Article Text

Abstract
Objectives To determine development of new and worsening meniscal damage over 5 years after acute anterior cruciate ligament (ACL) injury comparing rehabilitation plus early ACL reconstruction (‘early-ACLR’) versus rehabilitation with optional delayed ACL reconstruction (‘optional-delayed-ACLR’).
Methods We used knee MRIs from the only randomised controlled trial in the field including 121 young adults. One musculoskeletal radiologist read baseline and 5-year follow-up images using the Anterior Cruciate Ligament Osteoarthritis Score (ACLOAS). We defined development (ie, new and worsening) of meniscal damage both dichotomously and as a sum score representing severity (based on the reclassified ACLOAS meniscus grades). In the full analysis set, we analysed development of meniscal damage (yes/no) with logistic regression and severity with zero-inflated Poisson regression and adjusted for age, sex and baseline meniscal damage.
Results Over 5 years, new or worsening meniscal damage developed in 45% of subjects with early-ACLR and in 53% of subjects with optional-delayed-ACLR. The relative risk for development of meniscal damage on knee level was 1.3 (95% CI 0.9 to 1.9) in optional-delayed-ACLR versus early-ACLR. For medial and lateral meniscal damage, respectively, the relative risks were 2.1 (95% CI 1.1 to 3.9) and 1.0 (95% CI 0.6 to 1.5). The mean severity score was 1.5 higher (more severe damage) on knee level in optional-delayed-ACLR versus early-ACLR (95% CI 1.1 to 1.9) among those with meniscal damage at 5 years. For medial and lateral meniscal damage, respectively, the corresponding scores were 1.7 (95% CI 1.2 to 2.5) and 1.1 (95% CI 0.8 to 1.4).
Conclusion A strategy of early-ACLR may reduce development of medial meniscal damage following acute ACL injury. For the lateral meniscus, ACLR seems neither to be protective nor to increase the risk of damage.
Trial registration number ISRCTN 84752559.
- ACL
- knee
- meniscus
- randomised controlled trial
- knee surgery
Statistics from Altmetric.com
Introduction
Every year in Sweden, about 80 per 100 000 inhabitants aged 10–64 suffer an anterior cruciate ligament (ACL) injury of whom more than 60% are estimated to have surgical reconstruction of the torn ACL, within an average of 400 days after injury.1 2 An ACL injury often results in reduced knee function and the inability to perform high-level sports due to ensuing knee instability.3 4 Meniscal tears and traumatic cartilage damage are common concomitant injuries.5 6 Over time, the risk of developing meniscal damage increases after the ACL injury.7 It has been suggested that recurrent instability episodes due to the ACL injury after a non-surgical treatment strategy increase the risk for incident meniscal tear.7 This is a commonly used argument to perform early ACL reconstruction. However, there is no low-risk-of-bias evidence to support an advantage of early reconstruction of the ACL to a treatment strategy with rehabilitation and optional delayed ACL reconstruction in the prevention of further meniscal damage. Although the findings from one systematic review suggested an increased risk for meniscal damage after delayed ACL reconstruction, all included studies had important methodological shortcomings.8 For instance, there are strong selection criteria that determine whether a patient undergoes primary ACL reconstruction or rehabilitation with optional delayed ACL reconstruction. These selection criteria (eg, postinjury physical activity level, return to sports, body mass index and level of instability) may be associated with risk of meniscal damage. Also, these studies do not take into account the frequent meniscal procedures often performed at the time of early ACL reconstruction (eg, partial meniscectomy or repair), which may introduce bias in favour of ACL reconstruction. The research question is of particular importance as loss of meniscal function is associated with up to sixfold increased risk for the development of knee OA.9–13 Therefore, we investigated in this exploratory analysis the development of meniscal damage after 5 years on knee MRI, using data from the only randomised controlled trial (RCT) in the field, which compared rehabilitation with early ACL reconstruction versus rehabilitation with optional delayed ACL reconstruction.6
Methods
Study design
We used data from the Knee Anterior Cruciate Ligament, Nonsurgical versus Surgical Treatment (KANON) study (ISRCTN 84752559) for a secondary analysis.6 The trial was a RCT involving 121 young active adults that were randomised by computer-generated random numbers in permuted blocks of 20 to undergo structured rehabilitation and early ACL reconstruction (‘early reconstruction arm’) or structured rehabilitation with optional delayed ACL reconstruction (‘optional delayed reconstruction arm’). Allocation concealment was ensured by sequentially numbered, opaque, sealed envelopes, prepared by an investigator who was not involved in the randomisation procedure. The study was approved by the Ethics Committee of Lund University (LU 535–01).
Participants
Participants were recruited from the Department of Orthopedics at Lund University and Helsingborg hospital between February 2002 and June 2006 and were followed up at 5 years until 2011. Persons between 18 and 35 years of age with a recent knee trauma were eligible. They were included when a rotational trauma occurred to an uninjured knee, had an ACL injury determined by clinical examination and confirmed by MRI and participated in sport before the injury (score 5–9 on the Tegner Activity Scale). A person was excluded if any or both of the collateral ligaments were completely ruptured, if an unstable longitudinal meniscus tear required extensive repair which interfered with the rehabilitation protocol, and if a full thickness cartilage lesion was observed on MRI. Additional exclusion criteria have been reported.6
Outcomes
All included persons underwent knee MRI using the exact same scanner, a 1.5 T system (Gyroscan, Intera, Philips, Best, The Netherlands) with a circular polarised surface coil with identical sequences for all subjects and all time points. Knee MRIs at baseline (after randomisation but before treatment) and at 5-year follow-ups were read paired with knowledge of time sequence by one experienced musculoskeletal radiologist. Readings were performed using the cine-loop function on a standard clinical PACS system (GE Healthcare, Centricity, Barrington, Illinois, USA). Scores were recorded electronically on a designated custom-developed score sheet (MS Access, Microsoft, Redmond, Washington, USA). Reader blinding to ACL-reconstructed knees at the 5-year follow-up was not feasible, but the reader was unaware of the specific study questions or of any surgical interventions during the study period. Meniscal damage on MRI was scored according to the Anterior Cruciate Ligament Osteoarthritis Score (ACLOAS, online supplementary appendix, table 1).14 The primary outcome in the present report was development of meniscal damage defined as (1) an incident meniscal tear on follow-up MRI, which was not present at the baseline scan and (or); (2) a pre-existing meniscal tear which has expanded to involve another meniscal segment and (or); (3) incident loss of meniscus substance due to destruction, maceration or meniscal resection and (or); (4) increased medial or lateral meniscal body extrusion grade according to ACLOAS and (or); (5) new finding of postmeniscal repair.
Supplemental material
For greater sensitivity and to evaluate severity of meniscal damage, we also introduced a severity score based on the reclassified subregional meniscal grades from the ACLOAS (online supplementary appendix, table 1). We assigned the severity score to each meniscal segment (anterior, body and posterior for medial and lateral meniscus). On the knee level, all severity scores from the six segments were summed ranging from 0 to 30 points (0 if both menisci were normal at 5 years; 30 if both menisci were fully destroyed in all three subregions and any remnant of peripheral body rim was fully extruded at 5 years). Consequently, for compartment-specific exposure (medial and lateral meniscus, respectively), the severity scores could range from 0 to 15.
We also detailed the number and type of meniscal surgeries. Meniscal tears in both the early and delayed ACL reconstruction arms were treated either with an arthroscopic partial resection or repair depending on clinical signs and symptoms, MRI appearance and findings during surgery. For the early reconstruction arm, meniscal surgeries were typically performed concomitant with the ACL reconstruction and only occasionally at a separate knee arthroscopy. For the optional delayed reconstruction arm, meniscal surgeries were done as needed, that is, depending on clinical signs and symptoms and sometimes concomitant with the optionally delayed ACL reconstruction.
Statistical analysis
Baseline characteristics were summarised by mean and SD if continuous and normally distributed. If not so, data were summarised by medians and IQR. Categorical data were reported as absolute and relative frequencies.
In the full analysis set, we compared the proportions of developing (ie, new and worsening) meniscal damage on MRI (yes/no) between the two treatment arms using logistic regression. The model was adjusted for age, sex and baseline meniscal damage on MRI. Baseline meniscal damage was adjusted for if at least one of the segments had a meniscal tear at baseline, irrespective of the number of segments involved. In addition to relative risks (RR), we also present risk differences to provide estimates with easier clinical interpretation. We computed risk ratios and risk differences indirectly from a logistic regression model using method of standardisation as implemented in the Stata command adjrr.15 16 To compare severity of meniscal damage at 5 years using our sum score, we used a zero-inflated Poisson regression model, which accounted for the excessive zeros in the severity scores. This model was adjusted for age, sex and baseline severity score. Participants without MRI readings at baseline or at the 5-year follow-up were excluded from the regression analyses. After performing the analysis on knee level, we also repeated the analyses on compartment level, that is, separately for the medial and lateral meniscus.
In a secondary descriptive analysis, we presented the proportion of meniscal surgeries and the number of repeated meniscal surgeries for the early reconstruction arm and for the optional delayed reconstruction arm at three time points: (i) early meniscal surgeries, performed within 5 weeks after randomisation; (ii) delayed meniscal surgeries, performed 5 weeks until 5 months after randomisation; (iii) late meniscal surgeries, performed 5 months or later after randomisation. The overall proportions of meniscal surgeries in both treatment arms have been reported elsewhere.17
Last, we reported the descriptive statistics for the subjects as-treated. Subjects were then divided into early ACL reconstruction, delayed ACL reconstruction and rehabilitation only. As this is a secondary analysis of a RCT, we did not perform a formal sample size calculation prior to conducting this study. All analyses were performed in STATA V.15 and RStudio V.3.5.1.
MRI diagnostic accuracy
To estimate the diagnostic accuracy of detection of meniscal tear on MRI, we compared the ACLOAS baseline MRI readings with the clinical (non-ACLOAS) baseline MRI readings (from two different radiologists) of the study subjects as well as validation with the surgical reports from the early ACL reconstruction arm (considered the gold standard, although the surgeons had access to the clinical (non-ACLOAS) MRI readings before surgery). Meniscal tear in the ACLOAS was defined in accordance to ACLOAS grade 2–8. The clinical MRI readings have been reported in previous KANON publications,6 17 and here the scoring method consisted of four items: (i) no intrameniscal signal, (ii) intrameniscal signal not reaching surface, (iii) linear intrameniscal signal not reaching surface and (iv) intrameniscal signal reaching meniscal surface/meniscal tear. We defined a meniscal tear if the clinical grade was (iv).
Patient and public involvement
Patients were not involved in this research to comment on the study design or interpret the results. Patients were not invited to contribute in the writing or editing of the manuscript.
Results
Descriptive statistics
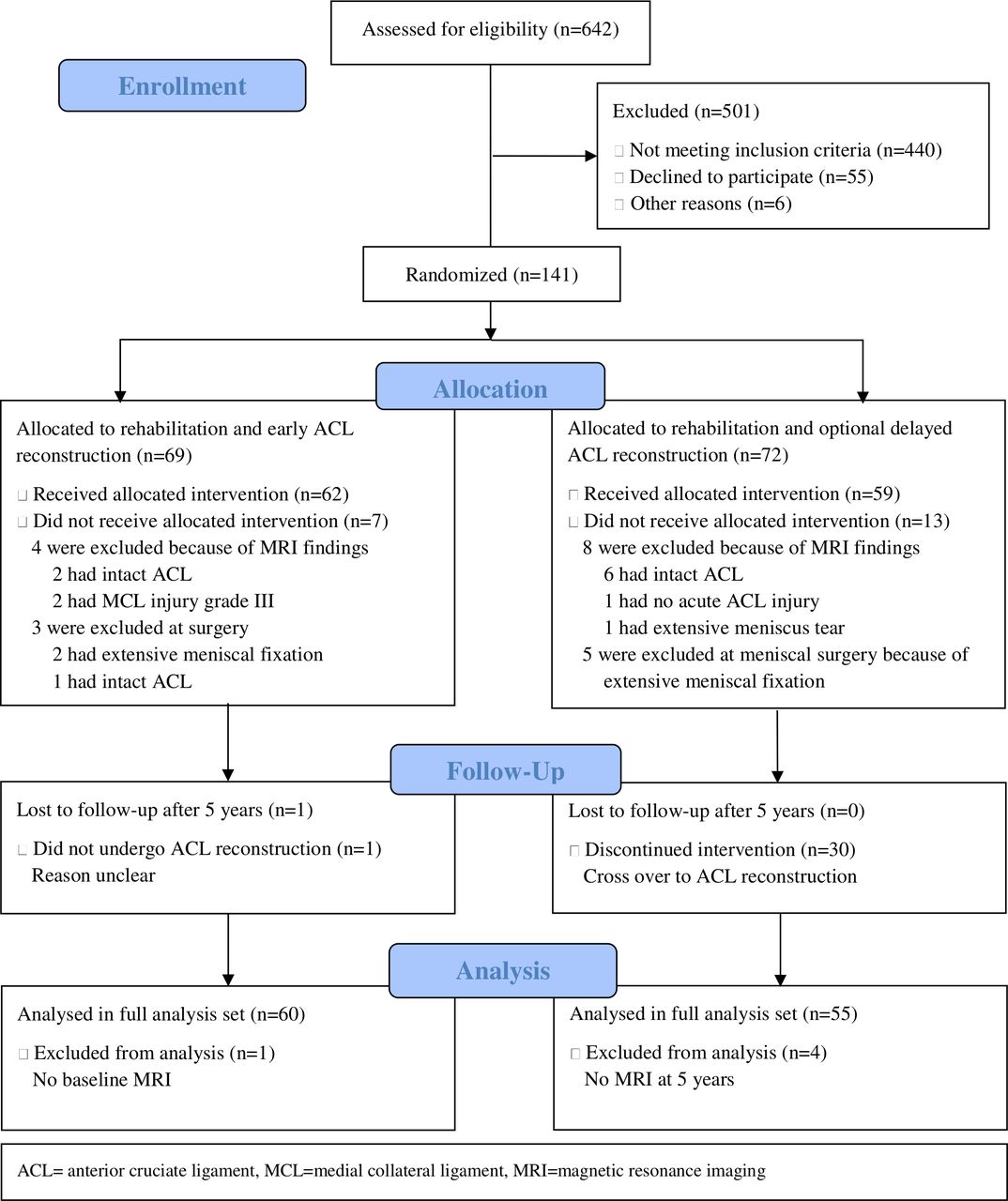
In the early reconstruction arm, 62 participants were included, of which one was lost to follow-up, leaving 61 subjects for analysis. In the optional delayed reconstruction arm, 59 subjects were included without loss to follow-up, with 30 subjects (51%) crossing over, that is, having had delayed ACL reconstruction within 5 years (figure 1). Subjects in the early reconstruction arm had a mean age of 26.3 years (SD 5.1) and 81% were men. In the optional delayed reconstruction arm, subjects had a mean age of 25.8 years (SD 4.7) and 66% were men.

Flow diagram.
In the early reconstruction arm, one subject had no MRI available at baseline and was therefore excluded from the analyses using MRI-based outcomes. In the optional delayed arm, four subjects had no MRIs obtained at 5 years and were excluded from the analyses using MRI-based outcomes. Before treatment, the early reconstruction arm had more lateral meniscal damage detected on MRI (ACLOAS; 25% vs 7%), but the proportion of medial meniscus damage was similar in both treatment arms (15%, table 1).
Baseline characteristics (full analysis set)
Development of meniscal damage
After 5 years, 27/60 (45%) of subjects in the early reconstruction arm had developed new (or worsening of) meniscal damage vs 29/55 (53%) in the optional delayed reconstruction arm. For medial meniscus, the corresponding proportions were 18% vs 38% and for lateral meniscus 37% vs 22%, respectively. Two examples of meniscal development on MRI over the course of 5 years have been included in the online supplementary appendix, figure 1. The frequency of each item that defines the development of meniscal damage has been included in the online supplementary appendix, table 2.
We found a RR for development of meniscal damage after 5 years on the knee level of 1.32 with a 95% CI of 0.92 to 1.88 in the optional delayed reconstruction arm versus the early reconstruction arm (table 2). For development of medial meniscal damage, the RR was 2.10 (95% CI 1.14 to 3.86), with a corresponding risk difference of 20.1% (95% CI 4.5% to 35.7%). For the lateral meniscus the RR was 0.97 (95% CI 0.63 to 1.52), with a corresponding risk difference of 0.0% (–13.9% to 12.4%). Corresponding ORs are presented in the online supplementary appendix, table 3. A greater proportion of subjects with no apparent pathology in the medial meniscus at baseline in the optional delayed reconstruction arm developed medial meniscal damage after 5 years compared with the early reconstruction arm (34% vs 12%). The most frequent change in meniscal integrity was status postpartial meniscectomy in the medial and lateral meniscal body and posterior horn (figure 2).
Results of the logistic regression analysis for development of meniscal damage and the zero inflated Poisson regression analysis for meniscal severity scores at 5 years compared with baseline for the optional delayed ACL reconstruction arm compared with the early ACL reconstruction arm (full analysis set)

{kind=link}
{kind=link}
Development of meniscal damage over 5 years compared with baseline MRI without adjustment for baseline meniscal damage. ACL, anterior cruciate ligament; APM, arthroscopic partial meniscectomy; MR, meniscal repair; MT, meniscal tear,.
Severity of meniscal damage
The observed severity score at 5 years ranged from 0.5 to 9.5 on knee level. Among those with meniscal damage at 5 years (severity score >0), for an average person in the early reconstruction arm the mean severity score on knee level was 2.7, while for an average person in the optional delayed reconstruction arm it was 3.9 (online supplementary appendix, table 4). This corresponds to an adjusted 1.46 higher (more severe) mean score on knee level (95% CI 1.13 to 1.87) in the optional delayed reconstruction arm (table 2). For medial meniscus, the corresponding ratio was 1.71 higher mean severity score (95% CI 1.18 to 2.47) in the optional delayed reconstruction arm and for lateral meniscus 1.06 (95% CI 0.80 to 1.40). The change in severity score from baseline to the 5-year follow-up for the medial and the lateral meniscus for each treatment arm, respectively, is detailed in the online supplementary appendix, figure 2. Because the zero inflated Poisson regression model has two parts, we present next to the results of the Poisson count model, also the inflated model for the prediction of excess zeros (online supplementary appendix, table 5).
Meniscal surgeries
At 5 weeks after randomisation, in the early reconstruction arm 43% of subjects had a meniscal surgery, compared with 24% in the optional delayed reconstruction arm. After 5 years, the number of persons with any meniscal surgeries was similar in both treatment arms (table 3).
Number of meniscal surgeries for the optional delayed ACL reconstruction arm compared with the early ACL reconstruction arm at three time points after randomisation (full analysis set)
As treated analysis
Development of meniscal damage on MRI was more frequent in the delayed ACL reconstruction group compared with the early ACL reconstruction arm and the rehabilitation only group (table 4). More than half of all meniscal surgeries in the delayed ACL reconstruction group were performed before ACL reconstruction (table 4).
Descriptive analysis on worsening of meniscal integrity and the number of meniscal surgeries for three as treated groups at 5 years of follow-up
MRI diagnostic accuracy
The overall diagnostic accuracy for medial meniscal tears compared with gold standard was 77% for the ACLOAS MRI readings vs 80% for the clinical MRI readings. For lateral meniscal tears, it was 75% and 73%, respectively (online supplementary appendix, table 6).
Discussion
We found that a strategy of early ACL reconstruction with rehabilitation may reduce the development of medial meniscal damage compared with a strategy of primary rehabilitation with optional delayed ACL reconstruction. In the presence of medial meniscal damage at 5 years, tears were less severe compared with optional delayed ACL reconstruction. However, the risk for future lateral meniscal damage (and its severity) was similar in both treatment arms.
Explanation of findings
Results from several studies have suggested that delayed ACL reconstruction is associated with the development of more medial meniscal tears and chondral damage.7 8 12 18–21 However, these were observational studies with inherent limitations, for instance a high risk of selection bias. The patients in these studies who had a delayed reconstruction were probably different to start with from patients who were selected for an early ACL reconstruction, for example, due to lower level of instability or anticipated lower postinjury physical activity level. To provide more robust evidence to this clinically important question, a randomised treatment allocation is warranted, ensuring the two treatment arms are comparable at baseline with respect to patient characteristics as well as known and unknown confounders. Our results of the ‘as randomised’ full analysis set RCT data suggest that medial meniscal damage occurs more frequently after optional delayed ACL reconstruction as compared with early ACL reconstruction. Hence, early ACL reconstruction may be protective of the medial meniscus. The clinical relevance of the protective effect needs to be evaluated in larger trials, as our results suggest a wide CI between 5% and 36% less persons with development of medial meniscal damage in the early ACL reconstruction arm. This greater risk of medial meniscal damage could hypothetically be due to recurrent or chronic instability episodes in the ACL-deficient knee.7 22 It could hypothetically also be due to a higher risk of reinjuries as a consequence of a quicker resumed high level of physical activity in persons who were not surgically treated, although we found no evidence for this in the current trial.22 23 However, we did not find an increased risk of lateral meniscal damage. The lateral meniscus is not as firmly attached to the joint capsule as the medial meniscus and therefore more mobile, which could explain that in an instability episode the lateral meniscus is less susceptible to tearing.24 The previous systematic review on observational studies also found an increased risk for medial meniscal tears, but not for lateral meniscal tears.8 In addition to the increased proportion of patients with new development of medial meniscus damage in the optional delayed arm, our results suggested that among those with meniscal damage at 5 years, the severity of the damage was on average ~50% greater compared with the early reconstruction arm, strengthening the main finding. The ACLOAS meniscal scoring had interobserver and intraobserver reliability with kappa’s ranging from 0.82 to 1.00.14 Overall percentage agreement ranged from 94% to 100%. Our severity score is based on the ACLOAS grades.
Meniscal improvement was detected on MRI for three patients. It is possible that small tears regress or heal or that a very minor arthroscopic partial meniscectomy is not detected on MRI. The validation of meniscal assessment using arthroscopy as the reference, ranged around 90% sensitivity and around 80% specificity.25 26
In the early reconstruction arm, the majority (84%) of patients with meniscal surgery during the follow-up had surgery performed less than 5 weeks after randomisation, whereas in the optional delayed arm only 44% of patients had their surgery in the same time period. This can be explained by meniscal surgeries being performed simultaneously with early ACL reconstruction and by the higher proportion of patients with meniscal tears on baseline MRI (ACLOAS) in the early reconstruction arm compared with the optional delayed arm (35% vs 22%). Nevertheless, at the end of the 5-year study period, a similar proportion of patients had been surgically treated for their menisci (49% in the early arm vs 54% in the optional delayed arm). This result is not completely consistent as earlier reported, because one meniscal surgery in the early arm was accidentally not included in the previous report.17
The 5-year report from the primary KANON trial showed that there were no essential differences (statistically or clinically-relevant) between the two treatment strategies in patient-reported outcomes or physical activity level. Therefore, we advocate that both treatment strategies should be considered in the treatment of the ACL-injured knee, either primary ACL reconstruction or structured rehabilitation with optional delayed ACL reconstruction. Longer term follow-up of low-risk-of-bias ACL rupture RCTs and prospective observational studies is needed to answer the question whether these two treatment strategies differently influence the risk of further symptomatic meniscal damage or later symptomatic osteoarthritis development before more definitive clinical recommendations can be made.
Limitations
We would like to state some important limitations. The detection of meniscal tears on MRI in the acutely injured knee in young individuals poses particular challenges, and the diagnostic accuracy may be lower than in older populations.25–27 We also found discrepancies between our ACLOAS readings and the prior clinical MRI readings, which is most likely explained by different calibration of two different readers, the use of different scoring systems (ACLOAS versus clinical), and that surgical reports (gold standard) were biased towards the clinical MRI readings which were available during surgery to help find meniscal tears.
Second, we use the term full analysis set, because the assumption for an intention to treat analysis that all randomised participants should be included was violated. Two persons in the early ACL arm and four persons in the optional delayed ACL arm were excluded because they did not have either baseline or follow-up MRI readings. This may have resulted in selection bias, for example, if MRI readings were more frequently missed in the optional delayed arm for persons with better outcomes, which could lead to a slight bias in our results.28 However, the number of excluded patients was so small that we expect the impact would be negligible.
Last, we did not provide a complete multivariable as treated analysis, because we could not ascertain the time of occurrence of the meniscal damage detected on the 5-year MRI scan (eg, before or after the delayed ACL reconstruction). Thus, we only provided descriptive statistics for the groups as they were treated.
Conclusion
Every second subject developed new or worsening meniscal damage over the first 5 years after an ACL injury. Our present analysis suggests that a strategy of early ACL reconstruction may reduce the risk of developing medial meniscal damage over this time period. In the presence of a medial meniscus tear, more severe tears were observed in the optional delayed ACL reconstruction arm compared with the early ACL reconstruction arm. For the lateral meniscus, early ACL reconstruction was neither protective nor increased the risk for development of meniscal damage. Because previous reports from the KANON trial showed no essential differences between the two treatment strategies, we advocate that both strategies should be considered in the treatment of the ACL-injured knee. The 10-year follow-up of the patients in the KANON-trial may shed further light on patient-reported outcomes and the natural course of meniscal integrity based on these two treatment strategies, that is, early versus optional delayed reconstruction of the ACL.
What is already known
Delayed ACL reconstruction is associated with the development of more medial meniscal tearsand chondral damage, but evidence comes from observational studies with inherent limitations.
What are the new findings?
With the use of randomised controlled trial data, we found that a strategy of early anterior cruciate ligament (ACL) reconstruction and rehabilitation may reduce the development of medial meniscal damage compared with a strategy of primary rehabilitation with optional delayed ACL reconstruction.
In the presence of medial meniscal damage, tears were less severe after early reconstruction than after optional delayed ACL reconstruction.
The risk for future lateral meniscal damage (and its severity) was similar in both treatment arms.
References
Footnotes
Twitter @barbara_snoeker
Contributors Barbara Snoeker takes responsibility for the integrity of the data and the accuracy of the data analysis. Barbara Snoeker and Aleksandra Turkiewicz performed statistical analyses. Barbara Snoeker drafted the manuscript. Frank Roemer, Aleksandra Turkiewicz, Richard Frobell, Stefan Lohmander, and Martin Englund contributed with acquisition of data, conceptual design, and analysis and interpretation of data. Barbara Snoeker, Frank Roemer, Aleksandra Turkiewicz, Richard Frobell, Stefan Lohmander, and Martin Englund contributed in drafting the article or critically revising it for important intellectual content. All authors gave final approval for the version to be submitted.
Funding The KANON study and this project received funding from The Swedish Research Council, Greta and Johan Kock Foundations, the Medical Faculty of Lund University, Region Skåne, Governmental funding of clinical research within the national health services (ALF), The Swedish Rheumatism Association, Thelma Zoegas Fund, The Stig & Ragna Gorthon Research Foundation, Swedish National Centre for Research in Sports, Crafoord Foundation, Tore Nilsson Research Fund and Pfizer Global Research.
Disclaimer Funding sources had no role in the design, collection and interpretation of the data or the decision to submit for publication.
Competing interests FWR, one of the coauthors, is Chief Medical Officer and shareholder of BICL, LLC.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.