Article Text

Abstract
Background Absolute numbers of head injuries in football (soccer) are considerable because of its high popularity and the large number of players. In 2006 a rule was changed to reduce head injuries. Players were given a red card (sent off) for intentional elbow-head contact.
Aims To describe the head injury mechanism and examine the effect of the rule change.
Methods Based on continuously recorded data from the German football magazine “kicker”, a database of all head injuries in the 1st German Male Bundesliga was generated comprising seasons 2000/01-2012/13. Injury mechanisms were analysed from video recordings. Injury incidence rates (IR) and 95% confidence intervals (95% CI) as well as incidence rate ratios (IRR) to assess differences before and after the rule change were calculated.
Results 356 head injuries were recorded (IR 2.22, 95% CI 2.00 to 2.46 per 1000 match hours). Contact with another player caused most head injuries, more specifically because of head-head (34%) or elbow-head (17%) contacts. After the rule change, head injuries were reduced by 29% (IRR 0.71, 95% CI 0.57 to 0.86, p=0.002). Lacerations/abrasions declined by 42% (95% CI 0.39 to 0.85), concussions by 29% (95% CI 0.46 to 1.09), contusions by 18% (95% CI 0.43 to 1.55) and facial fractures by 16% (95% CI 0.55 to 1.28).
Conclusions This rule change appeared to reduce the risk of head injuries in men’s professional football.
- Soccer
- concussion
- traumatic brain injury
- injury patterns
- epidemiology
- head impact
Statistics from Altmetric.com
Introduction
A unique feature of football (soccer) is the intentional use of the head to play the ball. Head collisions with an opponent player are inevitable with existing rules. Head injuries may also be caused by unintended or unprepared heading the ball, by kicking against the head or by contact between the head and elbow/arm.1–7 Prospective studies on head and neck injuries identified the unfair use of the upper extremity as a significant cause of head and neck injuries.1 8
Based on the analyses of injury mechanisms of head injuries during the FIFA World Cups (1998–2004),8 9 the International Football Association Board (IFAB) altered the law of the game in 2006 so that direct and deliberate ‘elbows to head’ were punished with a red card.
We therefore aimed to (1) describe the most common mechanisms leading to head injuries (in matches only) in elite male football players and (2) measure the effect of the rule change in the 2006/07 season on head injuries.
Methods
Study sample and design
A retrospective analysis of injury incidence rates (IRs) and injury mechanisms of head injuries in the first German Male Bundesliga was conducted for the seasons 2000/01–2012/13. We employed a retrospective comparison between seasons before the rule change and seasons afterwards. The rule change (penalising intentional elbow–head contacts with a red card) was introduced at the beginning of the 2006/07 season. In the present study this season was excluded from the analysis to ensure that referees and players became accustomed to the new rule. The analysis included 34 games per team in the regular season as well as games in official national and international competitions.
Neither Research Ethics Board approval nor the registration on clinicaltrials.gov was required for this study as all data were collected from public sources.10
Data collection
Data collection followed an a priori protocol and analysis plan. Head injuries, including publicly available clinical information (diagnosis and time loss), were identified by a structured search in the German football magazine ‘kicker Sportmagazin’ (all issues available online), which is published twice weekly with one journalist being responsible for one club and having contact with the club every day. The magazine presents injury reports. Additionally, a free-text search with defined search terms was conducted. For those injuries with an unknown outcome (eg, towards the end of the season), the mean time loss for the particular diagnosis in the present database was considered. Only match injuries were analysed. The injury mechanisms were captured on video recordings and analysed by two different investigators (sport scientists).8 10 11 Disagreements were discussed in a consensus meeting with a third investigator (medical doctor). The video recordings were re-evaluated and a final decision was made by the third investigator.1 Head injuries with no video recording available were classified as unknown injury mechanism and accounted for 18%.
Incident assessment
Observational criteria of head impact events during matches are listed in table 1. These defined criteria are in accordance with the analyses of injury mechanisms that have previously been published.8 11 12 Head injuries without video recordings are included in the analyses referring to total numbers and percentages.
Points of measurement for the retrospective analyses of head impact events during matches
Injury assessment
The football magazine ‘kicker Sportmagazin’ provided all relevant data on diagnosis such as concussions/traumatic brain injuries (TBI), contusions, facial fractures, lacerations/abrasions. The diagnoses were forwarded by team officials. Fractures of the zygomatic bone and skull (eg, base of the skull, calvaria and frontal sinus) as well as head contusions (to the skull and zygomatic bone only) were additionally grouped as ‘suspected concussions’ (independent from the original injury). Injuries with an unclear description and unknown diagnosis were categorised as ‘other injury’. In case an injury encompassed more than one diagnosis, the more severe injury was recorded. The severity of injuries was based on the time loss according to the consensus statement published previously13: slight (time loss 0 days); minimal (1–3 days); mild (4–7 days); moderate (8–28 days); severe (>28 days).
Match exposure
Match exposure was recorded via online sources on football statistics and calculated using the following calculation13: number of official games x number of players on the field x duration of the game in hours. Official games included all season games, different cup games (eg, DFB-Cup) and international games (eg, Champions League). Extra time in knock out games was also considered. Games of the national teams were not included.
Inter-rater reliability
Two observers independently screened the video recordings using a standardised evaluation sheet. The inter-rater reliability was 87%.
Statistics
All statistical analyses were performed with Windows Excel 2010. IRs were calculated with the following formula: incidence = (number of injuries/hours of match exposure)×1000. For the IRs, 95% CIs were calculated as follows14:
Lower 95% CI = Incidence/e1.96 × (square root [1/number of incidents])
Upper 95% CI = Incidence * e1.96 x (square root [1/number of incidents])
Injury incidences before and after the rule change were considered significant if the 95% CI of the incidence rate ratio (IRR) did not include 1.0 and if the p value of the z-statistics was <0.05 (significance level for the α-error).15 16 Descriptive data such as injury characteristics are presented as absolute numbers and percentages in parentheses.
Results
Exposure and injury incidence rates (IRs)
Exposure and IRs are shown in table 2. The total exposure over the 13-season period was 1 60 413 hours. A total of 356 head injuries occurred of which 92% were time loss injuries. The IR for each season is shown in figure 1. The IR for head injuries was 2.22 (95% CI 2.00 to 2.46) per 1000 match hours. Lacerations/abrasions were the most common head injuries (33%); concussions/TBIs and facial fractures accounted for 25% each; and contusions (12%) and ‘other injuries’ (5%) were the least frequent injuries. 15% of all head injuries accounted for suspected concussions. The highest average time loss (14±12 days, median 9 days) was observed in facial/head fractures, followed by concussions/TBIs (11±10 days, median 7 days), head contusions (5±4 days, median 4 days) and lacerations/abrasions (4±4 days, median 3 days).

Head injury variability in 13 seasons (2000/01–2012/13).
Comparison of injury characteristics of head injuries between the seasons 2000/01–2005/06 and 2007/08–2012/13
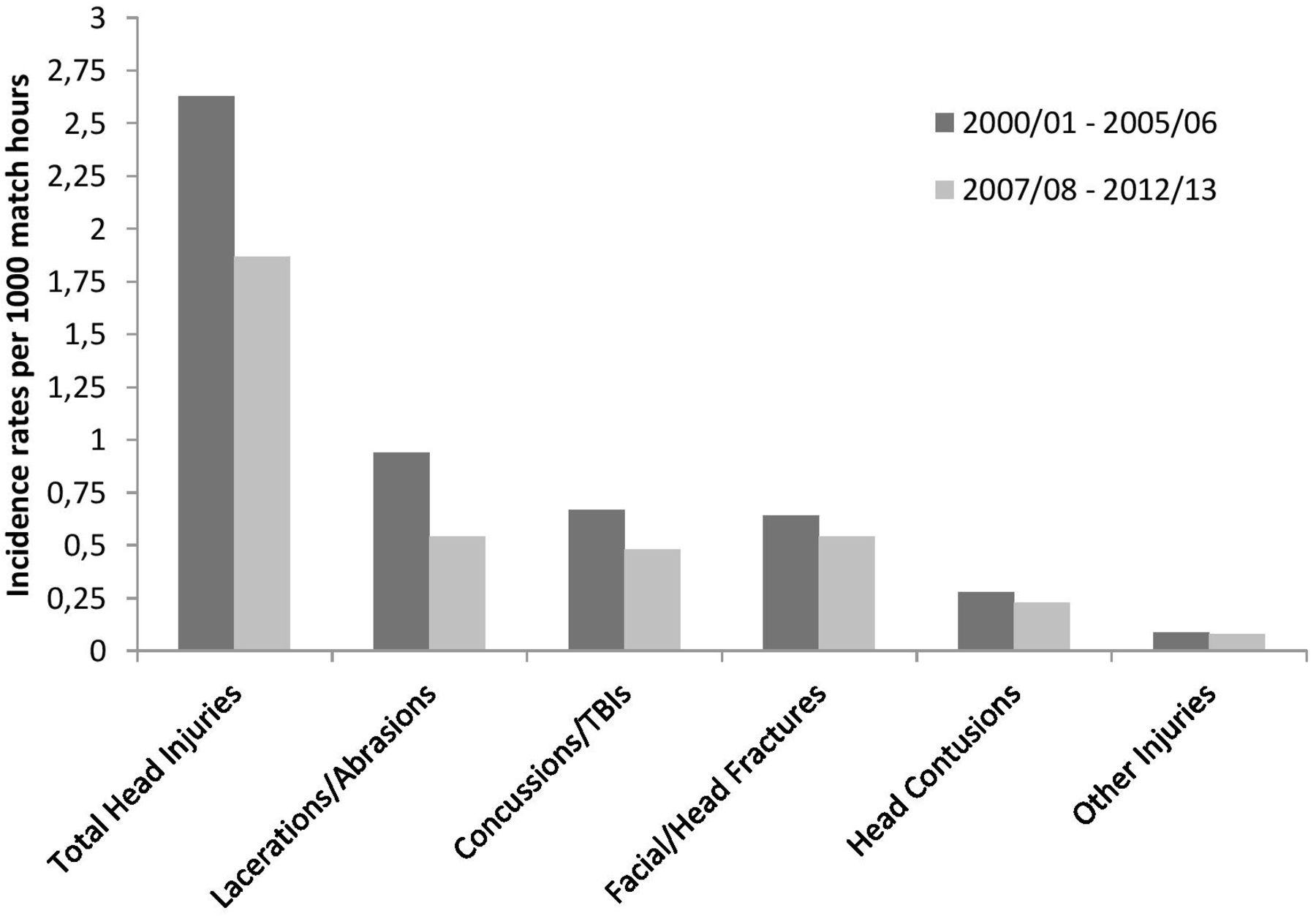
The comparison before and after the rule change in 2006 is shown in figure 2 and table 2. There was a lower number of head injuries in the seasons after the rule change (2007/08–2012/13) compared with before (2000/01–2005/06).
{kind=link}
{kind=link}
Head injury incidence rates for the seasons 2000/01–2005/06 and 2007/08–2012/13.
Injury mechanism
The detailed injury mechanisms are presented in table 3. The IRR for the three most frequent injury mechanisms for the first six seasons (2000/01–2005/06) versus the last six seasons (2007/08–2012/13) was 0.86 (95% CI 0.60 to 1.25, p=0.43) for head–head, 0.77 (95% CI 0.46 to 1.29, p=0.32) for elbow–head and 0.71 (95% CI 0.34 to 1.49, p=0.37) for foot–head.
Video analysis of injury mechanisms of head injuries
Point of contact on the head and tackle direction
More head impacts involved the side in the seasons 2007/08–2012/13 compared with 2000/01–2005/06 (IRR 2.23, 95% CI 1.30 to 3.84, p=0.004). The back of the head was significantly more often affected in the first six seasons (IRR 0.08, 95% CI 0.01 to 0.65, p=0.017). There was no difference for front and top of the head contacts. There was no significant difference in tackle direction before and after the rule change.
Discussion
After the rule change that introduced the red card in 2006, the overall number of head injuries decreased by about 29%. Lacerations/abrasions declined by 42%, and there were also reductions in concussions/TBI (29%), contusions (18%) and facial fractures (16%). The injury mechanism elbow–head was reduced by about 23%.
Epidemiology of head injuries in professional football
Compared with other contact sports such as rugby, American football or ice hockey, the IRs of head injuries in elite football are low.1 17–19 Injury rates in training are considerably lower than match and overall (comprising match and training injuries) rates.20 Nilsson et al 18 reported a 38-fold higher rate of head injuries during matches compared with training and a 78-fold higher rate of concussions. Fuller’s work that led to the rule change in 20068 reported an IR for head injuries of 12.5/1000 match hours with regard to international tournaments. The IR of head injuries is highest in matches of international tournaments8 21 and can reach IRs for muscle injuries of approximately 10/1000 match hours15 22 and joint injuries of 8/1000 match hours.15
Injury mechanisms and rule change
A rule was changed punishing direct and intentional elbow to head hits with a red card. All injury types were reduced after this rule change, demonstrating that rule changes in professional football may be an effective means to prevent injury. Nevertheless, a considerable variability of injury incidences over the 13-year period became apparent (figure 1). A longitudinal investigation of head injuries comprising, for example, 10+ years after the rule change is required to allow for a judgement on whether the rule change has a permanent effect.
Head injuries caused by elbow to head movements were less frequent after the rule change (IRR 0.77). This finding is in line with the results of Bjørneboe et al 23 who found a reduction in the rate of head incidents as well as head incidents caused by arm to head contact after stricter interpretation of the rules. Adding season 2006/07 to the six seasons after the rule change decreased the IRR from 0.77 to 0.66. It remains unknown how much the missing video recordings would have changed the injury mechanism elbow–head.
Extending current literature, any kind of body contact with another player was the most frequent cause of head injuries (as opposed to contact with the ground, posts, etc). Although the IR of head injuries was lower after the rule change, the percentage of contact-related injuries remained high. Potentially, there were fewer fouls or a greater commitment to fair play during header duels after the rule change, but it is impossible to reduce or even eliminate any contact between players as this is a fundamental part of football.
Head–head contact was the most frequent injury mechanism, followed by elbow–head and foot–head both before and after the rule change. The present results for head–head contact (34%) match with previously published data reporting 30–33%.1 8 24 25 The data of Delaney et al 24 matched the results of this study with regard to elbow–head events (17% in both studies). Andersen et al 1 reported a higher number of 34%. The upper extremity (including hand and arm) caused 35%8 and 38%,25 respectively, of head injuries. It should be noted that the latter studies were performed before the adaptation of the law in 2006 and might therefore have demonstrated higher numbers compared with the results of the present study.
Heading is a unique feature of football. The attempt to head the ball was the predominant action performed by both injured and non-injured players. Interestingly, no head injury occurred after intentional heading of the ball, indicating that the skill ‘heading’ is well trained. The effects of repetitive heading without resulting in concussions remain to be elucidated and were not within the scope of this project. Literature reviews on heading report conflicting results,5 7 26 27 but need to be interpreted with caution as the differentiation between (serial) concussions and sub-concussive blows is mandatory at this point.
Methodological considerations
All retrospective studies have some risk of bias and allow limited causal inference. Other factors, besides the rule change, may have contributed to the reduction of head injuries. Omitting season 2006/07 was considered to most appropriately carve out the potential effect of the rule change.
Interpreting head injuries is difficult as injuries with (accompanying) concussion symptoms are often not diagnosed as concussion or TBI but, for example, as head contusion only. Concussions can easily be overlooked by laypersons and even medical staff due to mild symptoms or even masked post-injury signs by the player himself. Donaldson et al 10 added facial fractures, excluding the nasal bone, to the category of concussion under the subheading ‘suspected concussion’. Their rationale was that substantial force is required to cause a facial fracture and this could also be associated with an intracranial injury.28 29 According to this, the estimated number of unreported cases of concussions and TBIs is even higher than has been reported,17 18 but remains uncertain. We used the diagnosis ‘suspected concussion’ as well. Facial fractures were included only if they affected the zygomatic bone or the skull. Additionally, head contusions to the aforementioned bones counted towards this category. Injuries affecting the nasal bone such as fractures or contusions, mandibular fractures and lacerations/abrasions were excluded from that category as such injuries may not necessarily transmit the force of impact directly to the cranium and the brain respectively. Certain lacerations/abrasions (if located directly on the skull) might be forceful enough to cause concussions and may also be classified as minor intracranial injuries. On the other hand, injuries retrospectively assigned to the category ‘suspected concussion’ might not have resulted in concussion-like impairments. Thus, the error of estimation for ‘suspected concussion’ seems likely to be somewhat balanced. Some head injuries (7%) encompassed more than one diagnosis. In these cases the more severe injury was recorded. These more comprehensive injuries might prolong the anticipated recovery time, and thus the time loss and the return to play.
Return to play after sustaining a concussion was previously recommended after 7–10 days.6 However, symptoms may persist even longer.30 31 The mean time loss after concussion and TBI during the 13-season period of the study was 11 days. This is consistent with the data of Nilsson et al.18 However, half of the present concussed players returned to play in less than 1 week despite current consensus recommendations that emphasise a sufficient rest period to achieve full recovery.6 Our data suggest that at least some players may have returned to play prematurely after concussion, but our study was not designed to address such a question.
In this analysis 82% of the head injuries were available on video recordings and can be regarded as excellent. This percentage is in accordance with a previous study in which 80% were identified.12 Other video analysis-based studies identified about 66%8 and 65%.1 The inter-rater reliability of 87% can be regarded as good compared with previously published studies of 85%8 and 95%.9 Only 18% of the head injury events were not available on video recordings. We see the video evidence and analysis as a strength of this study.
A strength of data collection in professional male football is the accuracy of time loss recording as full-time football players are seen daily by the medical staff. The football magazine ‘kicker Sportmagazin’ is published twice weekly with one journalist being responsible for one club and usually having contact with the club every day. Similarly, online open-source sports databases and the diagnoses being communicated to these media by team officials have previously been used to gather information on injuries in professional football.17 32 Yet the present data were not validated with medical records by each team’s medical departments.
Conclusion
Most head injuries in professional male football are caused by head–head and elbow–head contacts. After the rule change, the IR for elbow–head incidents decreased by 29% as well as the IRs for all head injury types. Rule changes in football may be an appropriate means of achieving a reduction in head injuries.
What are the new findings?
The injury incidence rate for head injuries in German professional football is lower than in high-risk sports
Head to head and the unfair use of the elbow are the main injury mechanisms leading to head injuries
Rule changes as an injury prevention strategy appear to reduce the occurrence of head injuries
Lacerations/abrasions and concussions/traumatic brain injuries decreased the most
How might it impact on clinical practice in the near future?
As head injuries bear the potential risk of long-term health sequelae, the identification of injury mechanisms is essential to develop preventative means in the future
The present data may be helpful for decisions on when to return to play
Acknowledgments
The authors wish to thank the ‘kicker Sportmagazin’ magazine for granting access to their online issues. The video recordings were obtained from the official German Football League (Die Liga – Fußballverband (DFL)).
References
Footnotes
Contributors TM, FB and CR were responsible for the conception and design of the study. FB was responsible for data collection over the study period. FB conducted the statistical analyses. FB, TT and KadF conducted the video analyses. FB wrote the paper. The draft of the paper was critically revised by CR, KadF and TM.
Funding This study was funded by the German Federal Institute of Sports Science.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. The funding statement was inadvertently omitted and this has now been reinstated. We would like to apologise to the authors for any inconvenience caused.