Article Text

Abstract
Bipolar and psychotic disorders are relatively common and likely to have a significant impact on quality of life and functioning which, in the context of elite sport, includes a potential negative impact on sporting performance. For this narrative review article, the literature on bipolar and psychotic disorders in elite athletes was comprehensively searched, and little empirical research was found. A diagnosis of bipolar or psychotic disorders may be challenging in elite athletes because of complicating factors related to the modifying role of exercise and potential precipitating impact of substance use. Medications used to treat bipolar and psychotic disorders may have side effects particularly problematic for elite athletes. Future research should be tailored to the specific characteristics and needs of elite athletes and to the sporting context in which the disorders may arise. Specifically, further research is needed on the prevalence and incidence of these conditions in elite athletes and the impact of both the disorders and their treatments on sporting performance.
- psychiatry
- disorder
- athlete
- sport
- elite performance
Statistics from Altmetric.com
Introduction
The typical age of onset of bipolar and psychotic disorders coincides with average peak performance in elite athletes,1 yet information on their prevalence in elite athletes and their impact on athletic performance is limited. Furthermore, evidence to guide the clinician who is providing treatment for these conditions in elite athletes is primarily based on ‘expert opinion’ and extrapolation from general (non-sporting) guidelines.
The purposes of this narrative review are to: (A) synthesise the literature on the diagnosis, prevalence, impact on performance and management of bipolar and psychotic disorders in elite athletes; and (B) provide recommendations based on what is currently known. One of the authors (MEH) searched key databases (PubMed, SportDiscus, PsycINFO, Scopus and Cochrane) and repeated the searches in November 2018 (3 months before intended submission). Figure 1 illustrates the search strategy. Search terms relating to the disorders, sports participation and the elite nature of participation were combined. We identified 420 potential references and included original studies that: (A) were written in English; (B) were conducted exclusively among current elite athletes; and (C) presented information on bipolar or psychotic disorders. Twelve references were retained based on these inclusion criteria. These were then used by the other authors to identify related references. Other literature was also reviewed, where there were gaps in athlete-specific literature, for guidance on diagnosis, prevalence, functional impairment and management. Elite athletes were defined as those competing at professional, Olympic or collegiate/university levels.
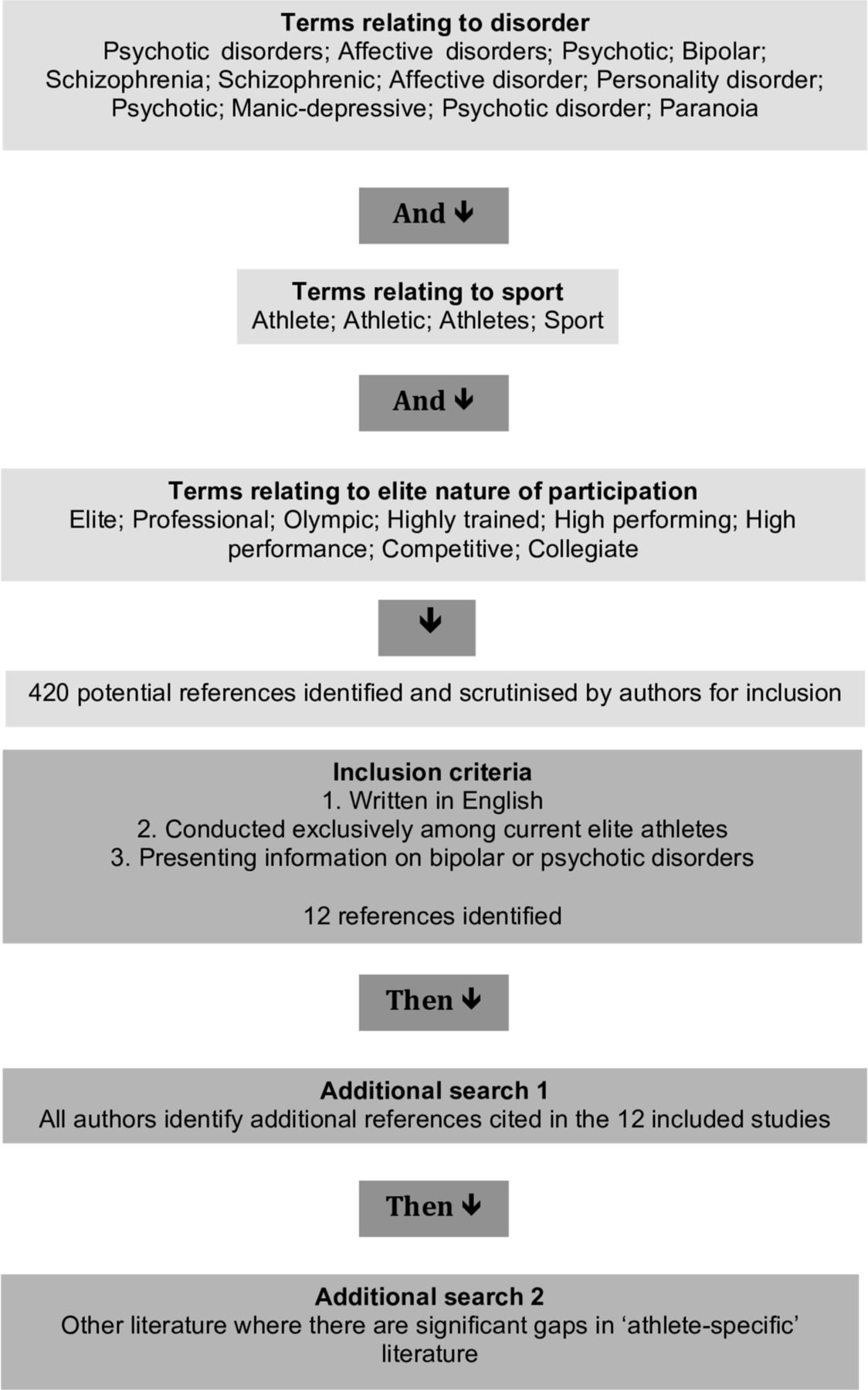
Search strategy.
Diagnosis of bipolar disorder
Bipolar disorder is a recurrent and often chronic mental health disorder. It is characterised by episodes of elevated mood (‘mania’, or when less severe, ‘hypomania’) and also commonly of depressed mood, with associated change in functioning.2
Mania is characterised by an abnormally and persistently elevated, expansive or irritable mood and disinhibited behaviour.2 Increased energy and reduced need for sleep are typical, and insight is frequently diminished. Psychotic symptoms such as delusions or hallucinations can occur and, if present, are usually consistent with the individual’s elevated mood (‘mood congruent’). Symptoms of mania must be present for at least 7 days and associated with significantly impaired function to permit diagnosis of a manic episode. Lesser degrees of functional impairment, or simply a change in functioning without impairment, for at least 4 days are consistent with a diagnosis of a hypomanic episode.2 Episodes of mania and hypomania tend to be less frequent, and shorter, than depressive episodes.3 4
Episodes of depression are characterised by some or all of the following: low mood; loss of interest or pleasure; reduced energy; changes in sleep and appetite; feelings of guilt or worthlessness; thoughts of death or suicide; psychomotor agitation or retardation; and poor concentration.2 Symptoms can last for weeks or more. For diagnostic purposes, a minimum of five symptoms and duration of 2 weeks is specified for a major depressive episode. If psychotic symptoms are present, they are usually congruent with the individual’s depressed mood.
Features of both hypomania or mania and depression can be concurrent (described as having ‘mixed features’).2 For example, an individual may exhibit increased activation and social disinhibition, but be dysphoric in mood. This combination may appear counterintuitive, but it is more common than often recognised.5 Individuals in such states are at particularly high risk for suicide.6
Two main specific subtypes of bipolar disorder are recognised.2 In bipolar I disorder, there has been at least one manic episode (with or without episodes of major depression); in bipolar II disorder, hypomanic and major depressive episodes have occurred, with no periods of mania.
Patients with bipolar disorder (especially bipolar II disorder) may be misclassified as having a purely depressive illness.7 Those with shorter hypomanic episodes and less functional impairment may not present for medical attention, and if no inquiry is made during assessment of a later depressive episode, the diagnosis may be missed.
Diagnosis of psychotic disorders
Psychotic disorders are characterised by symptoms such as hallucinations or delusions. In schizophrenia, additional symptoms are required to make the diagnosis, including some or all of the following: disorganised speech; grossly disorganised or catatonic behaviours; negative symptoms such as lack of motivation; and associated features such as inappropriate affect, cognitive deficits and problems with social cognition. The diagnosis is only made if some symptoms have persisted for at least 6 months and significant functional impairment exists.2
Other psychotic disorders are described and classified2 and their features are summarised in table 1. In delusional disorder, there is a narrower range of symptoms (primarily delusions). In brief psychotic disorder, the duration is shorter than in schizophrenia. In schizophreniform disorder, the duration is shorter and there is less functional impairment (often a provisional diagnosis). In schizoaffective disorder, mood symptoms occur alongside, and sometimes separate from, psychotic symptoms and may be primarily depressive or manic. Attenuated psychosis syndrome is not an official Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnosis but is noted within the DSM as a Condition for Further Study,2 with manifestations that reportedly include delusions, hallucinations or disorganised speech in attenuated (or subthreshold) form but still sufficient to be distressing or disabling. A proportion of individuals with attenuated psychosis syndrome will progress to a full psychotic syndrome,8 even when symptoms appear to have resolved.9 Individuals with attenuated psychosis syndrome are at risk for developing many non-psychotic disorders that may need treatment, particularly given their associations with suicidality.10 11
Schizophrenia and psychotic disorders2
Secondary bipolar and psychotic disorders
Substance/medication-induced bipolar disorder and bipolar disorder due to another medical condition are secondary bipolar disorders.2 Similarly, psychotic symptoms may also be substance/medication induced or due to another medical condition.2 Within the general population, some of these secondary disorders are more commonly a consideration when there is a later age presentation12 as they may be associated with conditions such as thyroid disease, multiple sclerosis and right-sided cortical or subcortical brain lesions, which are more common in older populations.13 Of more relevance in sporting populations are traumatic brain injuries, where secondary bipolar disorder is a possible although uncommon sequela,14 and stimulant or anabolic androgenic steroid (AAS) use contributing to depressive or hypomanic symptoms, an unstable mood or psychotic symptoms.15–17
Sports-specific diagnostic issues
A diagnosis of bipolar disorder or a psychotic disorder may be more difficult to make in an elite athlete. Exercise may be an outlet for the excess energy seen in mania or hypomania, which could delay diagnosis. In addition, overactivity may be obscured or normalised in the context of athletic training.18 AAS may be misused by athletes for performance reasons16 19; the mood disturbance and psychotic symptoms that have been reported in association with their use can confuse diagnosis. Importantly, though, hypomanic symptoms secondary to AAS are usually subsyndromal and typically only seen when high doses of multiple agents are used (often called ‘stacking’).17 20 Depressive symptoms have been described among athletes withdrawing from AAS use.17 20 Again, there is an association between high dosages and ‘stacking’ and depression.20 21 However, many studies of this topic had small sample sizes, no control groups, multiple potential confounders and cross-sectional designs. Other substances used by some athletes—including stimulants, cannabis and glucocorticoids—may be associated with psychotic symptoms.16 19 It is important to distinguish primary mood and psychotic disorders from substance-induced forms, as the latter may be self-limiting or require only short-term treatment.21 A comprehensive history—supplemented by appropriate urine testing and toxicology—is necessary to confirm the diagnosis.22 Table 2 provides a list of features that may help distinguish between primary bipolar and psychotic disorders and those secondary to substance misuse by elite athletes.
Features that may help distinguish between primary bipolar and psychotic disorders and those secondary to substance misuse in sport17 19–22
Assessment
For an elite athlete who may have bipolar disorder, the standard assessment begins with a detailed history of mood episodes, triggers and symptoms between episodes, with corroboration from a family member or other close informants if possible.23 A detailed history includes all medications (and any supplements or ergogenic aids) and will help diagnose common comorbidities such as anxiety disorders and other conditions that may confound the diagnosis. These include personality disorders, attention-deficit/hyperactivity disorder, illicit or prescribed drug use or use disorders, and medical conditions associated with secondary mania or secondary psychosis.13 23 24
The role of exercise in an athlete’s symptoms needs to be considered when assessing for bipolar disorder. Less frequent exercise is often associated with depression, and more frequent exercise with mania25; the amount of exercise may be a manifestation of the disorder.
Bipolar disorder is unusual compared with other mental health disorders in that regular exercise does not seem to offer a protective effect. In a large prospective community survey, the incidence of bipolar disorder over a 4-year period was greater in those with regular physical activity at baseline.26 Furthermore, although some patients with bipolar disorder report that exercise is helpful in mood regulation, directing energy and bringing structure to activities, others report that it contributes to spiralling of hypomanic and manic symptoms.27 The type of sport and the nature of the physical activity may be relevant. Rhythmic sporting activities (eg, running, walking and swimming) may be calming and facilitate mood regulation.27 Conversely, participants in extreme or high-risk sports (eg, mountain biking or rock climbing) report high scores on measures of bipolar symptoms.28
When considering the role of exercise in the development of hypomanic and manic symptoms, some possible mechanisms have been described. Exercise and antidepressant medication may share similar biological mechanisms29 and thus may induce hypomania and mania in patients with bipolar disorder.30 In addition, neurobiological systems involved in goal striving and reward seeking (principally dopaminergic projections) may be dysregulated in those with bipolar disorder.31 If there is such an underlying vulnerability in an individual engaged in performance sport, striving towards the sporting goal and seeking rewards through sport could act as a trigger for manic or hypomanic symptoms.32
In the assessment process, it may therefore be necessary to consider whether sporting activity is a manifestation of the underlying disorder, a helpful way of managing symptoms or a contributory factor to mood instability and especially to hypomania and mania.
Psychotic symptoms are experienced by 5%–8% of the general population33 and 7.5% of 13–18 year-olds.10 Since these symptoms do not necessarily predict overt psychotic disorders, careful assessment is warranted. The self-administered 16-item Prodromal Questionnaire34 may be a useful screening tool for psychotic disorders (table 3). The respondent indicates for each item whether this experience is ‘True or False’ and indicates how much distress is associated with each ‘True’ item, on a Likert scale of 0–3. A score is determined by summing the number of items endorsed as ‘True’. A score of 6 or more has optimal sensitivity (87%) and specificity (87%)34 and indicates the respondent may be at risk for psychosis. Athletes who meet this cut-off, or who otherwise disclose concerns about psychotic-like symptoms, should be referred to a specialist mental health service for a more detailed clinical history.35 There are no sports-specific psychosis screening tools.
The 16-item version of the Prodromal Questionnaire (PQ-16) by permission of the Oxford University Press34
If a psychotic disorder is suspected for the first time, rapid assessment by a specialist mental health service is indicated.35 The assessment should include a careful evaluation of symptoms, a psychosocial assessment and a risk assessment.35 36 Conditions that can cause secondary psychosis (eg, substance use disorders) should also be investigated as indicated. If medication is required, then medication choice will be influenced by both comorbid medical conditions such as renal or hepatic disease and by anticipated side effects such as dyslipidaemias, impaired glucose tolerance, hyperprolactinaemia and QTc prolongation. For these reasons, preliminary investigations often include renal and liver function tests, a metabolic profile (height, weight, blood pressure, and lipid and glucose profiles), prolactin levels and an ECG.36
Prevalence
The lifetime prevalence of bipolar disorder in the general population is approximately 0.4% for type I and 0.6% for type II; subthreshold symptoms are more common at around 1.4%.37 Lifetime prevalence of schizophrenia and related disorders is thought to be around 0.5%, but with regional variations.38 To date, there are no reliable prevalence data on either bipolar or psychotic disorders in elite athletes.39–41 However, schizophrenia seems to be under-represented in elite athletes.42 The late teens and early 20s are the peak age of performance in many sports, and close to the peak age of onset of conditions such as bipolar and psychotic disorders.1 Thus, it would be expected that elite athletes could present with either condition, if only by coincidence.
Impact on performance
Case reports of high-profile athletes with bipolar disorder indicate that the condition is not incompatible with sporting success.43 In addition, bipolar disorder is episodic, with relatively euthymic periods in-between symptomatic episodes.3 4 When hypomanic, an athlete’s training might not be unduly compromised, and functional impairment is not always found at this stage.2 However, as symptoms increase, concentration, decision-making and organisation are affected with associated functional impairments, including difficulty participating in sport, exercise and physical activity.44 Vigorous exercise may even precipitate or perpetuate mania in bipolar disorder,45 such that elite athletes with bipolar disorder may be limited in the maximum amount of exercise they can safely undertake without risk of mood destabilisation. This situation can be problematic when insight becomes impaired, as it often does in emerging mania, and individuals may be reluctant to respond to advice to change behaviours and activity patterns because they perceive no need to do so.
Although bipolar disorder is an episodic illness, individuals can expect to spend significant amounts of time in a symptomatic state. In one survey over an average of 12.8 years, those with bipolar I disorder spent 47.3% of the time experiencing symptoms. Depressive symptoms were the most common (39% of the time) but were often subsyndromal.4 A similar survey reported that individuals with bipolar II disorder were symptomatic 53.9% of the time, over an average of 13.4 years, with depressive symptoms the most common (50.3% of the time).3
Approximately 40% of people with bipolar disorder have some associated cognitive impairment.46 All cognitive domains are affected (including attention, executive function and memory), even when mood symptoms are relatively absent.47 The severity of impairment seems greatest in those suffering from type I bipolar disorder and in those with psychotic symptoms,48 but in general is not as problematic as in schizophrenia.49 There is promise that early initiation of effective treatments may prevent or attenuate cognitive deficits.50
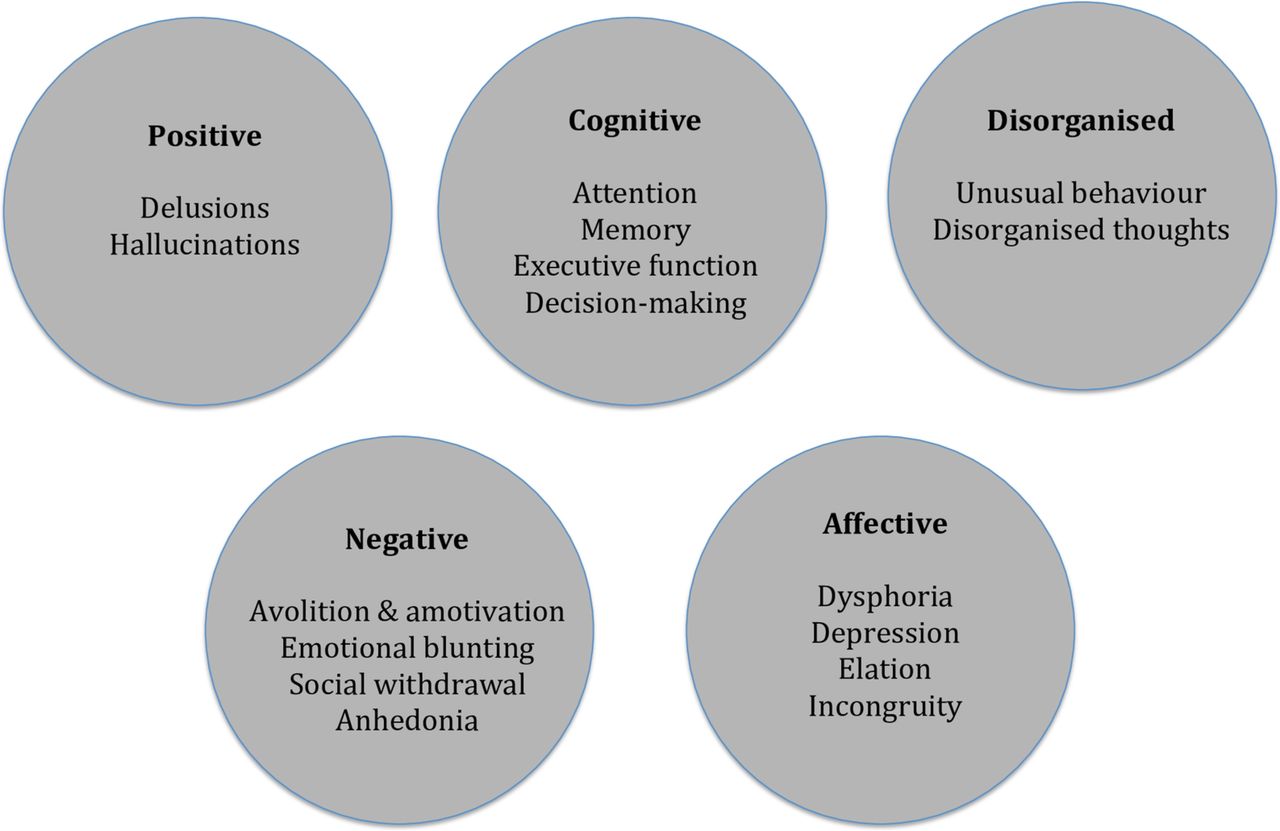
Symptoms in schizophrenia (and related psychoses) are often grouped into domains and five are illustrated in figure 2. Although some people with schizophrenia can expect a good outcome, a significant number will experience a more chronic and pervasive course with a resultant impact on sporting, academic, employment and social function. Symptoms in the cognitive and negative domains are primarily associated with functional impairment.51 52 Longer term symptoms in the negative domain, especially avolition and amotivation (lack of initiative for purposeful tasks), may negatively impact significantly on commitment and ability to sustain elite-level sports participation. Difficulties with executive function and working memory would be expected to impair ability to pursue most activities requiring processing speed and complex execution, including elite sports performance. Schizophrenia is thus likely to interfere with the demands of elite athletes for both training and competition. That this condition appears to be under-represented among elite athletes may relate to these issues.42
{kind=link}
{kind=link}
Symptom domains in schizophrenia.
Management
Delayed treatment of bipolar disorder53 and long-standing untreated psychosis54 both correlate with a worse outcome.
Clinical staging55 offers a longitudinal perspective of bipolar and psychotic disorders, from an at-risk state (ie, no symptoms), through attenuated or subthreshold syndromes, to first and potentially subsequent episodes. In subthreshold stages, psychological interventions and regular monitoring are recommended.56 Mood-stabilising or antipsychotic medication is typically reserved for the first episode of a diagnosed disorder, given the side effect profile of these medications.57
Exercise and psychotherapy interventions
Although individuals with bipolar and psychotic disorders may have difficulties sustaining high-level sports performance, there are potential benefits to continuing recreational exercise and sport. Adolescent athletes report multiple mental health benefits of sports participation, especially in team sports.58 Moderate levels of physical activity may also benefit symptoms of bipolar and psychotic disorders,45 59 60 although there remains a relative lack of research on the relationships between high-volume and high-intensity athletic training and symptoms of bipolar disorder or psychosis. Exercise can help former athletes diagnosed with psychosis to establish a new sense of self and purpose in recovery.61 Maintaining activities contributes to the experience of recovery that includes finding meaning in and developing a sense of agency, identity and engagement with life.62 Many individuals experiencing psychotic disorders encounter challenges with relationships and broader social inclusion; in such cases, physical activity and sports participation can help individuals sustain functioning.63
Hippocampal volume is lower than expected in individuals diagnosed with either bipolar disorder or schizophrenia,64 but can be increased by exercise in both patients and healthy controls, with associated improvements in cognitive function.65 Exercise may also improve neuroplasticity and promote neurogenesis in affected individuals; in addition, cardiorespiratory fitness may attenuate the changes in brain volume among those with schizophrenia.66 However, it is unknown if improved cognitive function or degree of attenuation can prevent illness progression so that an athlete could sustain an elite level of performance. Exercise may also reduce disrupted circadian rhythm and sleep patterns67 in both schizophrenia68 and bipolar disorder.69 At present, exercise and physical activity do not feature in the practice guidance for either bipolar disorder or schizophrenia in the UK or USA.23 24 35 36
Psychoeducation is recommended for bipolar disorder,23 24 and has the best evidence among all psychotherapy interventions for bipolar disorder within the general population.70 Educational components include information on the nature of the illness, factors that can cause destabilisation, use of long-term medications and the appropriate use of short-term medications and other strategies to address early signs of relapse. Interpersonal social rhythms therapy also reportedly sustains function in bipolar disorder.71 72 Other psychotherapy interventions that may be useful in bipolar disorder include cognitive–behavioural therapy, interpersonal psychotherapy for bipolar depressive symptoms and family interventions, although much of the evidence is extrapolated from patients with unipolar depression23 24 and none is specific to elite athletes.
Psychotherapy interventions such as cognitive–behavioural therapy and family interventions are also recommended for psychotic disorders,35 36 but again there is no sports-specific evidence on which to base such treatment in athletes. While family psychoeducation has fairly strong evidence for schizophrenia, that this intervention often consists of regularly occurring group meetings may be incompatible with elite athletes’ travel schedules and desire for confidentiality.
Medication management
There is limited evidence regarding medication treatment of bipolar disorder and psychotic conditions in athletes39–41; guidance comes primarily from extrapolation from general population recommendations, and from expert opinion regarding athlete prescribing. Overall, an approach of ‘carefully considered individual prescribing’ is recommended.73 One important element of this is to consider the potential negative impact of medication side effects on athletic performance.73 74 This is accompanied by the need to understand the impact of an athlete’s physiological stressors on both pharmacodynamics (the effect of the drug on the athlete) and pharmacokinetics (how the athlete’s body handles the drug).73 74
Guidance for the treatment of bipolar disorder needs to address acute mania/hypomania, acute depression, mood episodes with mixed features and long-term prophylactic treatment to minimise recurrence.13 23 24 During acute mania, antipsychotics can have a rapid antimanic effect and may be augmented with short-term benzodiazepines.13 23 24 First-generation (eg, haloperidol) and second-generation (eg, aripiprazole, lurasidone, olanzapine, quetiapine, risperidone, ziprasidone) antipsychotics can be used, with some guidance for the general population preferring second-generation drugs.24 Aripiprazole is recommended as the first choice in the general adolescent population because of its more favourable metabolic profile,23 which may be a consideration relevant to elite athletes as well. In those with less severe mania, monotherapy with valproate or lithium can be considered,24 although valproate should typically not be used in women of childbearing age, an age group into which most elite female athletes fall. For those who relapse while prescribed medication, it is helpful to begin by assessing treatment adherence and optimising existing treatments (eg, by checking lithium or valproate blood levels and increasing dosages if necessary).13 23 24 When mixed features are present, guidance suggests following treatment as for acute mania.13
In the depressive phase of bipolar disorder, optimising existing treatments is also recommended.13 24 Quetiapine, lurasidone, and olanzapine plus fluoxetine are particularly evidence-based choices in the general population.13 Lamotrigine also has efficacy,75 but requires slow titration over weeks. The evidence for lithium is more equivocal in acute treatment, but it is recommended if there is previous evidence of effectiveness,13 and it is more likely to be efficacious when combined with lamotrigine.76 Antidepressants have generally not been proven effective in treating bipolar depression.77 If an antidepressant is used, some individuals appear to respond to selective serotonin reuptake inhibitors, which appear to be less likely to cause a switch into mania than serotonin and norepinephrine reuptake inhibitors78 and tricyclic antidepressants.79 Regardless, antidepressants should be used cautiously and typically only in combination with a long-term antimanic treatment, especially for individuals with bipolar I disorder.13
For prophylaxis of future mood episodes in bipolar disorder within the general population, lithium is a usual first-line treatment and has efficacy in preventing relapse into either mania or depression.13 23 24 Quetiapine may reduce long-term depressive and manic relapses.80 Lamotrigine is more effective at preventing depressive relapses, while valproate and antipsychotics such as aripiprazole, lurasidone, olanzapine and risperidone are more effective for preventing manic relapses.13 23
Data on medication recommendations specifically for athletes with bipolar disorder are largely limited to expert opinion. Lithium and lamotrigine can be used by athletes, and sports psychiatrists have expressed preferences for these two drugs.81 Lithium has a narrow therapeutic window and requires careful monitoring, especially in athletes.73 Data on impact of exercise on lithium levels are preliminary and mixed. Sweat loss may lower lithium levels below therapeutic levels,82 83 but there is also concern that dehydration may raise levels towards toxicity.74 Lamotrigine, unlike many other medication options, does not cause weight gain and might be chosen for this reason.73 81 Among the second-generation (atypical) antipsychotics, aripiprazole, lurasidone and ziprasidone may be relatively less likely to cause sedation and weight gain, often considered problematic for athletes.73 81 Ziprasidone may cause QTc prolongation84 and thus may not be a first-line choice within this class for elite athletes.81 Quetiapine can be considered but is sedating for many, and aripiprazole may cause akathisia, which could negatively impact motor function and elite sporting performance.73
Within the general population, the mainstay of pharmacological treatment in an established and sustained psychotic illness is either first or second-generation antipsychotic medication, with clozapine reserved for treatment-resistant cases.35 36 85 Some guidance suggests choosing a drug based on the side effect profile, noting that first and second-generation drugs are broadly equal in efficacy.35 85 Other guidance recommends using second-generation antipsychotics preferentially unless there has been a good previous response to a first-generation drug.36
When offering treatment for athletes with psychosis, guidance again comes primarily from expert opinion. First-generation (typical) antipsychotics are an infrequent choice because of sedation, motor side effects and cardiac concerns,81 and the considerations when choosing a second-generation drug are similar to those described above in relation to bipolar disorder.
No pharmacological treatments approved for either bipolar or psychotic disorders require a Therapeutic Use Exemption (TUE). On occasion, beta-blockers have been used to manage tremor as a side effect of lithium therapy or akathisia as a side effect of antipsychotics; a TUE would be required for this treatment in certain sports and situations.86 Possible pharmacological treatments for athletes are summarised in table 4.
‘Sports specific’ medication options in bipolar disorder and psychosis73 74 81
Summary
Bipolar and psychotic disorders can have a significant negative impact on individuals in the general population, but the prevalence of these disorders among elite athletes is unknown. Cross-sectional studies to identify those with bipolar or psychotic disorder diagnoses are needed, as are methodologically more robust studies describing relationships between performance-enhancing substances and mental health symptoms and disorders. Information on particular symptom manifestations within sporting populations and population-specific screening tools would be especially useful. Although accurate prevalence data on bipolar and psychotic disorders in elite athletes are lacking, those who practise in sport require at least a basic knowledge of these conditions to ensure early identification and facilitate access to treatment, and thus improve outcomes.
Bipolar and psychotic disorders can be chronic and/or relapsing conditions where medication is recommended to restore and sustain health. Although psychotherapy interventions are usually recommended, these non-pharmacological strategies are generally in addition to medications rather than as alternatives. This is unlike treatments for anxiety disorders and mild or moderate depression, where psychotherapy may be an evidence-based alternative, and in attenuated psychosis syndrome, where psychotherapy used without medication may prevent symptom progression. The absence of athlete-specific medication trials is therefore of particular importance. High-quality data on uses of medication at the extremes of human physiology (ie, during intense exercise) and on the performance impact of commonly prescribed medications for bipolar or psychotic disorders are needed. At present, prescribers must rely on expert opinion, using information extrapolated from general population studies and taking into account the athlete’s physiology and the demands of each sport.
Finally, both physical activity and sports participation can have multiple benefits for individuals with bipolar or psychotic disorders. Mental health service providers can ally with the world of sport, exercise and fitness for the benefit of patients and to help improve outcomes for conditions that can be chronic and relapsing. This includes athletes whose illnesses impair their progress and who could be encouraged to maintain activities and, if necessary, given a supported exit strategy from elite-level sport to a lower or more recreational level of activity.
What is already known
Bipolar and psychotic disorder symptoms may be primary, a result of substance/medication use or a result of other medical conditions.
Bipolar and psychotic disorders often have a significantly negative impact on functioning and quality of life.
Individuals with bipolar and psychotic disorders may benefit from early treatment.
Bipolar and psychotic disorders are typically chronic in nature and generally require long-term medication management alongside psychotherapy interventions.
What are the new findings
A diagnosis of bipolar or psychotic disorders may be more difficult to make in an elite athlete because of complicating factors related to the modifying role of exercise and potential precipitating impact of substance use.
Symptoms of bipolar and psychotic disorders may have a negative impact on sport performance and may often be incompatible with elite-level sports participation, though there may be an important role for continued exercise at lower levels of participation even if elite-level competition is not possible.
Medications used to treat bipolar and psychotic disorders may have many side effects particularly problematic for elite athletes, though there is a need for more study of pharmacological options within this population.
More research is needed on the incidence and prevalence of bipolar and psychotic disorders within elite athletes, particular symptom manifestations within this population and population-specific screening tools that might be helpful.
Acknowledgments
The authors thank the other participants in the 2018 International Olympic Committee Consensus Meeting on Mental Health in Elite Athletes, including Cindy Miller Aron, David Baron, Antonia Baum, Abhinav Bindra, Richard Budgett, Niccolo Campriani, Joao Mauricio Castaldelli-Maia, Jeff Derevensky, Lars Engebretsen, Ira Glick, Vincent Gouttebarge, Michael Grandner, Doug Hyun Han, David McDuff, Margo Mountjoy, Aslihan Polat, Margot Putukian, Allen Sills, Torbjorn Soligard, Todd Stull, Leslie Swartz and Li Jing Zhu, for their input on the development and interpretation of this research.
References
Footnotes
Contributors AC, PG, SMR, RP, BH, CLR: substantial contribution to conception and design; acquisition, analysis and interpretation of data; drafting the work and revising it critically. MEH: substantial contribution to conception; acquisition and analysis of data; revising the work critically. RHMW: substantial contribution to design; acquisition, analysis and interpretation of data; drafting the work and revising it critically. All authors gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Competing interests RHMW reports personal fees in the last 3 years from Sunovion, Janssen, My Tomorrows, Lundbeck, Pfizer, LivaNova, Syntropharma, OCM Comunicaziona, American Center for Psychiatry & Neurology (United Arab Emirates), Qatar International Mental Health Conference, British Association for Psychopharmacology, European College of Neuropsychopharmacology, UK Medical Research Council, International Society for Affective Disorders and Wiley. He has received non-financial support from COMPASS and grants from research related to psychotropic drugs from the UK National Institute for Health Research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.