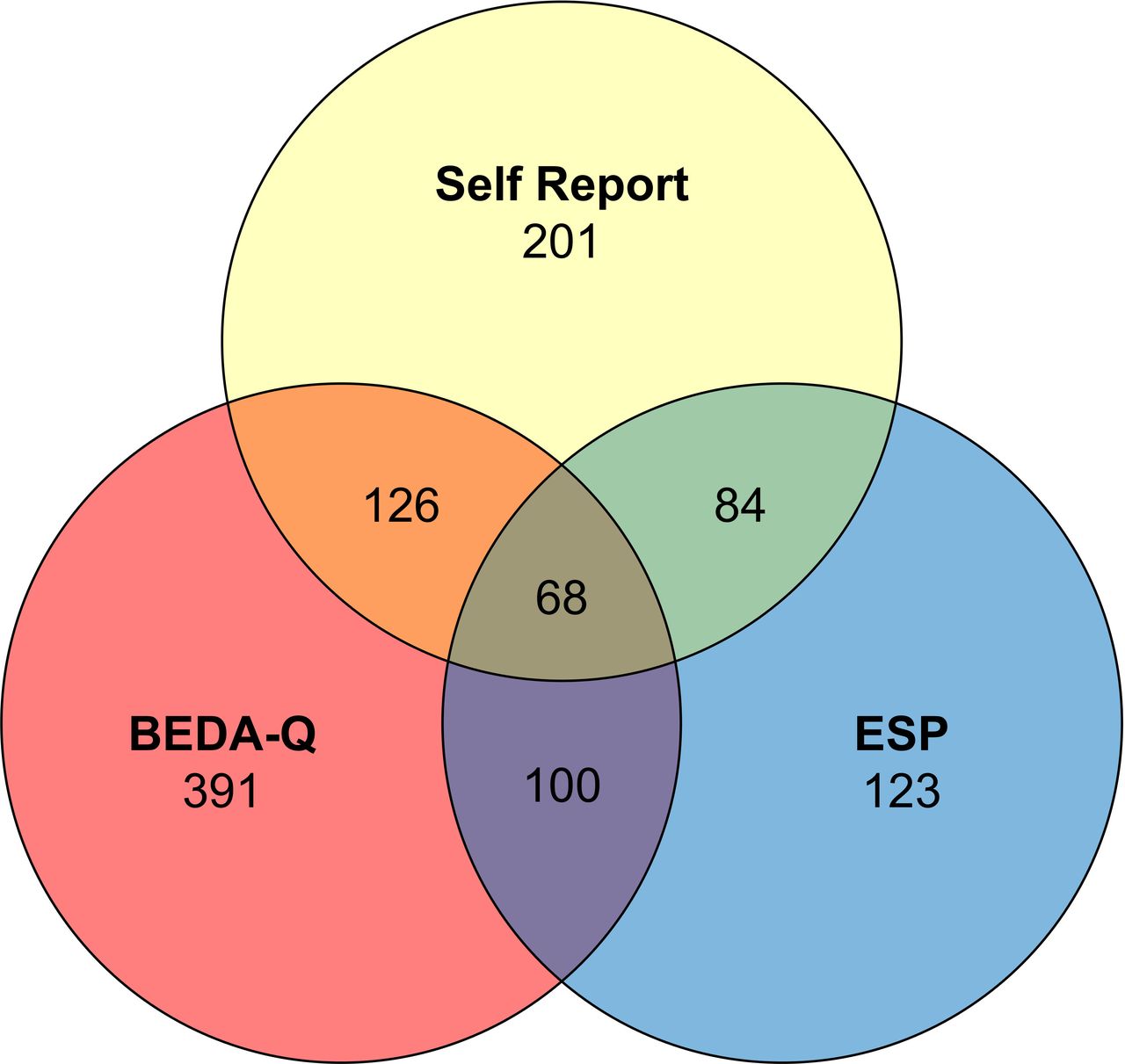
Distribution of participants categorised as low EA by screening tools. Non-overlapping areas represent all participants who were categorised as low EA using that test. Overlapping areas represent the subset of participants who were categorised by two or more tests. Sixty-eight participants met the low EA criteria for all three tests.
Health consequences
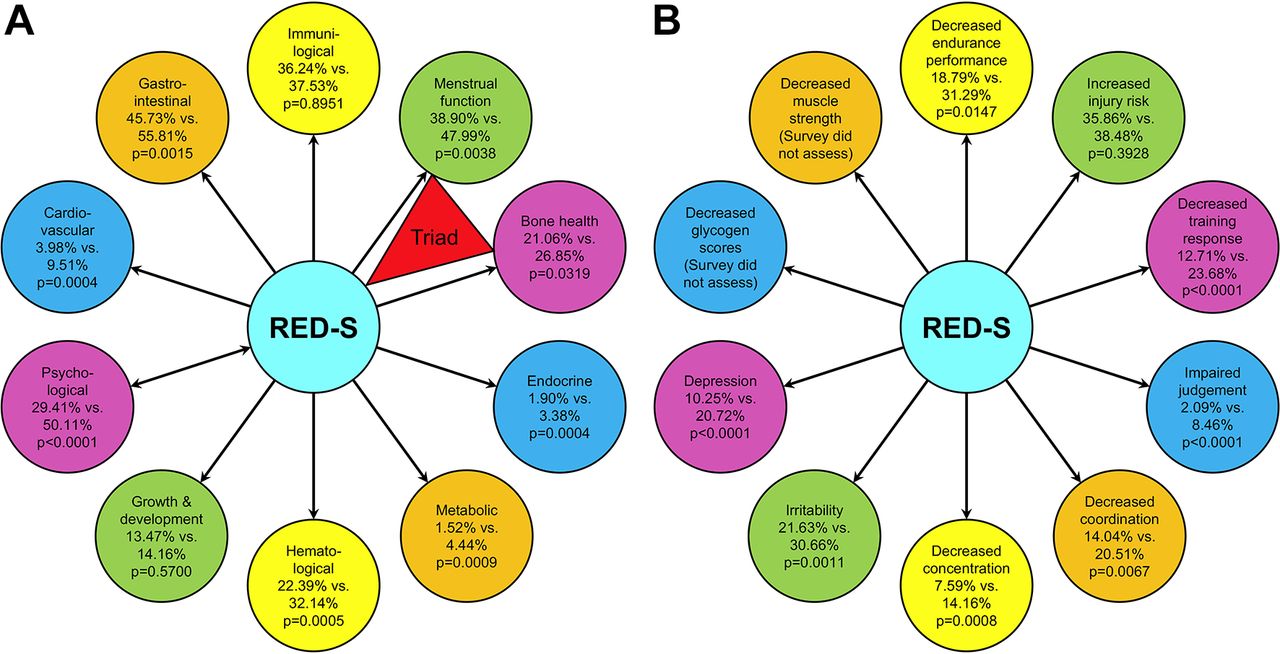
Using the conglomerate definition of low EA, the low EA group had a higher prevalence of menstrual dysfunction, impaired bone heath, endocrine abnormalities, metabolic impairment, haematological abnormalities, psychological disorders, cardiovascular symptoms and gastrointestinal symptoms (figure 2A; P<0.05). No differences in growth and development or immunological function were found between EA groups (figure 2A; P>0.05). Similar results were observed in subset analysis evaluating each health outcome in the three ED/DE screens separately and when grouped into two screen combinations (data not shown). The only exception was using BEDA-Q as the only screening measure for low EA. This analysis did not demonstrate differences between low and adequate EA in bone health, growth and development, and immunological function, and metabolic impairment only trended higher in the low EA versus adequate EA group (3.58% vs 2.46%, P=0.064).

{kind=link}
{kind=link}
(A) The prevalence of potential health-related RED-S consequences in those with and without ED/DE/high BEDA-Q/ESP score (surrogates for low EA/RED-S). Prevalence expressed as % of adequate EA with health consequence versus % of low EA with health consequence. (B) The prevalence of potential performance-related RED-S effects in those with and without ED/DE/high BEDA-Q/ESP score (surrogates for low EA/RED-S). Prevalence expressed as % of adequate EA with performance consequence versus % of low EA with performance consequence.
The likelihood of suffering various health consequences with low EA is shown in table 2. Athletes with low EA were three times more likely to suffer metabolic issues, more than 2.5 times more likely to suffer cardiovascular issues, 2.4 times more likely to report a history of psychological issues, 1.6 times more likely to report a history of haematological issues and nearly 1.5 times more likely to report gastrointestinal issues compared with adequate EA athletes.
Odds of negative health consequences in low EA versus adequate EA
Performance effects
Athletes with low EA had a greater prevalence of decreased training response, impaired judgement, decreased coordination, decreased concentration, irritability, depression and decreased endurance performance compared with the adequate EA group (figure 2B). No evidence of a difference in injury rate was found between low and adequate EA groups (figure 2B). These results largely held when each ED/DE screen was analysed separately and when grouped into two-screen combinations (data not shown). The only exception was BEDA-Q: this analysis identified no difference between groups for endurance (low EA 21.48%, adequate EA 18.72%, P=0.284) or injury (low EA 39.39%, adequate EA 35.63%, P=0.231). Subset analysis using BEDA-Q in combination with ESP found no evidence of a difference between groups for injury, but trended toward a difference in endurance (low EA 22.46%, adequate EA 17.92%, P=0.08).
The likelihood of experiencing these performance effects when low EA is present is shown in table 3. Compared with adequate EA, low EA athletes were 2.1 times more likely to report a decreased training response, 4.3 times more likely to report judgement impairments, 1.6 times more likely to report feeling uncoordinated and two times more likely to report problems concentrating. Athletes with low EA were also 1.6 times more likely to report feeling irritable, 2.3 times more likely to report feelings of depression and nearly 1.5 times more likely to report a decrease in endurance when partaking in sports and/or training compared with adequate EA.
Odds of negative performance effects in low EA versus adequate EA
Discussion
To our knowledge, this is the first study to assess the RED-S model in a clinical population of female athletes and is the largest survey of adolescent and young adult female athletes. Nearly half of all athletes surveyed screened positive for features consistent with low EA according to our criteria. Components of the Triad were clearly associated with our defined measure of low EA. Compared with athletes with adequate EA, athletes with low EA had a higher prevalence of the majority of the IOC-proposed RED-S health and performance consequences.
Low energy availability surrogates and RED-S outcomes
We categorised participants as having low EA by a positive response to any of the three measures (SR, BEDA-Q, ESP). EA has previously been defined as dietary energy intake minus exercise energy expenditure, normalised to fat-free mass,3 28 with each variable requiring accurate measurement for EA estimate. Due to the large size of this study and time constraints surrounding participant recruitment, precise laboratory measurement of EA was not feasible. Instead, we applied a simpler tool to differentiate participants who may have experienced low EA versus those with adequate EA. The use of surrogate markers for low EA has precedence in the literature (eg, the LEAF-Q).25
Our surrogate markers for low EA were not specific to the type of ED/DE assessed. The DSM-5 provides diagnostic criteria for eight different feeding and eating disorders, most of which lead to inadequate nutritional intake.29 Even bulimia nervosa and binge eating disorder are commonly accompanied by fasting or purging behaviours, such as vomiting, laxative abuse or excessive exercise, to compensate for bingeing episodes.29 The majority of our respondents who reported binge eating behaviours also specifically reported limiting food intake, following a restrictive diet, or currently or previously trying to lose weight.
Our method of categorising athletes who scored positive on any of the ED/DE tools as low EA may have included athletes at risk for low EA as opposed to only those of confirmed low EA status, possibly overestimating the number of respondents in the low EA group. To account for this, statistical modelling was performed on each measure individually and in combination with other measures. Both collectively and individually, the screening tools led to findings of more health and performance detriments in the low versus adequate EA group.
Overall, low EA was associated with the majority of RED-S health consequences, irrespective of the tool used to assess low EA (figure 2A). The relationships between low EA and Triad components are well established,3 4 and this study supports that model. While there is less evidence supporting the other RED-S health consequences,5 our study supports the proposed associations between low EA and endocrine,30 31 metabolic,32 haematological,7 psychological,12 33 cardiovascular34 and gastrointestinal impairments35 of the RED-S model. Specifically, risks of metabolic, psychological and cardiovascular issues were more than two-fold greater in those with low EA than those with adequate EA.
Compared with identifying participants with low EA using SR, ESP or a combination of tools, when low EA was measured solely using BEDA-Q, deficits in coordination and endurance performance were not observed. Of the three tools used, BEDA-Q was most inclusive (figure 1). BEDA-Q was designed specifically for female athletes and is a more in-depth ED screening tool than ESP and SR, including more questions about body image and perfectionism. Participants who screened positive only on BEDA-Q may be early in their disorder and have less severe EA deficits, that if left untreated, may cause more RED-S consequences.
Low EA was strongly associated with all assessed RED-S performance effects surveyed except increased injury risk (figure 2B). To date, the performance effects of RED-S have not been studied extensively in athletes.15 36 A 12-week study of 10 elite junior swimmers found sport performance declined in those with ovarian suppression secondary to energy deficit;14 identifying the exact cause for reduced performance is difficult. Our results support that low EA is associated with negative impacts on multiple performance domains and further research is needed to understand mechanisms contributing to these deficits.
In a study of 311 female high school athletes, those with current or past DE were found to be twice as likely to incur an injury during their season.37 While our study did not support these findings, our population may have led to selection bias in relation to this question. All participants were athletes presenting to a sports medicine clinic with a medical or surgical complaint. Additionally, we did not grade responses according to injury severity or duration of time missed, but instead used the number of distinct injuries leading to time loss within the last year. Quantifying injury rate by time loss has been reported to underestimate the number of injuries sustained by athletes.38 39 Accurate recollection of injuries over the course of 1 year may be subject to recall bias. The combination of these factors likely confounded the injury findings in this study. Of note, the low EA group had a higher prevalence of bone health consequences. This question included the number of lifetime bone stress injuries, which was higher in low versus adequate EA athletes.
Low EA was observed in 47.3% of the sample of female athletes participating in a wide variety of sports presenting to a sports medicine clinic. ED/DE prevalence in sports populations has been estimated to range from 6% to 45% in female athletes.40 Our participants presented with various chief complaints, including musculoskeletal injuries, concussion and Triad/RED-S components, to sports medicine practitioners of diverse medical and surgical backgrounds. Our clinic has over 20 practitioners, including a sports endocrinologist who specialises in treating female athletes with Triad/RED-S. When patients seen by the endocrinologist for any complaint were removed from the analysis, low EA was observed in 46% of the sample, highlighting the pervasiveness of low EA in a female sports medicine patient population.
The low EA group had a significantly higher mean BMI than the adequate EA group, illustrating that low EA is not always visible to the eye of the clinician. Body composition may be an important component of understanding an athlete’s EA status: an athlete with a normal BMI but very low percent body fat may be at risk for low EA. Fast, accurate, non-invasive and inexpensive measurements of body composition could aid trainers and physicians in screening female athletes for low EA.
Limitations
Our sample was primarily Caucasian and the age range was 15–30 years: this may limit generalising results to different ethnicities and ages. Using ED/DE screening tools as surrogates for low EA is not a validated method for diagnosing RED-S. The study design was cross-sectional using self-report, which can introduce bias. Many health and performance outcomes can be more accurately assessed with laboratory/imaging confirmation and exercise testing, although this is difficult to do for a large population. Despite these limitations, our large sample size (n=1000) and use of validated questionnaires when available allowed us to establish associations of RED-S with its components in a population of female athletes. Modelling separate and combined measures for low EA had good agreement for most health and performance outcomes.
The IOC’s RED-S concept and diagrams, expanding the emphasis to other systems beyond the reproductive and skeletal, have raised debate and interest within the field.17 41 The RED-S models do not explain causative pathways or related interactions. Some of the outcomes in the models have little athlete research data to date to support their inclusion and there is much that remains to be elucidated regarding the mechanistic effects of low EA on health and performance in a variety of sports populations. Future work should investigate the components of RED-S in a controlled setting to understand associations identified in this study based on self-reported data. In support of the Olympic movement,42 which promotes nondiscriminatory improvement of healthcare of athletes, future investigations should include males, females, athletes of different races and cultures, and athletes with disabilities in their recruitment.16 18
Conclusion
Our study demonstrates that low EA – the central component of RED-S – is associated with many of the health and performance consequences depicted in the RED-S models.5 Further prospective work is needed to better measure and define such effects of low EA and to understand the pathophysiology to guide management and treatment of RED-S.
What are the findings?
In the largest survey of adolescent/young adult female athletes, 1000 girls/women completed online questionnaires and were classified as having low or adequate energy availability based on answers to eating disorder/disordered eating questions.
Those with low energy availability had greater odds of many of the negative health consequences of RED-S (menstrual dysfunction, poor bone health, metabolic issues, haematological detriments, psychological disorders, cardiovascular impairment and gastrointestinal dysfunction) compared to those with adequate EA.
Those with low energy availability were more likely to have experienced many of the negative performance effects of RED-S (decreased training response, impaired judgement, decreased coordination, decreased concentration, irritability, depression and decreased endurance performance).
How might it impact on clinical practice in the future?
Athletes should be screened for low energy availability in order to prevent associated health consequences and performance effects.
Using a survey tool in clinical practice may help uncover risk factors for low energy availability and RED-S.
Findings from this study may encourage more research into clinical markers for RED-S outcomes.
Acknowledgments
Thank you to the patients and providers of the Division of Sports Medicine at Boston Children’s Hospital for their participation and interest in this project and to Elizabeth Koch for her assistance with data collection.
References
Footnotes
Contributors KEA: Conceptualisation of project, survey development, drafting and revision of manuscript, confirmation of final version to be published. BH: Contributions to data analysis, drafting and revision of manuscript. KMC and EFF: Contributions to data collection, revision of manuscript. GB: Contributions to advanced statistical analysis, drafting and revision of manuscript. AST: Contributions to survey development and revision of manuscript. KLP: Contributions to survey development, statistical consultation, drafting and revision of manuscript. AJS: Statistical consultation, drafting and revision of manuscript. ALP: Survey development and implementation, directed data collection, drafting and revision of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study was approved by the Boston Children’s Hospital Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No unpublished data were used in the preparation of this manuscript.