Article Text

Abstract
Objectives To adapt key components of exertional heat stroke (EHS) prehospital management proposed by the Intenational Olympic Committee Adverse Weather Impact Expert Working Group for the Olympic Games Tokyo 2020 so that it is applicable for the Paralympic athletes.
Methods An expert working group representing members with research, clinical and lived sports experience from a Para sports perspective reviewed and revised the IOC consensus document of current best practice regarding the prehospital management of EHS.
Results Similar to Olympic competitions, Paralympic competitions are also scheduled under high environmental heat stress; thus, policies and procedures for EHS prehospital management should also be established and followed. For Olympic athletes, the basic principles of EHS prehospital care are: early recognition, early diagnosis, rapid, on-site cooling and advanced clinical care. Although these principles also apply for Paralympic athletes, slight differences related to athlete physiology (eg, autonomic dysfunction) and mechanisms for hands-on management (eg, transferring the collapsed athlete or techniques for whole-body cooling) may require adaptation for care of the Paralympic athlete.
Conclusions Prehospital management of EHS in the Paralympic setting employs the same procedures as for Olympic athletes with some important alterations.
- disabled persons
- body temperature regulation
- hot temperature
- wheelchair
- athletes
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
With the increasing knowledge in the clinical management of heat-related illnesses, development of specific guidelines and protocols to treat exertional heat stroke (EHS) and other heat-related conditions are becoming readily available.1–3 These documents are of high relevance considering global warming, the increasing number of mass participation events that take place in extreme environments and the increasing number of participants of all competitive levels engaging in these events. Although elite athletes, including Paralympic athletes, are more likely to be better prepared for competing in the heat (ie, heat acclimatisation, pre-cooling and par-cooling) the medical care provided in elite events follow the same principles as those applied at mass participation events. The environmental conditions at the Tokyo 2020 Summer Olympic and Paralympic Games have raised concerns among teams, organisers and the scientific community due to the expected high temperatures and relative humidity, based on the recent trends and reports.4 In this context, a new set of guidelines for prehospital management of EHS at the Tokyo 2020 Olympic Games was recently published, focusing on the medical care and logistical set up required to provide high-quality care at the sporting venue.3 Although the clinical management of EHS in athletes competing in Para sport may adopt the same principles, there are substantial differences that should be taken into consideration when organising prehospital management strategies.
Athletes at the Paralympic Games are classified into 10 impairment types (eight physical impairments as well as visual and intellectual impairments) resulting in a heterogeneous athlete population. The available evidence indicates that the incidence of EHS in the Paralympic athlete population is low.5–7 Nonetheless, some Paralympic athletes across the spectrum of eligible impairments are inherently at greater risk of thermoregulatory strain during exercise in the heat (table 1). As such, heat syncope/exhaustion are still possible, and clinicians must be prepared to manage these athletes appropriately at the Paralympic Games and other events globally. Additionally, given the ever-increasing standard and professionalism of Paralympic sports (eg, 124 Paralympic records were broken during the Tokyo 2020 Paralympics) and the trend towards international events being staged in hot and/or humid environments and the increased prevalence of foreseen heatwaves,8 including the 2024 venue in Paris and 2028 venue in Los Angeles, the prevalence of EHS will likely increase over time.
Examples of medical condition specific to Paralympic athletes in relation to thermoregulation
EHS prehospital care overview
Basic components of EHS prehospital care include: (1) early recognition, (2) early diagnosis, (3) rapid, on-site cooling and (4) advanced clinical care.3 Unlike other sports-related medical emergency (eg, spinal injury, brain trauma, complex fracture), EHS requires the treatment to be completed on-site first, before the patient is transported to the advanced care.9 This is due to the fact that the duration of sustained hyperthermia is known to dictate patient prognosis.10 A delay in appropriate recognition, diagnosis and cooling can lead to catastrophic outcome.11 12 Current clinical best practice suggests that EHS patients must be cooled until their core body temperature is below 39°C within 30 min of the onset.3 Therefore, it becomes critical that medical providers working at sporting events with risk of EHS are well equipped with skills and resources to execute (1) rectal temperature assessment to confirm the diagnosis, (2) rapid cooling using whole-body cold-water immersion and (3) follow-up examination to assess discharge readiness.
When possible, it may be of benefit to acquire the athlete’s medical history and ongoing therapy prior to the event since impairment type indicated by the competition class does not necessarily represent whether the athlete is predisposed to increase thermoregulatory strain. For example, eligibility in the Quad class of wheelchair tennis is not restricted to athletes with tetraplegia. Consequently, a player with a spinal cord injury at the C8 level or above versus a player with an upper limb myopathy will both be eligible, but the former is at higher risk for exertional heat illness. If personal medical information cannot be acquired due to medical privacy reasons, organisers of the event are advised to request participating athletes and staff to report any foreseeable heat-related issues prior to the day of the competition. Some of the key questions to ask include: (1) presence of thermoregulatory impairment and the reason, (2) history of exertional heat illness, (3) baseline blood pressure, if lower than the reference value and (4) any intake of medication that may alter the interpretation of vital signs.
Heat deck/medical tent
Heat deck set-up and transfer of patient from field of play to medical tent
Heat deck, a designated area for EHS treatment and management, should be located within or adjacent to the main athlete medical tent. When the sport of interest involves Paralympic athletes, who compete in wheelchair sports (eg, wheelchair racing), the space within and corridor to the medical tent must be designed to accommodate the width of varying sports wheelchairs. Securing a clean water source, ice and appropriate drainage is at high priority to manage cold water immersion tubs.
Once the Paralympic athlete is suspected of experiencing EHS at the field of play, the athlete should be transferred directly to heat deck. Medical personnel assigned to work at Paralympic events should be familiar with transfer techniques of athletes with different impairments, particularly the collapsed athlete. Manual lifting in healthcare training programmes and policies are encouraged to prevent musculoskeletal injuries to the volunteers by athlete handling.13 14 If the Paralympic athlete collapses while in sports equipment (eg, sports wheelchair, handcycle), carefully extricate the athlete from their equipment. Therefore, prior familiarisation with equipment and strapping used by athletes is important.
Management of medical tent traffic
Given the complexity of managing emergency medical conditions in Paralympic athletes, it is important that a team representative who knows the athlete well is allowed to enter the heat deck during EHS management. This will allow the team representative to provide impairment-specific information (including medications and therapeutic use exemption considerations) to the management team, which may assist in the selection of prehospital care procedures. For athletes with visual impairment, their guide should have a guaranteed entry to the medical tent to provide assistance in the care of the athlete. Furthermore, athletes with communication disability (eg, dysarthria) should be allowed to have their team representative accompany the athlete to facilitate communication throughout treatment, and to ensure that the athlete has returned to baseline mental status prior to discharge.
Patient assessment
The general principles of prehospital EHS management in Paralympic athletes do not differ greatly from the standard care used in the general athletic context (figure 1). We encourage readers to review the paper by Hosokawa et al for an overview of the fundamental concepts.3
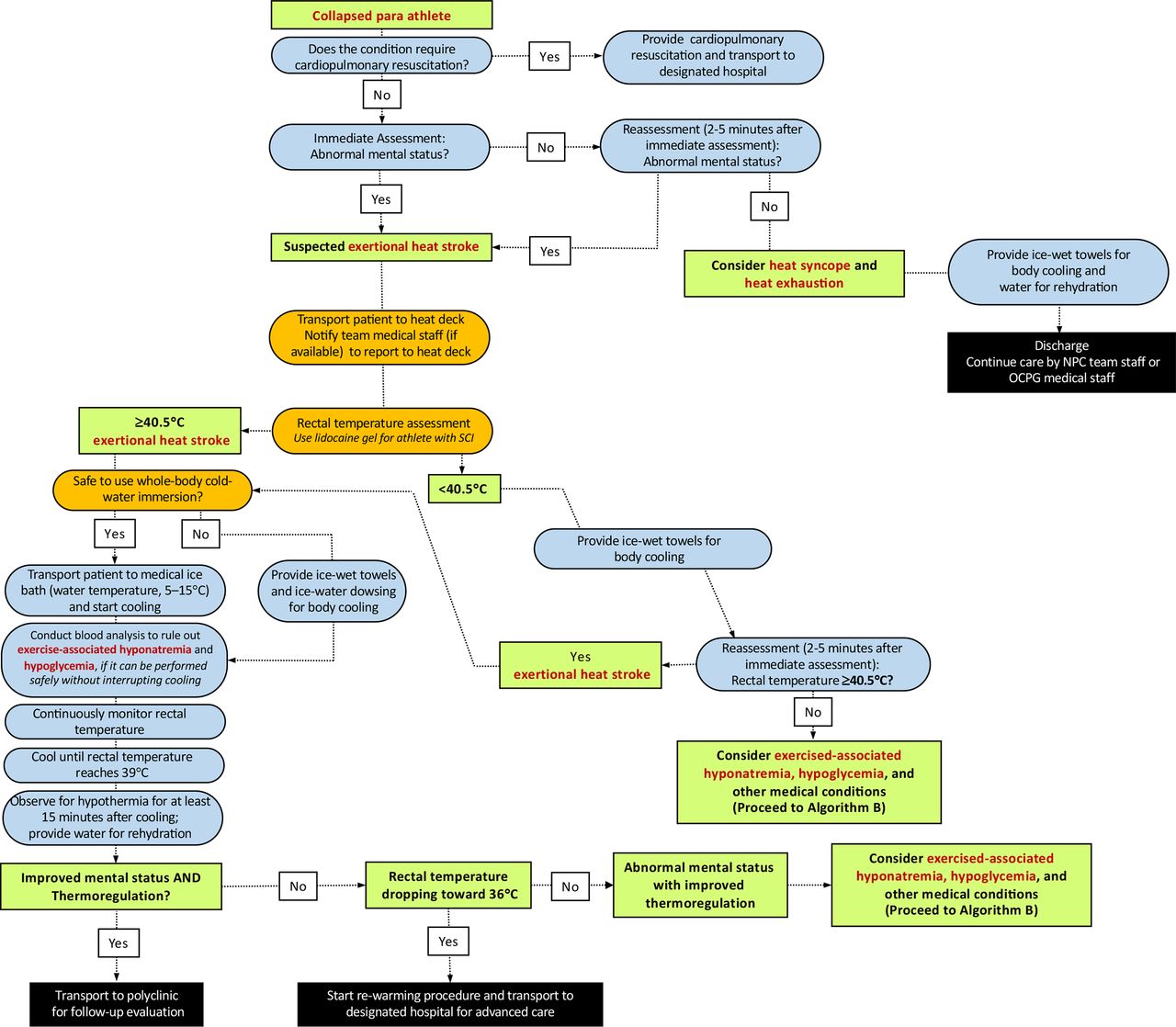
Algorithm (A1) for the initial diagnosis and management of a Paralympic athlete with suspected exertional heat stroke who has no risk of autonomic dysreflexia. NPC, National Paralympic Committee; OCPG, Organising Committees for the Paralympic Games; SCI, spinal cord injury.

Algorithm (A2) for the initial diagnosis and management of a Paralympic athlete with suspected exertional heat stroke who has potential risk of autonomic dysreflexia and impaired thermoregulation (ie, individuals with spinal cord injury at T6 or above). NPC, National Paralympic Committee; OCPG, Organising Committees for the Paralympic Games; SCI, spinal cord injury.
Rectal temperature should be assessed using a flexible probe to identify the extent of exercise-induced hyperthermia. If the collapsed athlete’s impairment is in the category of spinal cord injury at or above T6, heart rate and blood pressure should be checked immediately, and then monitored for signs of autonomic dysreflexia (AD) (table 2). These athletes are also at higher risk for impaired thermoregulation (eg, overheating/EHS or overshoot during cooling). When assessing the rectal temperature of athletes with spinal cord injury at or above T6, lidocaine gel should be used to prevent the risk of AD. However, such risk is minimal given this task constitutes only a brief, transient noxious stimulus. In relation to AD, medical providers should also consider bowel and bladder distension as the cause of AD (as EHS is unlikely to be the direct cause of AD). The induction of AD can have major implications on heart rate and blood pressure (elevations) leading to a dangerous condition. The reader is guided to Blauwet et al 15 for further guidance.
Overview of the 22 sporting events at Tokyo Paralympic Games and the sports/events where athletes are at risk for autonomic dysreflexia (AD) and impaired thermoregulation with a spinal cord injury at or above the level T6
Before moving the athlete to whole-body cold-water immersion tub, assessment for pressure sores, open wounds and local burns should also be conducted thoroughly, which may be more prevalent in amputee athletes and athletes with insensate regions (paraplegia and tetraplegia). If open wounds are present, cover the area with an appropriately disinfected or new cold-water immersion tub to avoid the risk of contamination. It should be noted that these steps must be taken expeditiously to avoid unnecessary delays in care.
Whole body cold-water immersion
Medical providers must continuously monitor rectal temperature throughout the cooling process to determine the end point of treatment (ie, rectal temperature reaches 39.0°C) (figures 1–3). Clinicians should be reminded that inserting a rectal thermometer with proper technique (ie, use of lidocaine gel) is unlikely to cause AD. The immersion tub size should be selected accordingly to the average body size of the participants. An immersion tub that is traditionally used for the purpose of recovery ice bath may not be suitable for EHS treatment as it may be too deep for medical providers to transfer the collapsed athlete in and out from the bath and has the risk of drowning (readers are referred to Hosokawa et al for sample size of the immersion tub).3 The use of a pole-less stretcher to transfer the Paralympic athlete in and out of the tub may have increased importance than Olympic athletes since manual handling and moving patients who have mobility limitations requires some practice. If an athlete with amputation experiences EHS and needs to be cooled, the prosthesis should be removed prior to immersion (or whenever possible, if it can be done safely) to maximise the skin surface to be cooled. In some cases, there will be a connection or interface device (commonly made of silicone), which should be removed to maximise the skin surface area to be cooled. In rare circumstances, where it is not safe to employ whole-body cold-water immersion (ie, athletes with known intellectual impairments who are not compliant to treatment measures), medical providers may choose whole-body rotating ice towels and/or ice water dousing as an alternative option, as these cooling methods have been shown to have adequate cooling rates.16 Tarp-assisted cooling (TACo) is another alternative cooling technique used to treat EHS.17 However, in the case where whole-body cold-water immersion is deemed unsafe, it is unlikely that the TACo method can be administered safely since it also involves significant patient transfer. Among a small group of Paralympic athletes at risk of AD (ie, spinal cord injury at or above T6), transfer and change in the positioning of the patient should be minimised as much as possible to prevent noxious inputs that could trigger AD. In such situations, medical providers may consider using a mix of whole-body rotating ice towels and partial body immersion (ie, entire upper extremity) (figure 2). The reader is directed to the work of Griggs et al 18 and Pritchett et al 19 for more practical guidance. It should be emphasised that reduction of internal body temperature within the initial 30 min of collapse ensures survival and minimises the severity of sequela.20

{kind=link}
{kind=link}
{kind=link}
Algorithm (B) for the management of an athlete with exertional heat stroke (continued from figures 1 and 2). When intravenous access is not available administer 1 mg (1 mL) Glucagon by intramuscular or subcutaneous injection and recheck blood glucose after 10 min. After Glucagon administration, administer supplemental carbohydrates orally once the patient has regained consciousness to prevent delayed hypoglycaemic. NPC, National Paralympic Committee; OCPG, Organising Committees for the Paralympic Games.
Finally, a laboratory study suggests that the risk of hypothermic overshoot may be more pronounced among athletes with impaired thermoregulation (eg, athletes with a spinal cord injury).21 Medical providers should monitor the rate of cooling closely as it may be faster compared with athletes with no disability.22 23
Hygiene-related considerations
Consider stump hygiene and skin health of athletes with a limb deficiency, particularly of the lower limb. While the residual limb may display skin irritation, if whole-body cold-water immersion is the preferred option, then ensure that once the prosthesis is removed, the area is fully dried post-immersion and cleansed to prevent infection.
Athletes with colostomy bags should still be cooled using whole-body cold-water immersion to prioritise life-saving procedure; however, whole-body cold-water immersion tub used to cool athletes with colostomy bag should be drained and disinfected after each use. If available, consider designating a large shower room (ie, such as those seen in sports arenas and locker rooms) where running water can be used to also cleanse the athlete while protecting privacy.
Post-treatment
There are currently no Para-athlete specific considerations for post-EHS treatment follow-up in the athlete medical tent. It is recommended that the need for specific testing be left to the team physician rather than medical tent team due to the wide variety of medical complications in Paralympic athletes.
Conclusion
Prehospital management of EHS in the Paralympic setting employs the same procedures as for an Olympic athlete with some important alterations. These include additional preparations to assist transport of Para-athletes with mobility equipment, planning for alternative whole-body cooling methods if cold water immersion is deemed unsafe, and extra precautions and monitoring for athletes at risk of AD. We hope that event and team medical practitioners and Para athletes themselves are familiar with the prehospital management of EHS, since global warming poses a significant risk to Para sport competitions in the future.
What are the findings?
The incidence of exertional heat stroke (EHS) is relatively low among Paralympic athletes, but with increased global warming and interest to host world stage events in hot and humid environments the risk of EHS in Paralympic athletes may increase over time.
Medical providers are advised to review participating athletes’ impairment classification and categories prior to the event in order to apply impairment-specific considerations to safely treat Paralympic athletes with suspected EHS.
Paralympic athletes with autonomic dysfunction may experience altered thermoregulation, putting them at higher risk of EHS, as well as hypothermic overshoot during cold water immersion.
Athletes with significant mobility disability with suspected EHS may warrant whole-body cooling options other than cold water immersion to ensure safety and ease of care.
How might it impact on clinical practice in the future?
While the core principles of prehospital management of EHS for Paralympic athletes are no different from the standard care used in the general athletic context, extra caution may be required regarding specific physiological differences (eg, autonomic dysfunction) that impact the management of the altered or collapsed athlete.
Due to the heterogeneous athlete population, a thorough knowledge and awareness of the physiological and thermoregulatory responses in Paralympic athletes is required to optimise medical services at sporting events.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Marco Bernardi, Sergio Migliorini, Yoshi Kamijo, Fumihiro Tajima, Michelle Trbovich for their expert opinion and support.
References
Footnotes
Twitter @paolo_emilio, @bstephenson311, @SportswiseUK, @ephysiol, @wderman
Contributors YH, PEA, SB and VLG-T contributed to the conception or design of the work. YH, PEA and VLG-T drafted the manuscript. YH, PEA, BTS, CB, SB, NW, SR, WD and VLG-T critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests WD reports grants from IOC Research Centers Grant, other from IPC Travel Support, grants from World Rugby, grants from AXA, grants from Ossur, outside the submitted work.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.