Article Text

Abstract
Objective Ethnic differences in sudden cardiac arrest resuscitation have not been fully explored and studies have yielded inconsistent results. We examined the association of ethnicity with factors affecting sudden cardiac arrest outcomes.
Methods Retrospective cohort study of 3551 white, 440 black and 297 Asian sudden cardiac arrest cases in Seattle and King County, Washington, USA.
Results Compared with whites, blacks and Asians were younger, had lower socioeconomic status and were more likely to have diabetes, hypertension and end-stage renal disease (all p<0.001). Blacks and Asians were less likely to have a witnessed arrest (whites 57.6%, blacks 52.1%, Asians 46.1%, p<0.001) or receive bystander cardiopulmonary resuscitation (whites 50.9%, blacks 41.4%, Asians 47.1%, p=0.001), but had shorter average emergency medical services response time (mean in minutes: whites 5.18, blacks 4.75, Asians 4.85, p<0.001). Compared with whites, blacks were more likely to be found in pulseless electrical activity (blacks 20.9% vs whites 16.6%, p<0.001), and Asians were more likely to be found in asystole (Asians 41.1% vs whites 30.0%, p<0.001). One of the strongest predictors of resuscitation outcomes was initial cardiac rhythm with 25% of ventricular fibrillation, 4% of patients with pulseless electrical activity and 1% of patients with asystole surviving to hospital discharge (adjusted OR of resuscitation in pulseless electrical activity compared with ventricular fibrillation: 0.30, 95% CI 0.24 to 0.34, p<0.001, adjusted OR of resuscitation in asystole relative to ventricular fibrillation 0.21, 95% CI 0.17 to 0.26, p<0.001). Survival to hospital discharge was similar across all three ethnicities.
Conclusions While there were differences in some prognostic characteristics between blacks, whites and Asians, we did not detect a significant difference in survival following sudden cardiac arrest between the three ethnic groups. There was, however, an ethnic difference in presenting rhythm, with pulseless electrical activity more prevalent in blacks and asystole more prevalent in Asians.
Statistics from Altmetric.com
Introduction
Sudden cardiac arrest (SCA) is a major public health problem accounting for approximately 424 000 deaths annually in the USA.1 Despite progress in treatment and prevention of coronary heart disease, and advances in cardiopulmonary resuscitation (CPR), SCA remains a leading cause of mortality due to its high fatality.2 ,3
The burden of SCA differs across ethnic groups: numerous studies have shown that blacks have a higher incidence of SCA compared with whites.4–10 Some, but not all, studies suggest that blacks have poorer SCA survival compared with whites.4 ,6 ,8 ,11–13 While some studies posit that the increased SCA mortality among blacks is inherent to the ethnic group,4 ,6 ,14 others report that it is in part due to socioeconomic status with those in the lower socioeconomic strata at higher risk of mortality.15 ,16 Several studies have concluded that the survival differences between races are due to disparities in favourable SCA circumstances such as having a witnessed arrest, or healthcare-related factors such as receiving bystander CPR and shorter emergency medical services (EMS) response time.8 ,11–13 ,17–25 Additionally, it has been noted in some but not all studies that the presenting rhythm differs between the ethnicities, with a lower proportion of blacks and Asians in ventricular fibrillation (VF),4 ,6 ,8 ,11 ,12 ,26 a rhythm associated with better outcomes.7 Lastly, one study suggested that blacks receive fewer proven lifesaving interventions post-SCA, such as coronary angioplasty and cardioverter defibrillator (ICD) implantation.27
These discrepancies merit further investigation, to shed light on the complex pathophysiology of SCA and to identify potential health services differences, and to improve management and prevention strategies across all ethnicities. We examined a cohort of SCA cases (3551 whites, 440 blacks and 297 Asians) attended by paramedics in Seattle and King County from 1988 to 2009. Our goal was to investigate the association of ethnicity with factors that affect SCA outcomes, including sociodemographic characteristics, underlying medical co-morbidities, SCA circumstances such as presenting rhythm, and medical care such as duration of resuscitation.
Methods
Study population
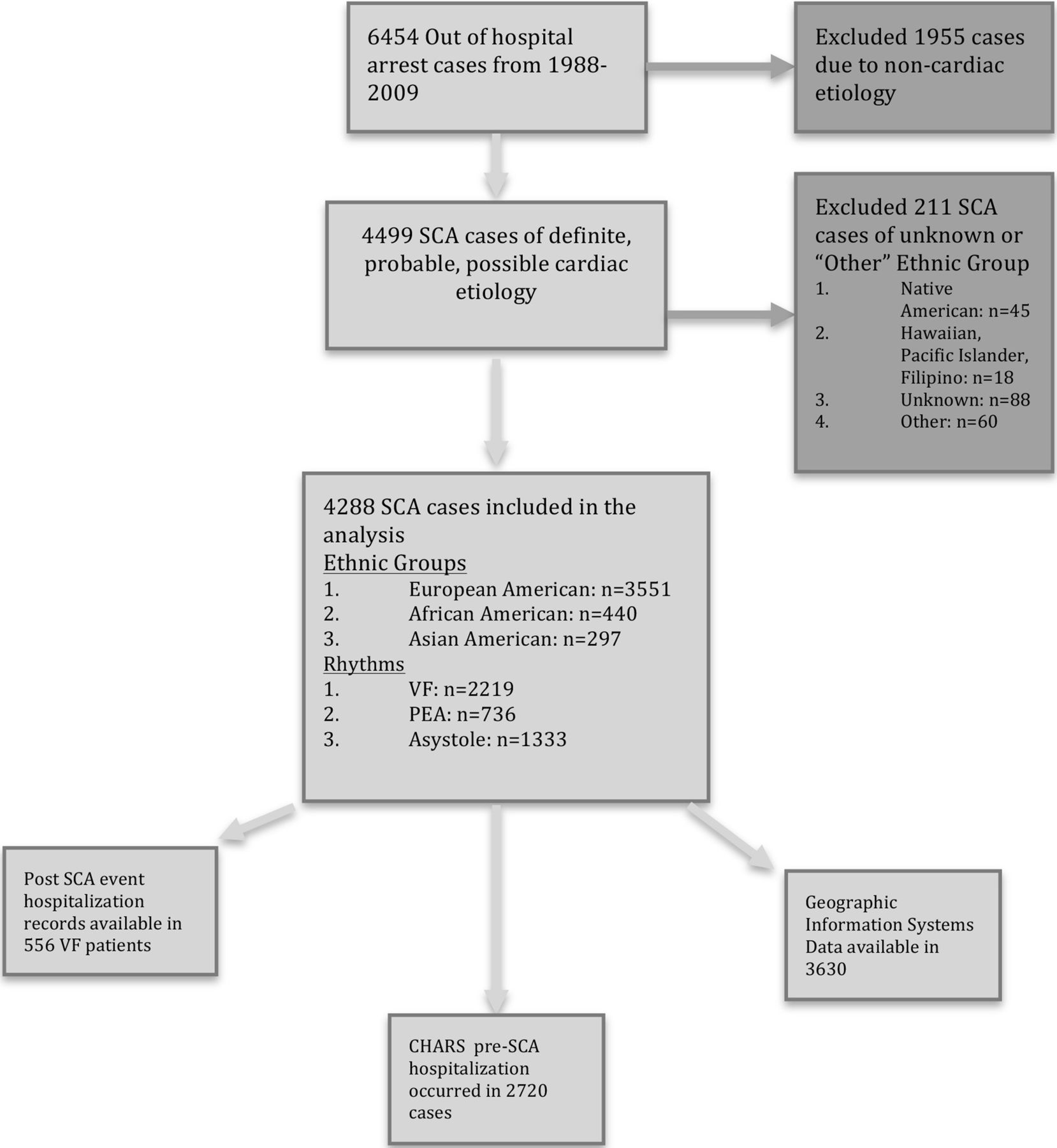
We studied cases of out-of-hospital arrest attended by paramedics in Seattle and King County, Washington between 1988 and 2009 as part of the Cardiac Arrest Blood Study repository (CABS-R).28 SCA was defined as a sudden pulseless condition presumed due to an arrhythmia in the absence of any evidence of a non-cardiac cause of the arrest. Exclusion criteria for the CABS-R were age <18, temperature below 34°C on arrival and incarcerated or pregnant individuals. From 6454 out-of-hospital arrest cases collected, we excluded cases with an evident acute non-cardiac morbidity that could account for the arrest, such as drug overdose, stroke, aortic aneurysm rupture, other acute bleeding, acute respiratory failure or trauma. To minimise misclassification of phenotype, we excluded cases with chronic terminal illnesses including terminal cancer or end-stage liver disease (n=1955 excluded, figure 1). Cases were adjudicated as definite, probable or possible cardiac arrest. For this study, we included all three groups in the case definition. Sensitivity analyses were run excluding those in the possible cardiac arrest group.
{kind=link}
Flow chart depicting case inclusion, and data available on such cases. CPR, cardiopulmonary resuscitation; PEA, pulseless electrical activity; EMS, emergency medical services.
Ethnicity was ascertained by paramedic incident reports, hospital medical records and death certificates, and we limited our analysis to three ethnic groups: Americans of primarily European descent (here referred to as whites, n=3551), Americans of primarily African descent (here referred to as blacks, n=440) and Americans of primarily East Asian descent (here referred to as Asians, n=297). We excluded those with unknown ethnicity or other ethnic groups from our study (n=211).
By definition, location of arrest was out-of-hospital, which included arrests occurring in clinic settings as well as assisted living and skilled nursing facilities. Sensitivity analyses were performed excluding these latter cases.
Data were obtained from: (1) EMS incident reports, available for all cases; (2) postarrest hospitalisation data from the EMS quality assurance review, available for 556 cases with VF; (3) the Washington State Comprehensive Hospital Abstract Reporting System (CHARS) database of hospital discharge diagnoses, available for 2720 cases and (4) Geographic Information Systems data for socioeconomic variables, available for 3630 cases (figure 1).
Covariate definitions
Socioeconomic information was based on 1999 US census tract estimates obtained by using the address of residence for each case obtained from death certificate/EMS incident report/hospital records, and included median household income, proportion of residents under the 1999 threshold for poverty and the proportion of adult residents not graduated from high school.
CHARS data were used to classify clinically recognised pre-SCA chronic health conditions. Sixty-three per cent of our cases had one or more prior hospitalisation records in CHARS from 1988 to 2009 from which we obtained information about past discharge diagnoses of myocardial infarction (MI), heart failure (HF), ischaemic or haemorrhagic stroke, atrial fibrillation, renal failure, pulmonary disease, as well as admissions for the following procedures: coronary angiogram, coronary angioplasty and coronary artery bypass graft (CABG) surgery. Those admitted without these diagnoses/procedures, and those without any record of hospital admissions, were regarded as not having a history of these conditions. Additionally, the diagnoses of hypertension and diabetes were examined in a subgroup analysis restricted to the 63% of cases with hospital records (n=2720), to avoid the assumption that people for whom hospitalisation data were missing are free of these conditions.
The presenting rhythm was the first observed rhythm when EMS personnel applied a defibrillator, classified into three categories: VF, pulseless electrical activity (PEA) and asystole. Thirty ventricular tachycardia cases were included in the VF category. Complete heart block was included in the PEA group. Public location of arrest was defined as an indoor or outdoor public location where others could have witnessed the arrest. Bystander CPR was defined as documented receipt of CPR prior to EMS arrival. EMS response time was measured from dispatch time to arrival on scene. Resuscitation duration was measured from the initiation of EMS care until cessation of resuscitation efforts by EMS personnel. If resuscitation efforts had not ceased, then the duration was measured up to arrival at the hospital. Postevent hospitalisation records, collected on a subset of VF cases only, provided data on post-SCA medical services.
Outcome definitions
Circulatory resuscitation was defined as survival to hospital admission; cases that expired in the field or the emergency department were considered not to have been successfully resuscitated. Survival was defined as discharge from the hospital alive.
Statistical analysis
For unadjusted analyses, we compared sociodemographic characteristics, inpatient medical history, SCA circumstances and medical care among three ethnic categories using Pearson χ2 test for categorical or binary variables, and ANOVA for continuous variables.
For adjusted analyses of the association of ethnicity with outcomes of SCA, we used logistic regression with robust SEs to estimate OR, 95% CIs and p values. In model 1 we adjusted for age, gender and event year, and in model 2 we added presenting rhythm. In model 3 we included variables we had chosen a priori that are associated with SCA outcomes based on previously published literature,7 ,20 specifically: location of arrest, witnessed arrest, bystander CPR, EMS response time interval. In model 4 we included prior inpatient medical co-morbidities (MI, HF, stroke, atrial fibrillation, renal failure and lung disease). In all models, whites served as the reference group.
Given the strong association of presenting rhythm with resuscitation and survival from SCA, we used multinomial logistic regression with robust SEs to identify predictors of the three presenting rhythms as the outcome, with VF as the reference group. As a secondary analysis, we created a second regression model limited to the subgroup of cases with hospitalisation records, to evaluate the associations of prior history of hypertension and diabetes with the presenting rhythms. Lastly, we tested for effect modification of risk factors by ethnicity.
Due to the multiple testing being performed in our analyses, we chose a p value of 0.01 as a threshold for statistical significance to reduce type I error. STATA V.13 was used for all statistical analyses.
This study was conducted with the approval of the University of Washington Institutional Review Board.
Results
Demographic characteristics, prior medical co-morbidities and SCA circumstances
The cohort of SCA cases included 3551 whites, 440 blacks and 297 Asians. Black cases were younger than white and Asian cases, and, on average, blacks and Asians had lower average census tract-defined education and income than whites (table 1). We examined ethnic differences in co-morbidities requiring hospitalisation among the cases prior to their arrest (table 1). Blacks had the lowest proportion hospitalised with atrial fibrillation, and blacks and Asians had a larger proportion of cases with hypertension, diabetes mellitus and end-stage renal disease during a previous hospitalisation compared with whites (p<0.0001). However, there was little or no difference in the proportion previously hospitalised with coronary artery disease (CAD) diagnoses or procedures among the three ethnic groups.
Demographic characteristics and co-morbidities obtained from pre-event hospitalisation records of patients with sudden cardiac arrest (SCA) in Seattle/King County, 1988–2009
At the time of SCA, black and Asian individuals were less likely to be found in VF compared with white SCA cases (table 2, 53% whites, 46% blacks and 41% Asians were found in VF). Blacks had a higher proportion of PEA as presenting rhythm, while Asians had a higher proportion of asystole compared with whites (table 2). Additionally, blacks were the least likely to receive bystander CPR and Asians were the least likely to have a witnessed arrest (table 2).
Ethnic differences in sudden cardiac arrest event characteristics
Acute care during SCA and postresuscitation care
Except for response time (table 2), which was shorter for blacks and Asians compared with whites, there were no statistically significant differences in healthcare delivery among the three ethnic groups, with comparable defibrillatory shocks for VF, drug therapies administered for each separate rhythm and duration of resuscitation (table 3, all p>0.01). Post-SCA hospital care was only measured on a modest proportion of eligible patients (461 whites, 58 blacks and 37 Asians), however, from the available data, a similar trend was noted in medical care delivered to all three groups after their hospitalisation with SCA (table 3). Among VF cases, all three ethnicities had similar rates of coronary catheterisation (46% whites, 35% blacks and 38% Asians). In patients with VF who survived to hospital discharge, there was no significant difference in the proportion that received CABG surgery (13% whites, 12% blacks and 7% Asians) or ICD (34% whites, 40% blacks and 24% Asians) prior to hospital discharge by ethnic group. There was a suggestion of fewer coronary angioplasties among black compared with white or Asian cases (15% whites, 2% blacks, 16% Asians, p=0.02), but the small sample size limited the power to find an association that exceeded our preset threshold for significance.
Ethnic differences in sudden cardiac arrest care, by presenting rhythm*†
Association of ethnicity with survival to hospital admission and hospital discharge
Approximately 45% of VF cases survived to hospital admission (successful resuscitation), and 25% survived to hospital discharge. By comparison, only 4% of PEA cases and 1% of asystole cases survived to hospital discharge (see online supplementary table S1). In unadjusted analyses, there were no differences in resuscitation and survival among the three ethnic groups overall and when stratified by presenting rhythm (see online supplementary table S1). In multivariable analyses, accounting for various SCA characteristics did not alter the lack of association of ethnicity with SCA outcomes (table 4, see online supplementary table S2 and figure S1). It also showed that the strongest predictors of survival included presenting rhythm, with worse survival in PEA and asystole relative to VF (see online supplementary table S2: PEA vs VF OR 0.15, CI 0.10 to 0.22, p<0.001, asystole vs VF OR 0.04, CI 0.02 to 0.08, p<0.001). Other predictors of worse survival were older age, male gender, non-public location of arrest, unwitnessed arrest and longer EMS response time. None of the medical co-morbidities examined showed an association with survival in multivariable analyses (see online supplementary table S2 and figure S1). Excluding assisted living and skilled nursing facility cases in sensitivity analyses did not significantly alter these findings (data not shown).
Supplementary table
Unadjusted and multivariable adjusted models for resuscitation to hospital admission and survival to hospital discharge in blacks and Asians relative to whites*
Association of patient characteristics and arrest circumstances with presenting rhythm
Because presenting rhythm is strongly associated with resuscitation outcomes, we examined patient characteristics and arrest circumstances associated with presenting rhythm (table 5 and see online supplementary tables S3 and S4). In multivariable analysis, PEA and asystole cases tended to be older and were less likely to be male compared with VF cases (table 5 and see online supplementary table S4). PEA and asystole cases had longer EMS response times and were less likely to have had a witnessed arrest in a public place than VF cases. Also, PEA and asystole cases tended to have less prior cardiovascular disease than VF cases but were more likely to have renal failure, lung disease, hypertension or diabetes (table 5 and see online supplementary table S4). No statistically significant effect modification by ethnicity was found (data not shown).
Covariates associated with presenting rhythm (multivariable model) comparing PEA and asystole with ventricular fibrillation
Discussion
Our large SCA cohort study showed no ethnic difference in successful resuscitation in the field or survival to hospital discharge, despite blacks and Asians having a higher prevalence of a number of unfavourable circumstances and characteristics associated with worse SCA resuscitation outcomes. While lack of sufficient power to detect a difference in outcomes may account for differences between our study findings and those described in prior reports, the 95% CI range of our findings suggest that compared with whites, blacks may have at most a 20% decreased survival, but up to a 54% increased chance of survival. These findings differ from prior reports that have found up to twofold decrease risk of survival among blacks.6 This study suggests the possibility that with optimal prehospital care, outcomes of SCA among ethnic groups can be similar despite underlying differences in some prognostic factors.
Blacks and Asians in our study have a higher percentage of a number of characteristics associated with worse resuscitation outcomes, including lower socioeconomic status, presenting rhythms of PEA and asystole, unwitnessed events and less likelihood of receiving bystander CPR; as well as some characteristics associated with more favourable resuscitation outcomes including younger age and shorter response times. The ethnic differences in patient characteristics and SCA circumstances in our study were largely similar to prior published reports.4 ,6 ,8 ,11–13 ,26 ,29 Furthermore, the proportion of black and Asian SCA cases presenting in VF was lower than for white cases, corroborating findings of other studies.4 ,8 ,11 ,26 We found shorter EMS response times for blacks and Asians compared with whites, perhaps due to closer medic unit base location to these communities in Seattle. Given the strong association of SCA survival with response times, this may partly explain the comparable survival rates across ethnicities in our study.
Notably, we did not find any evidence of ethnic disparities in healthcare delivery including duration of resuscitation. Additionally, in contrast to a prior published report, there was no statistically significant ethnic difference in either CABG surgery or ICD implantation among VF survivors,27 however we note that we lack data on a large number of eligible patients in post-SCA hospital care.
Presenting rhythm was a key predictor of outcome, with better survival for VF relative to PEA and asystole. Our study demonstrates that ethnicity was a strong predictor of presenting rhythm in SCA cases; the association of blacks with PEA remained even after adjustment for co-morbidities and circumstances surrounding SCA that influence rhythm, such as unwitnessed arrest. While the disproportionate amount of renal disease, lung disease, hypertension and diabetes mellitus in both blacks and Asians might partially explain this difference, further investigation is warranted to better understand how clinical conditions, event circumstances and acute pathophysiology influence ethnic differences in presenting arrest rhythm.
A number of strengths of this study should be noted. First, our study setting of Seattle and King County minimises the effect of inadequate or inconsistent prehospital care as a factor in ethnic differences in SCA outcomes. Additionally, the out-of-hospital arrest cases from the Cardiac Arrest Blood Study were rigorously reviewed, and only cases adjudicated to have a cardiac aetiology were included in the main analyses, to allow for a more uniform phenotype and exclude misclassification bias. Furthermore, this is also the first study to examine characteristics and outcomes for Asians, in addition to blacks and whites.
Several limitations deserve consideration. First, unlike prior published reports, our cohort has a higher proportion of shockable rhythms, which is partly a reflection of our definition of SCA and rigorous adjudication of SCA cases to only include those with primary cardiac aetiology, which are likely to present in ventricular tachycardia (VT)/VF, however such a dissimilarity should not affect our question of interest. It is also partly a reflection of faster EMS response time, as VT/VF can degenerate into asystole over minutes, and while the community's advanced EMS care is a strength, it limits the study's generalisability to other locations around the country. Second, our study's sample size, although large compared with many prior published reports, is still limited. Third, we lacked individual income, education and poverty data, and instead used census tract information from 1999 US Census data. Furthermore, the ethnic differences in medical co-morbidities might be underestimated in blacks or Asians, who may have less access to healthcare, leading to inaccurate classification. While we had rigorous hospitalisation data prior to the cardiac arrest, we did not have uniform access to outpatient medical records to ascertain chronic medical co-morbidities that do not require hospitalisation, which likely resulted in incomplete adjustment for confounding by underlying medical conditions. Furthermore, we did not have uniform access to autopsy data for all SCA cases, therefore we were unable to comment on the pathophysiology underlying the ethnic differences in presenting rhythms of SCA. We additionally lack preclinical imaging data, such as electrocardiogram and echocardiography data, prior to arrest on the majority of cases. While we have detailed information on EMS care and response times, response time is measured from EMS dispatch to arrival on scene and does not take into account the time from the arrest until 911 is called. Whether there are ethnic differences in time from arrest until 911 is called is unknown. Finally, we have insufficient captured information on hypothermia protocol in SCA cases.
In summary, our study, set in Seattle and King County Washington, with an effective and mature emergency medical care system did not find evidence of a difference in survival post-SCA among blacks and Asians compared with whites.30 This finding contrasts to prior reports suggesting lower survival among blacks. There is a difference by ethnicity in presenting rhythm, one of the strongest predictors of survival, with more PEA among blacks, and more asystole among Asians. Further investigation of the underlying pathophysiology of SCA cases, including autopsy data, and more detailed medical history, including EKG and echocardiographic data, is needed to better understand these ethnicity-specific differences in presenting rhythms. Additionally, continued research is needed in ethnicity-specific healthcare delivery and infrastructure that may influence cardiac arrest outcomes.
Key messages
What is already known on this subject?
Sudden cardiac arrest (SCA) is a major public health problem and some studies have shown that blacks have higher incidence of SCA as well as worse survival rates, these ethnic differences have not been fully explored.
What might this study add?
Our large SCA cohort study showed no ethnic difference in SCA survival to hospital discharge (multivariable adjusted OR for blacks vs whites, 1.11, 95% CI 0.79 to 1.54; for Asians vs whites, OR 1.33, 95% CI 0.87 to 2.05), despite blacks and Asians having a higher prevalence of a number of unfavourable circumstances and characteristics associated with worse SCA resuscitation outcomes. This study also shows that there is a difference by ethnicity in presenting rhythm, one of the strongest predictors of survival, with more pulseless electrical activity among blacks (blacks 20.9% vs whites 16.6%, p<0.001), and more asystole among Asians (Asians 41.1% vs whites 30.0%, p<0.001).
How might this impact on clinical practice?
The findings of our study suggest that with optimal prehospital care, outcomes of SCA among ethnic groups can be similar despite underlying differences in some prognostic factors and that there is no increased mortality inherent to a specific ethnicity. In addition, there needs to be further research into the ethnic differences in presenting rhythms of SCA.
Acknowledgments
Joanna Ghobrial, MD, MS and Nona Sotoodehnia, MD, MPH had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors listed have contributed sufficiently to the project to be included as authors.
References
Footnotes
Contributors JG and NS conceived the idea of the study. JG, NS and SRH initiated the study design and its implementation. NS is the grant holder. JG, NS and TMB provided statistical expertise in observational study design and JG conducted the primary statistical analysis. All authors contributed to refinement of the study protocol and approved the final manuscript.
Funding Grants from the National Heart, Lung, and Blood Institute (NHLBI): HL111089, HL088456, HL088576, HL091244 and HL092111. Additional funding was provided by the John Locke and Medic One Foundations.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from the CABS-R study are available to Cardiovascular Health Research Unit investigators based at the University of Washington, Seattle, Washington, USA. The data are also available to collaborators when requested.