Article Text

Abstract
Purpose To determine the potential associations between physical activity and risk of SARS-CoV-2 infection, severe illness from COVID-19 and COVID-19 related death using a nationwide cohort from South Korea.
Methods Data regarding 212 768 Korean adults (age ≥20 years), who tested for SARS-CoV-2, from 1 January 2020 to 30 May 2020, were obtained from the National Health Insurance Service of South Korea and further linked with the national general health examination from 1 January 2018 to 31 December 2019 to assess physical activity levels. SARS-CoV-2 positivity, severe COVID-19 illness and COVID-19 related death were the main outcomes. The observation period was between 1 January 2020 and 31 July 2020.
Results Out of 76 395 participants who completed the general health examination and were tested for SARS-CoV-2, 2295 (3.0%) were positive for SARS-CoV-2, 446 (0.58%) had severe illness from COVID-19 and 45 (0.059%) died from COVID-19. Adults who engaged in both aerobic and muscle strengthening activities according to the 2018 physical activity guidelines had a lower risk of SARS-CoV-2 infection (2.6% vs 3.1%; adjusted relative risk (aRR), 0.85; 95% CI 0.72 to 0.96), severe COVID-19 illness (0.35% vs 0.66%; aRR 0.42; 95% CI 0.19 to 0.91) and COVID-19 related death (0.02% vs 0.08%; aRR 0.24; 95% CI 0.05 to 0.99) than those who engaged in insufficient aerobic and muscle strengthening activities. Furthermore, the recommended range of metabolic equivalent task (MET; 500–1000 MET min/week) was associated with the maximum beneficial effect size for reduced risk of SARS-CoV-2 infection (aRR 0.78; 95% CI 0.66 to 0.92), severe COVID-19 illness (aRR 0.62; 95% CI 0.43 to 0.90) and COVID-19 related death (aRR 0.17; 95% CI 0.07 to 0.98). Similar patterns of association were observed in different sensitivity analyses.
Conclusion Adults who engaged in the recommended levels of physical activity were associated with a decreased likelihood of SARS-CoV-2 infection, severe COVID-19 illness and COVID-19 related death. Our findings suggest that engaging in physical activity has substantial public health value and demonstrates potential benefits to combat COVID-19.
- COVID-19
- physical activity
Data availability statement
Data are available on reasonable request. Study protocol, statistical code: available from DKYon (email: yonkkang@gmail.com). Data set: available from the National Health Insurance Service of Korea (NHIS-COVID-19 data) through a data use agreement.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
The COVID-19 caused by the novel SARS-CoV-2 has spread rapidly across the globe.1–3 Despite dedicated efforts to end the pandemic including vaccination and antiviral therapies based on blood products and antibody, the emergence of more than 5000 mutations and the continued second or more waves of infection have made the prevailing situation extremely complicated.4 Baseline characteristics of patients, including old age, obesity, heavy smoking status and underlying comorbidities, such as hypertension, respiratory disease, cardiovascular disease and cancer have been shown to be associated with increased risk of COVID-19 and COVID-19 related death.1–3 5 6 There is rapidly accumulating evidence on the risk factors for COVID-19 that are a function of interactions between the pathogen, host and environment. However, there is limited information about the impact of an individual’s level of physical activity, an important modifiable factor, on the potential infectivity and prognosis of COVID-19.
Physical activity is one of the leading determinants of health, and the lack of adequate physical activity is estimated to be responsible for 6%–10% of the global burden of major chronic diseases and 9% of premature deaths.7 Sufficient physical activity is known to be associated with substantially reduced risk for all-cause and disease-specific mortality,8 multiple chronic diseases (such as metabolic syndrome and type 2 diabetes),7 cancer7 and cardiovascular disease9 and improved physical function, cognition and quality of life.10 It is well established that regular and sustained participation in physical activity is beneficial for almost every facet of health, and the supporting evidence continues to grow.10 Moreover, previous studies have suggested that physical activity has a protective effect against infectivity and severity of respiratory infection due to its immunological benefits.11–13 The recently published Physical Activity Guidelines for Americans, second edition, which was originally proposed for preventing chronic disease-related mortality, provides a clear guidance on the types (such as aerobic and muscle-strengthening activity) and amount (eg, 150–300 min a week of moderate intensity of physical activity for adults) of physical activity that provides substantial health benefits.10
During the ongoing pandemic, measures taken by governments globally to control the transmission of COVID-19 include ‘lock downs’ and social distancing.14–16 This has substantially decreased people’s daily behaviours, routine and population levels of physical activity,17 which may lead to an unhealthy lifestyle.10 Previous studies had investigated the potential association between physical activity and COVID-19 with inconsistent results; no association with SARS-CoV-2 infectivity18 and COVID-19 severity,18 and beneficial association with COVID-19 severity19–21 have been found by various studies. Thus, the impact of physical activity on COVID-19 infectivity and clinical outcomes remains unclear.
Previous studies had described the health benefits of physical activity including those on the immune system.22 We established the hypothesis that this association will also apply to COVID-19, an infectious respiratory disease. Therefore, the aim of this study was to investigate the hypothesis that sufficient physical activity may reduce the risk of COVID-19 infectivity, severity and its related mortality among patients who underwent SARS-CoV-2 testing or decrease the length of hospital stay among patients confirmed with COVID-19. We used a large-scale, population-based, nationwide claim-based cohort data that included all patients who underwent laboratory testing for SARS-CoV-2 in South Korea.
Methods
Data source
We performed a high-quality, population-based, nationwide study using the data from the Korean National Health Insurance Service (NHIS) that includes data of all individuals who underwent SARS-CoV-2 testing in South Korea through services facilitated by the Korea Disease Control and Prevention Agency (KDCA) and Ministry of Health and Welfare, South Korea, between 1 January 2020 and 30 May 2020. The following link can be used to access the Korean NHIS site: https://nhissnhisorkr/bd/ab/bdaba000engdo/. The dataset links and consists of general health examination results, national COVID-19 related registers, including COVID-19 related outcomes and death records, and health insurance data for the past 5 years, including insurance eligibility data, outpatient and inpatient healthcare records, and pharmaceutical visits. The cohort dataset has the following characteristics: (1) the Korean government provided complimentary and mandatory health services and insurance to all Korean patients with COVID-191–3 5; (2) COVID-19 related death and outcome records were obtained by national COVID-19 related registers generated by the KDCA; and (3) all patient-related data were anonymised to ensure confidentiality from the Korean government.
Study population
The study population comprised all Korean individuals aged ≥20 years who underwent the SARS-CoV-2 testing between 1 January 2020 and 15 May 2020 by medical or KDCA referral (excluding self-referral (self-referred patients were tested anonymously for their privacy); n=212 768). Subsequently, we linked their national general health examination data between 1 January 2018 and 31 December 2019 to obtain the assessment on their level of physical activity. If the participants had multiple health examination data, the most recent was used. The total observational period was from 1 January 2015 to 30 July 2020, and individual index data were the data of the first SARS-CoV-2 testing for each patient. SARS-CoV-2 infection was confirmed by nasal and pharyngeal swabs using the laboratory real-time reverse transcriptase-PCR assay, which was authorised by the KDCA.1–3 5
Age, gender, household income and region of residence were obtained from insurance eligibility data. Smoking habits, frequency of alcohol consumption, physician-diagnosed history of diabetes mellitus, tuberculosis, stroke, cardiovascular disease, hypertension, dyslipidaemia and previous use of medication for hypertension, dyslipidaemia, diabetes mellitus and cardiovascular disease were obtained from general health examination, including self-reported questionnaires and personal medical interview. Body mass index and systolic and diastolic blood pressure were measured. Blood glucose and creatinine for estimating glomerular filtration rate and total cholesterol were obtained from fasting serum samples during general health examination. The Charlson comorbidity index was considered as reported previously.23
Exposures and outcomes
The leisure time physical activities of each participant was estimated during the general health examination and personal medical interview.23 Participants were asked to report the frequency of physical activity weekly in two categories: vigorous intensity physical activity is defined as intense exercise that causes severe shortness of breath (ie, running) and moderate intensity physical activity is defined as exercise that causes mild shortness of breath (such as brisk walking and bicycling). We calculated the time of physical activity in min/week by multiplying the frequency (times/week) and duration (min/time). Muscle strengthening was considered by frequency (times/week) using the following question according to physical activity guidelines10: ‘How often do you do muscle strengthening activities in a week, such as lifting weights or push-ups (times/week)’.
Aerobic physical activity was divided into two categories: recommended aerobic physical activity (≥150 min/week of moderate intensity activity or ≥75 min/week of vigorous intensity activity or greater than an equivalent combination) and insufficient aerobic physical activity (<150 min/week of moderate intensity activity, <75 min/week of vigorous intensity activity and less than an equivalent combination). Equivalent combination was calculated using the general rule that 2 min of moderate-intensity activity counts the same as 1 min of vigorous intensity activity.10 Muscle strengthening activity was divided into two categories: recommended muscle strengthening activity (≥2 times/week) and insufficient muscle strengthening activity (<2 times/week). Using these categories for aerobic and muscle strengthening physical activity, the level of physical activity was categorised into four: (1) insufficient aerobic activity and muscle strengthening; (2) muscle strengthening only (insufficient aerobic activity and recommended muscle strengthening activity); (3) aerobic only (recommended aerobic activity and insufficient muscle strengthening activity); and (4) aerobic and muscle strengthening (both recommended activity).
In addition, we categorised physical activity according to metabolic equivalent task (MET) score on the energy cost. Each category of activity was assigned a MET score on the energy cost, and the weighted MET-minutes per week was calculated by multiplying the standard MET score, duration and frequency per week.24 25 Ratings of 4.0 and 8.0 METs were assigned for moderate and vigorous intensity activity, respectively.24 25 The level of physical activity was categorised into four: (1) inactive (0 MET min/week), (2) insufficiently active (0–<500 MET min/week), (3) active (500–<1000 MET min/week) and (4) highly active (more than 1000 MET min/week).
We linked the study participants to the national COVID-19 related registers generated by KDCA. The outcomes examined were SARS-CoV-2 infection (positive laboratory SARS-CoV-2 testing result), severe clinical outcomes of COVID-19 (ICU admission, administration of invasive ventilation or COVID-19 related death),1–3 5 26 COVID-19 related death and/or length of hospital stay.
Eight cohorts studied
We generated the eight cohorts for robustness and generalisation of our results (online supplemental table S1 and figure 1): (1) cohort A was the main study that consisted of participants who received general health examination between 2018 and 2019 (online supplemental figures S1 and S2; n=76 395); (2) propensity score matched cohort A was performed by matching two groups (insufficient aerobic and muscle strengthening vs aerobic and muscle strengthening; n=5298); (3) cohort B consisted of only COVID-19 confirmed patients in cohort A (n=1293); (4) cohort C was conducted differential conditions of ‘exposure’ using the MET score (online supplemental figures S3 and S4; n)=76 395); (5) propensity score matched cohort C was performed by matching two groups (insufficient physical activity group (0–500 MET min/week) vs sufficient physical activity group (more than 500 MET min/week); n=59 986); (6) cohort D consisted of participants who received general health examination between 2015 and 2019 (online supplemental figures S5 and S6; n=118 768); (7) propensity score matched cohort D was performed by matching two groups (insufficient physical activity group (0–500 MET min/week) vs sufficient physical activity group (more than 500 MET min/week); n=23 860); and (8) cohort E consisted of only COVID-19 confirmed patients in cohort C (n=3882).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material

Participant profile in all cohort.
Participants in cohort A and B were categorised by exercise guideline and those in cohort C by MET score.10 The Korean general health examination has added a questionnaire about muscle strengthening as of 2018; we could not calculate muscle strengthening by using data from 2015 to 2017. Therefore, participants in cohorts D and E were categorised by MET score. If the participants had multiple health examination data, the most recent was used.
Sample size calculation
Although there has been no study on the association between SARS-CoV-2 infectivity and physical activity, we calculated the sample size based on a previous study on the relationship between COVID-19 severity and physical activity.21 We had originally calculated that for each group to have an 80% power to show a 2.8-fold improvement of severity among COVID-19 patients (1% in inactive group vs 2.8% in active group), at a 5% significance level, we would need to enrol 900 patients with COVID-19 in each group. Finally, we included 1293 patients with COVID-19 who engaged in insufficient physical activity and 1002 patients with COVID-19 who engaged in sufficient muscle strengthening, aerobic or both physical activities.
Statistical analyses
In the nationwide Korean cohort, ‘exposure’ was the physical activities according to physical activity guidelines10 in cohorts A and B or those according to MET score in cohorts C–E. The ‘primary end point’ was the positive SARS-CoV-2 testing results, severe COVID-19 illness or COVID-19 related death in cohorts A–E; the ‘secondary endpoint’ was the length of hospital stay among COVID-19 confirmed patients in cohorts B and E. The ‘individual index data’ were the data of first laboratory SARS-CoV-2 testing.
To assess the different confounding effects in our study, we used three sequential inclusion adjusting model by modified Poisson regressions presented by adjusted relative risks (aRRs) with 95% CIs or multivariable analysis of covariance presented by adjusted mean difference with 95% CIs. We also fitted a cubic spline model with four knots selected by the lowest Akaike information criterion.27 Furthermore, we confirmed the linearity assumption of systolic and diastolic blood pressure, fasting blood glucose and serum total cholesterol using Box-Tidwell test (all p value >0.05), the normality assumption of length of hospital stay using Kolmogorov-Smirnov test (p value >0.05) and homogeneity of variances assumption of length of hospital stay using Levene’s test (p value >0.05).
Model 1 was adjusted for age (20–39, 40–59 and ≥60 years) and sex. Model 2 was adjusted for age; sex; region of residence (Seoul Capital Area, Daegu/Gyeongbuk area and other area); Charlson comorbidity index (0, 1 and ≥2); history of diabetes mellitus, tuberculosis, stroke and cardiovascular disease; body mass index (continuous, using the cubic spline function); systolic blood pressure (continuous); diastolic blood pressure (continuous); fasting blood glucose (continuous); serum total cholesterol (continuous); glomerular filtration rate (≥90, 60–89 and ≤59 mL/min); household income (low, middle and high); smoking (never, ex and current); alcoholic drinks (<1, 1–2, 3–4 and ≥5 days per week); and medication for hypertension, diabetes mellitus and cardiovascular disease. Finally, model 3 was adjusted for minimal selected potential confounders by directed acyclic graph approach (figure 2; age, sex, region of residence, household income, smoking and alcoholic drinks).
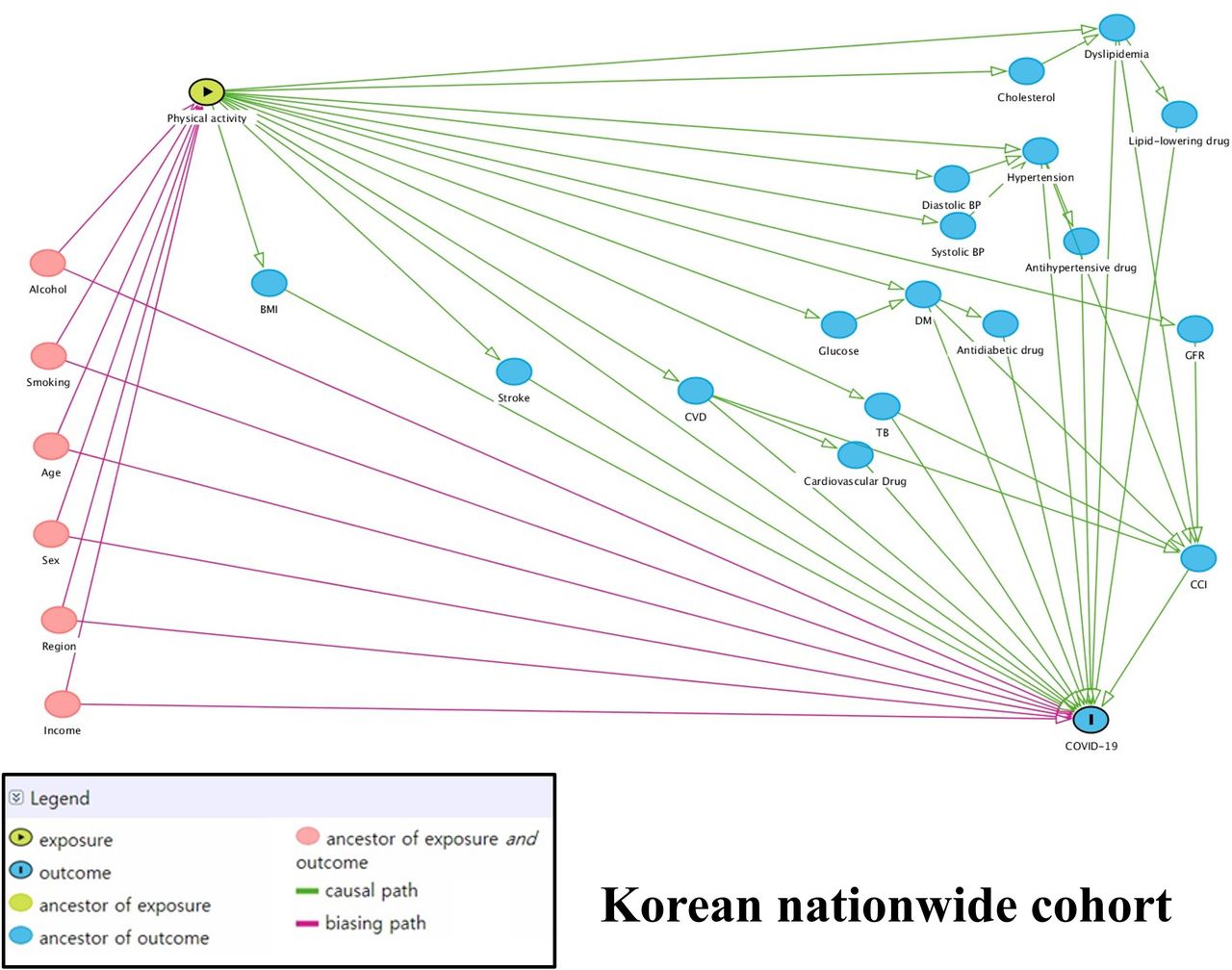
Directed acyclic graph demonstrating the implicitly assumed causal association between physical activity (‘exposure’) and risk of COVID-19 (‘outcome’) in the Korean nationwide cohort before matching. Confounders, potential mediators and exposure–outcome associations are indicated. BMI, body mass index; BP, blood pressure; CCI, Charlson comorbidity index; CVD, cardiovascular disease; GFR, glomerular filtration rate; TB, tuberculosis.
To test the stability and reliability of our results, we performed several analyses with multiple conditions. First, we analysed two differential conditions of ‘exposure’ such as using the physical activity guidelines10 (cohorts A and B) and MET score (cohorts C–E). Second, we performed propensity score matching three times to reduce potential confounding effects and to balance the baseline characteristics (matched cohort A: insufficient aerobic and muscle strengthening vs aerobic and muscle strengthening; matched cohorts C and D: insufficient physical activity group vs sufficient physical activity group). Propensity scores were derived using a logistic regression model with adjustment (model 2), and a ‘greedy nearest-neighbour’ algorithm was used to match patients in the two groups in a 1:1 ratio (random selection without participant replacement within specified calliper widths (0.01 SD)). We used robust SEs to obtain 95% CIs in matching analysis. Adequacy of matching was calculated by comparing standardised mean differences (SMDs) and propensity score density plot (online supplemental figures S7 and S9). An SMD of less than 0.1 indicates no major imbalance between the two groups.5 28 Third, we conducted the sensitivity analysis by generating cohorts B and E, including only patients with COVID-19. Fourth, to avoid overfitting issues, a directed acyclic graph approach was used to confirm adequate potential mediators, and thus, a visualisation of the causal relationship between physical activity (‘exposure’) and the risk of COVID-19 (‘outcome’) was provided. Fifth, we performed the subgroup analysis, in which there was stratification according to age, gender, smoking status and Charlson comorbidity index, which have a statistical significance of interaction (p interaction value <0.05). Finally, we used the Sidak’s correction for multiple comparisons to reduce the probability of type 1 error. Statistical analyses were performed using SPSS (V.25.0; IBM Corp, Armonk, New York, USA), R software (V.3.1.1; R Foundation, Vienna, Austria) and SAS (V.9.4; SAS Institute).23 29 Directed acyclic graphs were presented using Daggity (V.2.3; http://www.dagitty.net/). A two-sided p value of less than 0.05 was considered statistically significant.
Supplemental material
Supplemental material
Supplemental material
Patient and public involvement
No patients were directly involved in designing the research question or in conducting the research. No patients were asked for advice on interpretation or writing up of the results. There were no plans to involve patients or the relevant patient community in the dissemination of study findings at this time.
Results
Cohort A
Among 76 395 adults (age groups: 33.5% (20–39 years), 37.8% (40–59 years) and 28.7% (≥60 years); male, 48.8%), we identified 41 293 (54.1%), 5036 (6.6%), 18 994 (24.9%) and 11 072 (14.5%) adults with insufficient aerobic and muscle strengthening, muscle strengthening only, aerobic only and aerobic and muscle strengthening, respectively (table 1). During the observation period, 2295 (3.0%), 446 (0.58%) and 45 (0.059%) adults were diagnosed with COVID-19 (SARS-CoV-2 test positive), severe COVID-19 and COVID-19 related death, respectively (online supplemental table S11).
Baseline characteristics of patients who performed the SARS-CoV-2 testing in the Korean nationwide cohort (cohort A)
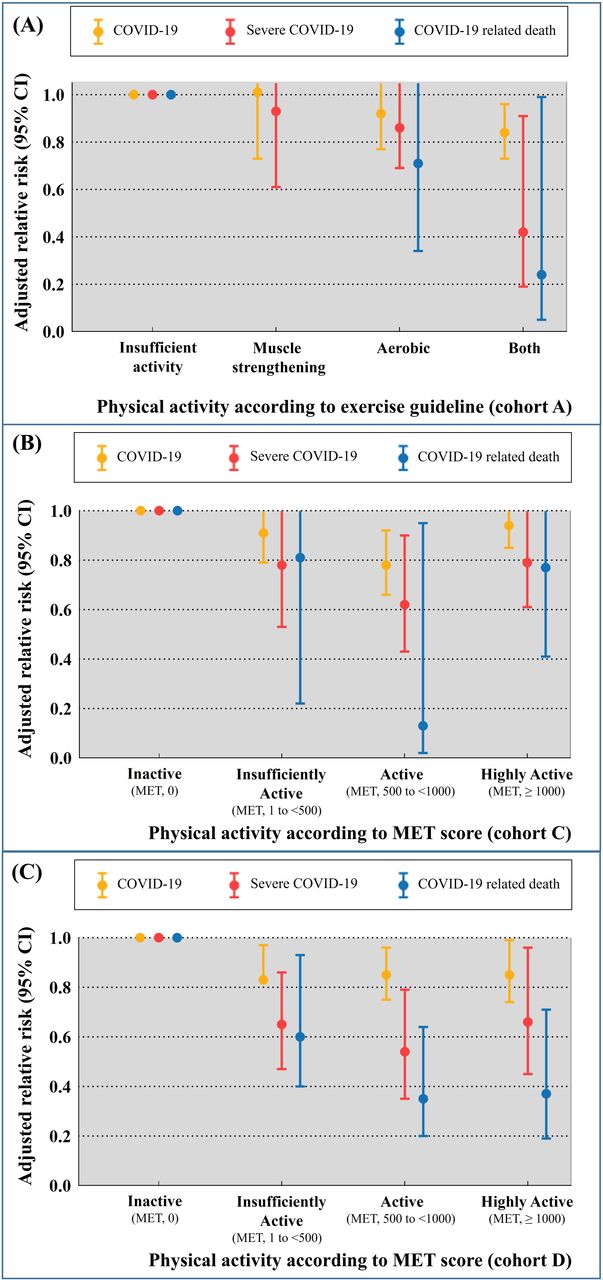
Table 2 and figure 3 show that adults with aerobic and muscle strengthening had a lower risk of COVID-19 infection (3.1% for insufficient aerobic and muscle strengthening vs 2.6% for aerobic and muscle strengthening; aRR (model 2) 0.85; 95% CI 0.72 to 0.98), severe COVID-19 (0.66% vs 0.35%; aRR (model 2) 0.42; 95% CI 0.34 to 0.91) and COVID-19 related death (0.08% vs 0.02%; aRR (model 2) 0.23; 95% CI 0.06 to 0.99). In subgroup analysis stratified by the covariates (table 3), the effect sizes of risk of COVID-19 infection between patients with insufficient aerobic and muscle strengthening and those with aerobic and muscle strengthening were stronger among middle aged adults (40–59 years; aRR 0.85; 95% CI 0.70 to 0.99), men (aRR 0.81; 95% CI 0.64 to 0.98), never smokers (aRR 0.79; 95% CI 0.58 to 0.94) and those having low Charlson comorbidity index (0 score; aRR 0.74; 95% CI 0.58 to 0.94) than in other groups. Similar effect sizes and patterns of severe COVID-19 were found among older adults (≥60 years; aRR 0.16; 95% CI 0.02 to 0.96), never smokers (aRR 0.44; 95% CI 0.23 to 0.99), and those having low Charlson comorbidity index (0 score; aRR 0.23; 95% CI 0.09 to 0.80). Moreover, we also found similar patterns after Sidak’s correction (online supplemental table S12).

{kind=link}
{kind=link}
{kind=link}
Association between physical activity according to 2018 physical activity guidelines for Americans and SARS-CoV-2 infection, severe COVID-19 illness and COVID-19 related death in cohort A. (A) Association between physical activity according to MET score and SARS-CoV-2 infection, severe COVID-19 illness and COVID-19 related death in cohort C (B) and cohort D (C). The level of physical activity was categorised into four: (1) inactive (0 MET min/week), (2) insufficiently active (0–<500 MET min/week), (3) active (500–<1000 MET min/week) and (4) highly active (more than 1000 MET min/week). Whiskers represent 95% CIs, and dots indicate full adjusted relative risks. MET, metabolic equivalent of task.
Adjusted relative risk (95% CIs) of SARS-CoV-2 infection, severe COVID-19 outcomes and COVID-19 related deaths associated with study patients who engaged in physical activities according to exercise guideline (cohort A)
Subgroup analysis of the association of SARS-CoV-2 infection and severe COVID-19 outcomes associated with study patients who engaged in physical activities according to exercise guideline
Matched cohort A
After 1:1 propensity score matching in cohort A (2649 for insufficient aerobic and muscle strengthening vs 2649 for aerobic and muscle strengthening), there were no major imbalances of baseline characteristics assessed by SMDs (online supplemental table S2; all SMDs ≤0.04). Those with aerobic and muscle strengthening had 27% lower risk of COVID-19 (aRR (model 2) 0.73; 95% CI 0.54 to 0.99) and 57% lower risk of severe COVID-19 (aRR (model 2) 0.43; 95% CI 0.20 to 0.95) than those with insufficient aerobic and muscle strengthening (table 4).
Sensitivity and additional analysis of the association of SARS-CoV-2 infection, severe COVID-19 outcomes and COVID-19 related death associated with study patients who engaged in physical activities according to exercise guideline or MET score
Cohort B
Among COVID-19 confirmed patients in cohort A (table 4 and online supplemental table S2; n=2295), we found that those with aerobic and muscle strengthening had a decreased risk of severe COVID-19 (aRR (model 2) 0.66; 95% CI 0.47 to 0.90) and length of hospital stay (adjusted mean difference, −2.08 days; 95% CI −4.04 to −0.14).
Cohort C
The 76 395 adults in cohort C were stratified according to MET score (table 4 and online supplemental table S4). The active group (500–<1000 MET min/week) was found to have 22% lower risk of COVID-19 infection (aRR (model 2) 0.78; 95% CI 0.66 to 0.92), 38% lower risk of severe COVID-19 (aRR (model 2) 0.62; 95% CI 0.43 to 0.90) and 83% lower risk of COVID-19-related death (aRR (model 2) 0.17; 95% CI 0.07 to 0.98) than the inactive group. The insufficiently active group and highly active group had a modest 9% and 6% lower risk of COVID-19 infection, 22% and 21% lower risk of severe COVID-19 and 19% and 21% lower risk of COVID-19-related death than the inactive group, respectively (figure 3).
Matched cohort C
We conducted a propensity score matched analysis to compare low physical activity group (0 to 500 MET min/week) with sufficient physical activity group (≥500 MET min/week). There were no major imbalances in baseline characteristics assessed by SMDs (table 4 and online supplemental table S6; all SMDs <0.07). In model 2, there was less SARS-CoV-2 infection (aRR 0.90; 95% CI 0.83 to 0.99) and severe COVID-19 (aOR 0.77; 95% CI 0.63 to 0.95) in the high physical activity group than in the low physical activity group. Moreover, we also found similar patterns after Sidak’s correction (online supplemental table S13).
Cohort D
Among 118 768 included adults, we identified 22 811 (19.2%), 50 052 (42.1%), 25 932 (21.8%) and 19 973 (16.8%) adults who were inactive, insufficiently active, active and highly active, respectively (online supplemental table S7). During the observation period, 3882 (3.3%), 277 (0.23%) and 122 (0.10%) adults were diagnosed with COVID-19 (SARS-CoV-2 test positive), severe COVID-19 and COVID-19 related death, respectively.
Online supplemental table S8 and figure 3 show that the active group (500–<1000 MET min/week) had 15% lower risk of COVID-19 infection (aRR (model 2) 0.85; 95% CI 0.75 to 0.96), 46% lower risk of severe COVID-19 (aRR (model 2) 0.54; 95% CI 0.35 to 0.79) and 65% lower risk of COVID-19-related death (aRR (model 2) 0.35; 95% CI 0.20 to 0.64) than the inactive group. However, the insufficiently active group and highly active group had a modest 11% and 15% lower risk of COVID-19 infection, 35% and 34% lower risk of severe COVID-19 and 40% and 63% lower risk of COVID-19 related death than the inactive group, respectively (table 4).
Matched cohort D
We conducted a propensity score matched analysis to compare low physical activity group (0–500 MET min/week) with sufficient physical activity group (≥500 MET min/week). There were no major imbalances in baseline characteristics assessed by SMDs (table 4 and online supplemental table S9; all SMDs <0.015). In model 2, there was less SARS-CoV-2 infection (aRR 0.87; 95% CI 0.76 to 0.99), severe COVID-19 (aOR 0.58; 95% CI 0.35 to 0.99) and COVID-19 related mortality (aOR 0.46; 95% CI 0.22 to 0.96) in the high physical activity group than in the low physical activity group.
Cohort E
Among the patients diagnosed with COVID-19 (n=3882), the risk of severe COVID-19 was less in the insufficiently active group (aRR (model 2) 0.73; 95% CI 0.53 to 0.99) and active group (aRR (model 2) 0.68; 95% CI 0.44 to 0.98) than in the inactive group. The COVID-19 related mortality among patients with COVID-19 was lower in the active group (aRR (model 2) 0.49; 95% CI 0.27 to 0.82) and highly active group (aRR (model 2) 0.43; 95% CI 0.22 to 0.83) than in the inactive group (table 4 and online supplemental table S10). The length of stay in hospital of patients with COVID-19 was lower only in the active group (adjusted mean difference, −1.85 day; 95% CI −3.63 to −0.05) than the inactive group, while no further benefits were observed in the insufficiently and highly active groups.
Discussion
Findings of our study
To our knowledge, this is the first large-scale, population-based, nationwide study that investigated the relationship of physical activity with the infectivity and severity of COVID-19 and its related death. In this nationally representative cohort study, we found that those who reported aerobic and muscle strengthening activities that met or exceeded the 2018 exercise guidelines had a lower risk of SARS-CoV-2 infection (aRR 0.85; 95% CI 0.72 to 0.96), severe COVID-19 illness (aRR 0.42; 95% CI 0.19 to 0.91) and COVID-19 related death (aRR 0.24; 95% CI 0.05 to 0.99) than those who did not. The effect sizes of these associations were significant among the elderly, men, never smokers and those having low Charlson comorbidity index. Furthermore, the recommended key target range of MET score (500–1000 MET min/week) was associated with the maximum beneficial effect size for the reduced risk of SARS-CoV-2 infection (aRR 0.78; 95% CI 0.66 to 0.92), severe COVID-19 illness (aRR 0.62; 95% CI 0.43 to 0.90) and COVID-19 related death (aRR 0.17; 95% CI 0.07 to 0.98). Interestingly, the length of stay in hospital was shortened about approximately 2 days in patients who performed both aerobics and muscle strengthening (adjusted mean difference: −2.08 days) or with MET 500–1000 MET min/week (adjusted mean difference: −1.85 days). These findings were consistent across a broad range of sensitivity and subgroup analyses using cohorts A–E or propensity score matching.
Comparison with previous studies
While several studies describe the health benefits of physical activity, most studies focused on non-communicable diseases.8 Few studies on physical activity and risk of respiratory infectious diseases have shown inconsistent results: beneficial association in USA (n=78 062)11 and Poland (n=1028)13 and no association in Denmark (n=5368),30 Sweden (n=2038)31 and USA (n=83 165).32 Furthermore, several intervention trials conducted in the USA, Brazil, Canada, Portugal, Spain and Turkey have produced non-conclusive and inconsistent results.33 Small sample size, heterogeneity of the study population, short-term follow-up period and inappropriate study design (ie, cross-sectional or uncontrolled cohort design) contributed to low levels of evidence and inconsistent results.11 13 30–33 However, a recent meta-analysis of 14 intervention trials suggested that exercise had a significant effect on the severity of symptoms and number of symptom days (mean difference −2.24 days), similar to our results. Moreover, a recent large meta-analysis including 55 studies suggested that physical activity is associated with a 31% and 37% risk reduction of community acquired infectious disease and its related mortality, respectively, which is consistent with our results.12
Though there are previous studies on the association between physical activity and the risk of COVID-19, the results are inconsistent; no association of physical activity with SARS-CoV-2 infectivity18 and COVID-19 severity18; and beneficial association with COVID-19 severity.19–21 Small sample size (patients with COVID-19, n=20718 or 246),19 uncontrolled cohort design,18–21 non-various definitions of physical activity,18–21 non-sophisticated statistical techniques to reduce several biases18–21 and different methods of collecting data for measuring exercise (24-hour movement patterns and self-reported questionnaire) contributed to inconsistent results in these studies (online supplemental table S14). Furthermore, most of the studies were conducted in the UK and USA18–21; the findings in Asia were unknown. These studies had explained the association using the hypothesis that regular physical activity is an important contributor to exercise capacity and favourably influences biological pathways that are involved with the body’s response to an infection, which is a consistent hypothesis supporting our results. Moreover, our study was primarily demonstrated the beneficial relationship between SARS-CoV-2 infectivity and physical activity.
Possible explanations of our results
Habitual exercise has the following beneficial effect on the immune system34: (1) enhanced immunosurveillance with an immune defence activity and metabolic health by increased immunoglobulins, anti-inflammatory cytokines (interleukin (IL)-6, IL-1ra and IL-10), neutrophils, cytotoxic T, immature B and natural killer cell subsets; (2) reduced systemic inflammation promoted by the recirculation of immune cells and mediates an anti-inflammatory and antioxidant state through multiple pathways; and (3) improved regulation of the immune system and delayed onset of immunosenescence. In addition, a previous study demonstrated that physical activity inhibits lung inflammation and bacterial colonisation in respiratory infectious disease involving IL-10/nuclear factor-κB.35 Recently, a study reported that physical activity helps to shift the balance of the ACE2 axis.36 It means that physical activity induces expression of ACE2 in skeletal muscle that leads to reduced circulating ACE2 that may have protective effect in susceptibility to SARS-CoV-2 and severity of COVID-19.36 The above-mentioned immunological benefits of exercise may prevent the infection, severity and death due to COVID-19.
Policy implication
Recent studies reported that total physical activity significantly decreased between immediately before and during the COVID-19 pandemic worldwide and across all age groups.17 Although research evidence continues to mount that decreased in physical activity during the COVID-19 pandemic is a critical threat to public health, its impact on infectivity and clinical outcomes has not been clearly defined. The results of this study demonstrated the importance of physical activity in decreasing the risk of infectivity, severity and mortality of COVID-19, so that it can be reflected in future guidelines. The WHO launched ‘#HealthAtHome’ campaign, including the recommendation of physical activity, to help manage weight and reduce the risk of non-communicable diseases such as cardiometabolic disease that can increase susceptibility to or severity of COVID-19.37 38 WHO recommended that people of all ages and abilities need to be as active as possible and encouraged people to engage in regular aerobic physical activity and bone and muscle strengthening activity.37
Strengths and limitations
There are several limitations in this study that need to be addressed. First, physical activity was assessed by self-report, which may lead to misclassification. Misclassification of physical activities by a self-report usually leads to regression dilution bias, which may lead to an underestimation of the magnitude of true association.22 Second, we can only assess the binary variable of muscle strengthening activity. Although frequency of muscle strengthening activity was not available, 2018 physical activity guidelines recommend only the use of binary variable (≥2 times/week), not frequency data. Third, the data of physical activity status was obtained at a single point of recent general health examinations and excluded light intensity physical activity. Furthermore, there is the possibility that individuals may tend to overestimate levels of physical activity on average with variations in possible effects, especially over longer periods of recall. However, the ‘exposure’ of physical activity can change at index data, which may influence the magnitude of the true association. Moreover, physical activity was only collected during leisure time; household and occupation-related physical activities were missing, which may influence the magnitude of true association.39 Future prospective cohort or interventional studies with serial and direct measurements of physical activity (ie, mobile exercise apps) are needed to investigate the true association between exercise and COVID-19. Fourth, although we adjusted a variety of covariates and matched using propensity score, we cannot exclude the possibility of unexpected confounding variables such as dietary patterns. To address this, we generated several cohort studies and performed several sensitivity analyses that may make our results robust and generalisable. Fifth, our results should be interpreted with caution since our study comprised only Asian patients (Korean), and ethnic prevalence of ACE2 polymorphism is different, which may affect the ACE2 axis. Finally, COVID-19 outcomes have improved over time, due to improvement in management,40 and our study was performed with data from the early stages of the pandemic. Further longitudinal studies are warranted. Sixth, measurement error in some confounders such as alcohol consumption and household income can result in residual confounding. Furthermore, the estimates are biased as the study did not capture the time-varying nature of both exposure and many of the confounders.41 Seventh, some estimated 95% CIs such as 0.05 or 0.06 in table 2 clearly suggest sparse data bias, which should be acknowledged as an important limitation.42 Although we used several analyses such as modified Poisson regressions model and matching analysis, it should be noted that the target effect of each analysis are different. While conditional effect is estimated in modified Poisson regressions, average effect in the exposed group is estimated in propensity score methods. Finally, patients with self-referral were tested anonymously to maintain privacy, and their data were unavailable in our database; therefore, exclusion of those with self-referral may have led to increase in selection bias.
Despite these limitations, this is the first large-scale, population-based, nationwide study to investigate the association between physical activity and risk of COVID-19 infectivity, severity and related death. Our data were collected from a large population that contains nationwide data of physical activity of over 100 000 individuals. To date, this is the first and largest analysis that focused on these relationships. We used the validated physical activity assessment according to the 2018 physical activity guidelines for Americans, and our data (such as previous medical history, body mass index, blood pressure and blood sample) were measured or obtained by medical staff during personal medical interview.
Conclusions
This study provides new evidence that physical activity, including both aerobic and muscle strengthening exercises, led to substantial reductions in the infectivity of SARS-CoV-2, risk of poor outcomes and death related to COVID-19. In particular, the effect sizes of these associations were significant among elderly, men, never smokers and those having low Charlson comorbidity index. However, the recommended key target range of MET score was associated with the maximum beneficial effect size for reduced the risk of SARS-CoV-2 infection, severe COVID-19 illness and COVID-19 related death. Interestingly, the length of hospital stay was shortened by approximately 2 days in patients who reported aerobic and muscle strengthening activities that met or exceeded the 2018 exercise guidelines (adjusted mean difference: −2.08 days) or those with MET 500–1000 MET min/week (adjusted mean difference: −1.85 days). The findings of the study suggest that public health policies and strategies to increase physical activity at the population level may reduce the risk of SARS-CoV-2 infection and minimise adverse consequences in patients with COVID-19. Encouraging individuals to maintain recommended levels of physical activity during the COVID-19 pandemic should be promptly and vigorously considered at the public health level.
Key messages
What are the findings?
Our results indicated that those who engaged in both aerobic and muscle strengthening activity according to 2018 exercise guidelines had a lower risk of SARS-CoV-2 infection (adjusted relative risk (aRR), 0.85; 95% CI 0.72 to 0.96), severe COVID-19 illness (aRR 0.42; 95% CI 0.19 to 0.91) and COVID-19 related death (aRR, 0.24; 95% CI 0.05 to 0.99) than those who did not.
Our findings reported that the recommended key target range of metabolic equivalent task (MET; 500–1000 MET min/week) was associated with the maximum beneficial effect size for reduced the risk of SARS-CoV-2 infection (aRR 0.78; 95% CI 0.66 to 0.92), severe COVID-19 illness (aRR 0.62; 95% CI 0.43 to 0.90) and COVID-19 related death (aRR 0.17; 95% CI 0.07 to 0.98). The length of stay in hospital was shortened about approximately 2 days in patients with both aerobic and muscle strengthening or with 500–1000 MET min/week.
How might it impact on clinical practice in the future?
The findings of the study suggest that public health policies and strategies to increase physical activity at the population level may reduce the risk of SARS-CoV-2 infection and minimise adverse consequences in patients with COVID-19.
Encouraging individuals to have active level of physical activity during the COVID-19 pandemic should be promptly and actively considered at the public health level.
Data availability statement
Data are available on reasonable request. Study protocol, statistical code: available from DKYon (email: yonkkang@gmail.com). Data set: available from the National Health Insurance Service of Korea (NHIS-COVID-19 data) through a data use agreement.
Ethics statements
Patient consent for publication
Ethics approval
The National Health Insurance Service-National Sample Cohort has ethical approval form the Institutional Review Board of Sejong University (SJU-HR-E-2020-003).
Acknowledgments
The authors appreciate healthcare professionals dedicated to treating patients with COVID-19 in Korea, the Ministry of Health and Welfare, the Health Insurance Review & Assessment Service of Korea and the National Health Insurance Service of Korea for sharing invaluable national cohorts in a prompt manner.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SWL and DKY are joint first authors.
Contributors DKY had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version before submission. Study concept and design: SWL, JIS and DKY; acquisition, analysis or interpretation of data: SWL, SYM, HYJ and DKY; drafting of the manuscript: SWL, JL, JIS and DKY; critical revision of the manuscript for important intellectual content: all authors; statistical analysis: SWL and DKY; study supervision: SWL, JIS and DKY. DKY is guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (NRF2019R1G1A109977913).
Disclaimer The funders had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.