Article Text

Abstract
Background This study investigated the influence of African/Afro-Caribbean (black) ethnicity on the clinical profile and outcomes in hypertrophic cardiomyopathy (HCM).
Methods 425 consecutive patients with HCM (163 black and 262 Caucasians (white); mean age 52.5±16.6 years) were assessed at three cardiomyopathy centres. Repeat assessments were performed every 6–12 months and mean follow-up was 4.3±3.0 years. The primary outcome was a composite of cardiovascular death, cardiac arrest or appropriate device therapy.
Results A fortuitous diagnosis of HCM was more commonly made in black compared with white patients (31.3% vs 19.1%, p=0.004). An abnormal ECG at presentation was more frequent in black patients (98.2% vs 90.5%, p=0.002), with T-wave inversion being a common feature (91.4% vs 73.0%, p<0.001). Asymmetric septal hypertrophy was the predominant pattern in both ethnic groups; however, apical (22.2% vs 10.7%, p<0.001) and concentric (9.3% vs 1.5%, p<0.001) patterns were more prevalent in black patients. Hypertension was more frequent in black patients (58.3% vs 31.7%, p<0.001). There were no ethnic differences in risk factor profile or primary outcome. Independent predictors of the primary outcome were non-sustained ventricular tachycardia (HR 6.03, 95% CI 3.06 to 11.91, p≤0.001) and hypertension at presentation (HR 2.02, 95% CI 1.05 to 3.88, p=0.036), with an additive effect.
Conclusion Black ethnicity is an important determinant of the phenotypic expression of HCM but does not adversely affect outcomes. Apical and concentric hypertrophy are common in black patients and may hinder the identification of HCM in this cohort. Hypertension has an adverse effect on outcome, irrespective of ethnicity.
Statistics from Altmetric.com
Introduction
Hypertrophic cardiomyopathy (HCM) is recognised for its diverse phenotypic expression.1 The influence of ethnicity on clinical and morphological features is unknown. Observations from athletes2 ,3 and hypertensive patients4 ,5 reveal that individuals of African/Afro-Caribbean origin (black) ethnicity exhibit a higher prevalence of ECG repolarisation changes and left ventricular hypertrophy (LVH) compared with Caucasian (white) individuals. This combination creates diagnostic challenges with respect to the differentiation of morphologically mild HCM from other causes of LVH in this ethnic group.2 ,5 The issue is confounded by the high prevalence of hypertension in the black population,6 which has been associated with poor outcomes in white HCM cohorts.7 Furthermore, reports from the USA reveal that deaths from HCM are more prevalent among black athletes,8 raising the possibility that HCM exhibits a more malignant course in black individuals. This study sought to address differences in the clinical phenotype, risk factor profile and outcome of HCM between black and white patients.
Methods
Patient selection and definitions
Between 2001 and 2014, 425 consecutive patients with HCM (262 (61.6%) white and 163 (38.4%) black) were assessed in three specialist cardiomyopathy clinics in London, UK. These clinics serve regions with a diverse ethnic composition where the population of black individuals reaches 30%–40%. Ethnicity was self-assigned. Ethical approval was obtained from the local research ethics committee and all patients gave informed consent to participate in the study. Patients were diagnosed after either: (1) primary care referral for symptoms and/or the detection of a cardiac murmur; (2) investigation for an abnormal ECG; (3) cascade screening of family members of patients with HCM; (4) referral from another hospital for specialist evaluation or (5) presentation with cardiac arrest.
HCM was diagnosed on the basis of LVH ≥15 mm in any myocardial segment on echocardiography and/or cardiac MRI (CMRI), in the absence of another condition capable of producing the same magnitude of LVH.9 Patterns of LVH were categorised according to the location of the myocardial segment revealing the greatest degree of hypertrophy on echocardiography and/or CMRI. Concentric LVH was categorised as global myocardial hypertrophy with <2 mm difference between adjacent segments. In cases of mild (<15 mm) LVH (n=60; 14.1%), HCM was diagnosed in the context of supportive features, including: (1) an established pathogenic gene mutation (n=30); (2) a family history of HCM or sudden cardiac death (SCD) in a first-degree relative (n=17); (3) LVH confined to the apical segments (n=12); (4) presentation with cardiac arrest in the presence of mild asymmetric septal hypertrophy and unobstructed coronary arteries (n=1).
Hypertension was defined according to the Seventh Joint National Committee criteria10 as a blood pressure (BP) of ≥140/90 mm Hg on an average of two or more properly measured seated BP readings and/or patients on established antihypertensive therapy. Good BP control was assessed by clinic visit and general practitioner BP measurement records in addition to 24-hour ambulatory BP monitoring. Among patients with a history of hypertension (n=178; 41.9%), HCM was diagnosed in the presence of severe LVH ≥20 mm (n=36) or in the context of LVH ≥15 mm in any myocardial segment and supportive features, including: (1) an established pathogenic gene mutation (n=31); (2) a family history of HCM or SCD in a first-degree relative (n=32); (3) non-concentric, segmental patterns of LVH confined to the apical segments (n=35), mid-septum (n=24) or anterior wall (n=3) and (4) systolic anterior motion of the mitral valve leaflets (n=17).9 ,11–13
Clinical evaluation
All patients were investigated with history, physical examination, 12-lead ECG, two-dimensional echocardiography, exercise testing and 24-hour ambulatory ECG monitoring. A total of 246 patients (58%) underwent CMRI. All patients had repeat assessment on a 6–12 monthly basis. Analysis relating to ECG and structural data was performed on the presenting investigations. Data from study entry to the last contact in clinic or death were used for the purposes of risk stratification and outcomes. Mean follow-up duration was 4.3±3.0 years (range 6 months to 13 years).
12-lead ECG
Standard 12-lead ECG was performed with individuals in the supine position. T-wave inversion of ≥−0.1 mV in two or more contiguous leads was considered significant other than in leads V1, aVR and III. Deep T-wave inversion was defined as a T-wave deflection of ≥−0.2 mV. ST segment shift of ≥−0.1 mV in two or more contiguous leads was considered significant. LVH was identified using the Sokolow-Lyon criterion. Pathological Q-waves were defined as ≥0.04 s in duration or a Q:R ratio of ≥0.25.
Echocardiography
Standard views of the heart were obtained and analysed in accordance with European Society of Cardiology (ESC) guidelines.14 LV ejection fraction was calculated using Simpson's method.15 Indices of diastolic function were assessed in the apical four-chamber view with pulsed-wave Doppler across the mitral valve and tissue Doppler imaging of the septal and lateral mitral valve annulus.16
Exercise stress testing
All patients were exercised to exhaustion using the standard Bruce protocol on an upright treadmill stress test.17 BP measurements and ECG readings were taken at 1 min intervals and analysed specifically for arrhythmias. A systolic BP rise of >25 mm Hg from baseline to peak exercise was considered normal.18
24-Hour ambulatory ECG monitoring
Ambulatory 24-hour ECG monitoring was performed specifically to detect supraventricular and/or ventricular arrhythmias.19 All individuals were encouraged to continue their daily activities during monitoring. Non-sustained ventricular tachycardia (NSVT) was defined as three or more consecutive ventricular beats at a rate of >120 bpm with a duration of <30 s.
Cardiac MRI
CMRI was performed using methods previously described and analysed with semi-automated software.20 All volumes and masses were indexed for age and body surface area. Late gadolinium images were acquired after intravenous gadolinium-diethylenetriamine penta-acetic acid (DTPA) administration.20 The presence or absence of late gadolinium enhancement was recorded as a binary variable.
Genetic testing
Genetic testing for mutations in sarcomeric contractile protein genes was offered to all individuals with a clinical diagnosis of HCM or suspected HCM. Genetic tests were performed by established and reputable clinical genetics laboratories with experience in performing genetic testing for inherited cardiac conditions. Pathogenic mutations were defined according to currently accepted guidelines.21 Overall, 63 black patients (38.7%) and 132 white patients (50.4%) underwent genetic testing.
Risk assessment, events and outcomes
Conventional markers of SCD were used for risk stratification, namely: (1) history of unexplained syncope; (2) family history of SCD in one or more first-degree relatives; (3) LVH of ≥30 mm; (4) NSVT on ambulatory monitoring or exercise testing and (5) an abnormal systolic BP response to exercise.9 The estimated 5-year risk of SCD was calculated using the ESC risk stratification model.13 The primary outcome was a composite of cardiovascular death, cardiac arrest or appropriate device therapy, defined as appropriate anti-tachycardia pacing and/or shock delivery from an implantable cardioverter-defibrillator (ICD). Cardiovascular deaths included all HCM-related cardiovascular deaths (SCD, end-stage heart failure and stroke) and non-HCM-related cardiovascular deaths. Secondary outcomes included myocardial infarction and stroke. Of the 425 individuals, 16 were excluded from subsequent survival analysis due to a primary event prior to study entry. Of the remaining 409 patients, a further 16 had experienced a secondary event prior to study entry and were excluded from subsequent survival analysis for secondary events.
Statistical analysis
The Kolmogorov-Smirnov test was used as a test of normality. Values were expressed as mean±SD or percentages, as appropriate. Comparisons were performed by Student's t-test, Mann-Whitney U test and χ2 test (or Fisher's exact test, where appropriate) for normally distributed, non-normally distributed and categorical variables, respectively. Survival curves were constructed according to the Kaplan-Meier method and comparisons were performed using the log-rank test. HRs and 95% CIs were calculated with Cox proportional hazards regression models. A two-tailed p value of <0.05 was considered significant throughout.
To determine predictors of the primary outcome, clinical variables were tested using univariate analysis. Variables with a p value of <0.1 for univariate associations were entered into a backward stepwise multivariable Cox proportional hazards regression model to determine independent predictors of the primary outcome. All analyses were performed using SPSS software (V.20.0; IBM, Chicago, USA).
Results
Baseline demographics
Baseline demographics, clinical presentation and comorbidities in black versus white patients are presented in table 1. A history of hypertension at study entry was almost twice as common in black compared with white patients. A total of 91 black patients (55.8%) and 79 white patients (30.2%) were on antihypertensive treatment. The majority of patients with hypertension (145 out of 178, 81.5%) had good BP control (<140/90 mm Hg), established over a mean period of 44.1±23.9 months (range 5–120 months). Only 11 patients (2.6%) exhibited persistently elevated BP during follow-up.
Baseline demographic characteristics, mode of presentation and symptoms at initial evaluation in black versus white patients with HCM
Mode of presentation and symptoms
The diagnosis of HCM was triggered predominately by symptoms in both groups (table 1). A fortuitous diagnosis of HCM was more common in black patients (31.3% vs 19.1%, p=0.004). In particular, black patients were more likely to be identified following investigation of an abnormal ECG performed for an unrelated reason (27.0% vs 10.7%, p<0.001). In contrast, white patients were more frequently diagnosed after familial screening (6.7% vs 17.6%, p=0.001). Compared with white patients, more black patients presented with cardiac arrest (3.1% vs 0.0%, p=0.008) or with New York Heart Association class IV symptoms (3.1% vs 0.4%, p=0.008).
ECG changes
A higher proportion of black patients exhibited an abnormal ECG (98.2% vs 90.5%, p=0.002) (table 2). Although common in both ethnicities, repolarisation abnormalities were more prevalent in black patients, particularly T-wave inversion (91.4% vs 73.0%; p<0.001), including lateral T-wave inversion (84.0% vs 68.0%, p<0.001) and deep T-wave inversion (80.2% vs 58.3%, p<0.001). The prevalence of ST-segment depression was also more common in black patients (55.6% vs 45.6%, p=0.046), while pathological Q-waves were more common in white patients (11.1% vs 23.2% p=0.002).
Electrical and structural characteristics of black versus white patients with HCM
Structural changes
There were no ethnic differences in mean left atrial dimension, LV dimensions, maximum LV wall thickness, LV mass or LV systolic function (table 2). Though common in both groups, asymmetric septal hypertrophy was observed in only one-third of black patients compared with over half of white patients. In contrast, both apical and concentric patterns of LVH were more common in black patients. Importantly, almost 10% of black patients (n=16) revealed concentric LVH. Of these, four had a positive gene test, three had a family history of HCM, two exhibited LVH of ≥20 mm and one experienced a cardiac arrest. The remaining five individuals had no history of hypertension or other conditions capable of producing the same magnitude of LVH. Of the patients subjected to CMRI, the presence of late gadolinium enhancement was more common in white patients (55.8% vs 70.3%, p=0.022).
Diagnosis of HCM in patients with hypertension and concentric LVH
Seven patients (six black and one white) had concentric LVH and a past history of hypertension. The BP was well controlled for at least 12 months in all individuals and for ≥24 months in six individuals. Three patients revealed a pathogenic gene mutation, two revealed severe LVH with a maximum LV wall thickness of 24 and 25 mm respectively and one had a family history of HCM (see online supplementary table S1).
Supplementary table
We performed a separate analysis to examine ethnic differences after excluding all patients in whom the LVH could potentially be attributable to hypertension alone. All patients with concentric LVH and a past history of hypertension (n=7) were excluded as were white patients with a previous history of hypertension and LVH of <16 mm (n=10) and all black patients with a previous history of hypertension and LVH <20 mm (n=49), irrespective of the pattern of hypertrophy. A higher cut-off for LV wall thickness was selected for black patients because it is recognised that black individuals may exhibit a greater magnitude of LVH in response to high LV afterload.2 ,13 The final cohort consisted of 108 black patients and 251 white patients. A comparison of key parameters between these two groups revealed similar findings to the original data (see online supplementary table S2).
Genetic analysis
Of all patients referred for genetic testing, a recognised disease-causing mutation was identified in a similar proportion of black and white patients (54.0% vs 50.8%, respectively, p=0.675). The vast majority of black and white patients had mutations in the myosin-binding protein C gene (54% and 51%, respectively).
Risk factor profile for SCD
Among 409 patients eligible for survival analysis, there were no ethnic differences in the overall risk of SCD based on conventional risk markers or the ESC risk stratification model (table 3).13 Regarding individual risk factors, a history of syncope was more common in black patients whereas an abnormal BP response to exercise was more common in white patients (table 3).
Risk factor profile in black versus white patients with HCM eligible for survival analysis (n=409)
Primary and secondary outcomes
During the study period, a similar proportion of black and white patients experienced primary and secondary outcome events (table 4). Of the 409 patients eligible for survival analysis, 24 (5.9%) died from cardiovascular causes, 7 (1.7%) survived a cardiac arrest and 11 (2.7%) received appropriate ICD therapy. Kaplan-Meier survival analysis demonstrated no differences in estimated freedom from primary outcome in black versus white patients over the follow-up period (p log-rank=0.095, figure 1A). Similarly, Kaplan-Meier survival analysis demonstrated no ethnic differences in estimated freedom from stroke or myocardial infarction over the follow-up period.
Events and comorbidities in black versus white patients with HCM eligible for survival analysis (n=409)
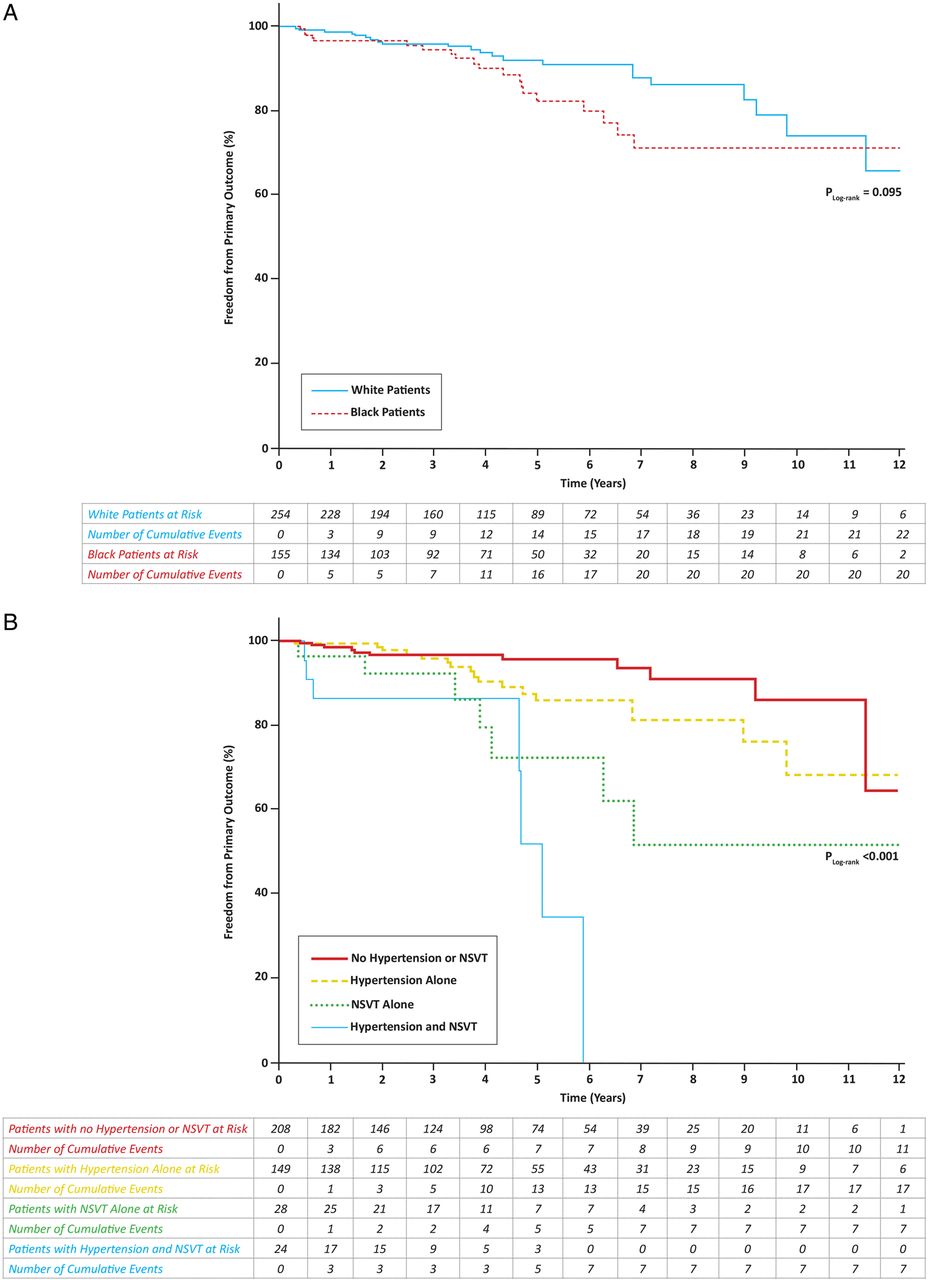
Kaplan-Meier curves illustrating freedom from the primary outcome during the study (A) according to ethnicity and (B) according to the presence or absence of NSVT and/or hypertension, in various combinations, for the overall cohort of black and white patients eligible for survival analysis (n=409). NSVT, non-sustained ventricular tachycardia.
Determinants of the primary outcome
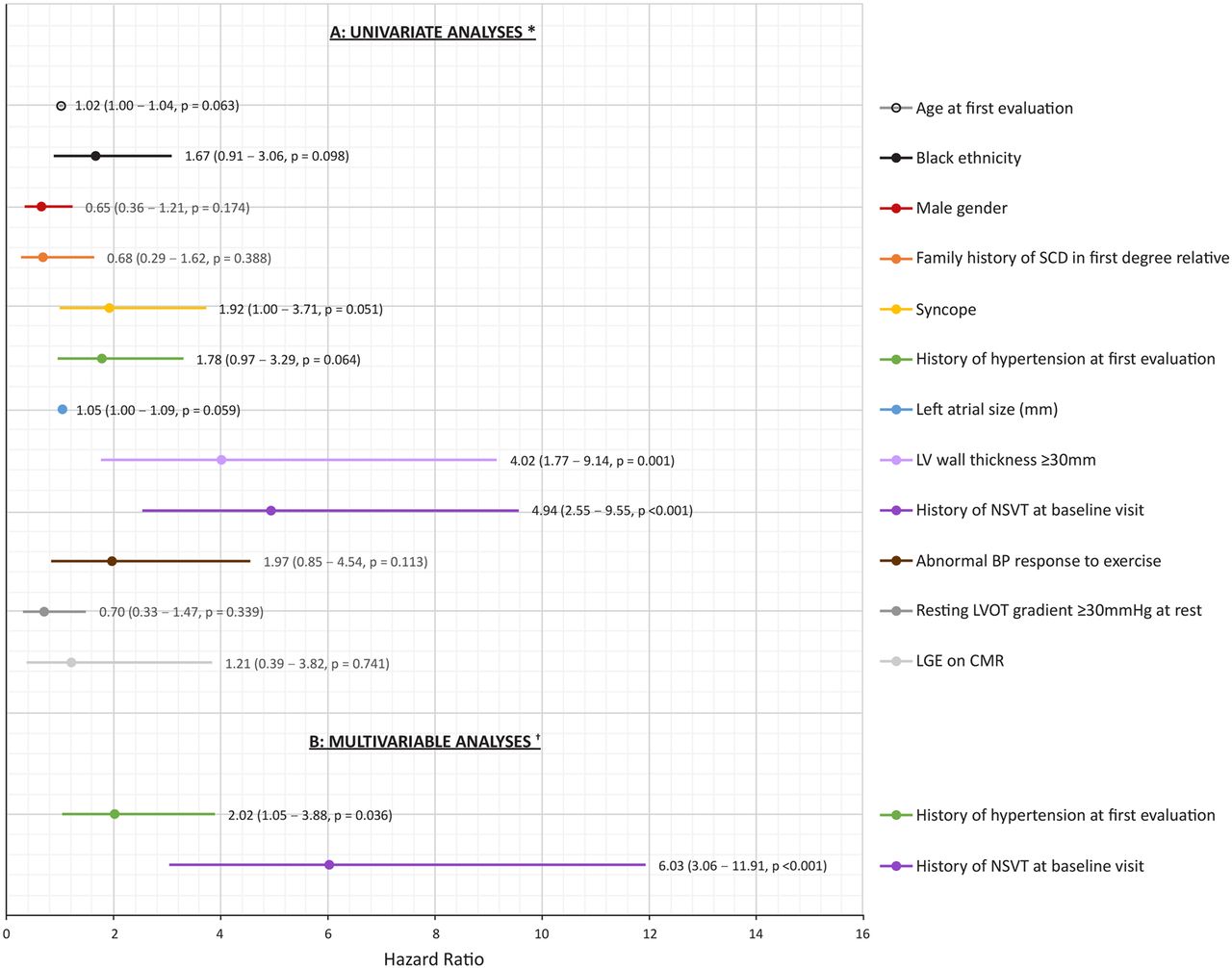
Univariate analysis demonstrated an association between the primary outcome and several cohort characteristics (figure 2A). However, on multivariable analysis (figure 2B), only hypertension (HR 2.02, 95% CI 1.05 to 3.88, p=0.036) and NSVT (HR 6.03, 95% CI 3.06 to 11.91, p≤0.001) remained independent predictors of the primary outcome. Log-rank test analysis demonstrated an additive detrimental effect on freedom from primary outcome among patients with hypertension and NSVT (figure 1B).

{kind=link}
{kind=link}
Forest plot depicting results of univariate (A) and multivariable (B) analyses for predictors of the primary end point (cardiac death, appropriate implantable cardioverter-defibrillator (ICD) therapy or cardiac arrest) in the total cohort of black and white patients with hypertrophic cardiomyopathy eligible for survival analysis (n=409). *The figure depicts statistically significant variables and variables considered to be associated with an increased risk of SCD in hypertrophic cardiomyopathy. †Using backward stepwise (likelihood ratio) method; all variables that demonstrated a p value of <0.1 in the univariate analyses were included in the multivariable model. BP, blood pressure; CMR, cardiac magnetic resonance; LGE, late gadolinium enhancement; LV, left ventricular; LVOT, left ventricular outflow tract; NSVT, Non-sustained ventricular tachycardia; SCD, sudden cardiac death.
Treatment strategies
Myectomies and Disopyramide use were more common in white patients, whereas the use of antihypertensive agents was more common in black patients (table 5).
Treatment strategies in black versus white patients with HCM eligible for survival analysis (n=409)
Influence of hypertension on the HCM phenotype
Based on the high prevalence of co-existent hypertension and its association with the primary outcome, we performed a separate comparison between hypertensive and normotensive patients (see online supplementary table S3). Of interest, patients with HCM and a history of hypertension were on average 15 years older at the time of diagnosis compared with normotensive patients (59.5±13.3 vs 44.7±16.7 years, p<0.001). However, there were no differences between the two groups with respect to the magnitude and pattern of LVH, prevalence of resting LV outflow tract obstruction, the proportion with a disease-causing genetic mutation or conventional risk factors for SCD, with the exception of a family history of SCD which was more common in the normotensive group (22.7% vs 13.5% p=0.017). Hypertensive patients demonstrated inferior indices of diastolic function (as assessed by E/E′) compared with normotensive patients.
Discussion
HCM is a relatively common and treatable condition with a relatively benign course in most patients.1 Despite being recognised as a global disorder, data relating to the phenotypic manifestations and natural history in black patients are scarce.8 ,22 ,23 Additionally, black patients have a high prevalence of hypertension, which is conventionally regarded as an exclusion criterion for the diagnosis of HCM; therefore, the diagnosis of HCM is probably under-reported in this cohort. However, black ethnicity modulates a number of cardiovascular diseases, including myocardial infarction,24 stroke25 and heart failure.26 The present study provides a comprehensive description of the clinical phenotype and natural course of HCM in a well-characterised cohort of black and white patients in the UK with equal access to a national healthcare system.
Phenotypic differences between black and white patients
Almost all black patients (n=160, 98.2%) exhibited an abnormal ECG, with a high prevalence of T-wave inversion (n=148, 91.4%), which was frequently deep (n=130, 80.2%) and involved the lateral leads (n=136, 84.0%). In contrast, almost 10% of white patients revealed a normal ECG. One-third of black patients exhibited apical or concentric patterns of hypertrophy compared with only 12% of white patients. Both patterns of hypertrophy may be responsible for failure to diagnose HCM in black individuals, leaving them vulnerable to complications. In the context of hypertension, concentric LVH may be mistaken for hypertensive heart disease, while apical hypertrophy may go undetected on conventional echocardiography and the associated marked repolarisation changes falsely attributed to a ‘left ventricular strain pattern’. The observation that patients with a history of hypertension (mainly black) were diagnosed with HCM, on average, 15 years later than normotensive patients supports this theory.
In this study, the electrical and structural differences between black and white patients with HCM persisted even after excluding individuals who may be considered to have hypertensive heart disease, suggesting that such differences are a genuine reflection of the impact of ethnicity on the HCM phenotype. In this regard, a diagnosis of HCM should be entertained in all black patients with a history of hypertension who exhibit marked LVH and T-wave inversion in the lateral leads despite good BP control.27
Ethnic differences in HCM risk profile
Black patients did not exhibit a higher prevalence of conventional risk markers for SCD or higher 5-year risk.13 In addition, ethnicity was not a determinant of the composite primary outcome of death, cardiac arrest or appropriate ICD therapy. Therefore, our findings do not indicate a more malignant course of HCM in black patients. In contrast, data from a US registry of SCD in young athletes reported a higher number of HCM-related SCDs in black athletes.8 Although an increased predisposition to fatal arrhythmias during strenuous exercise on the HCM phenotype in black athletes cannot be excluded, the registry findings are likely to reflect relatively higher participation rates, lower accessibility to healthcare or underdiagnosis of HCM in black athletes during pre-participation evaluation.2 ,3
The influence of hypertension on outcome in HCM
The prevalence of hypertension in our cohort was similar to that reported in the general black and white population28 and some HCM cohorts,29 although higher than that reported in other studies of patients with HCM.30 Multivariable analysis identified NSVT and hypertension as independent predictors of the primary outcome, irrespective of ethnicity, gender or age (figure 2B). NSVT conferred a sixfold increased risk of reaching the primary outcome during the study period. Hypertension was present in 40% of the overall cohort and was more prevalent in black patients. Although hypertension had limited influence on the phenotypic expression of HCM (see online supplementary table S3), it was associated with a twofold increased risk of reaching the primary outcome during the study period. The combination of NSVT and hypertension had a significant additive impact, further reducing event-free survival (figure 1B). These findings are unsurprising given that hypertension adversely affects several disease processes and that NSVT is a well-established risk marker for SCD in HCM. However, the observations nevertheless have important implications for the HCM population given the considerable overlap between hypertension and HCM in clinical practice, underscoring the need for good BP control in patients with HCM.
Study limitations
The authors acknowledge that this study was conducted in tertiary centres and therefore the cohort may have suffered from referral bias and excluded stable, low-risk patients. This may account for the higher adverse events compared with the published literature. Although healthcare is free for all UK citizens, disparities have been reported in access for ethnic minorities31 and may have resulted in fewer black individuals with HCM being referred for evaluation or a greater number being subject to delayed referral. However, the similarity in age at diagnosis and age at first evaluation between black and white patients suggest that these possibilities are less likely (table 1). Patients with a history of hypertension were diagnosed more than a decade later than normotensive patients and the higher prevalence of hypertension in the black cohort may have resulted in more black patients with HCM arriving later in the healthcare system with established disease.
It is possible that a small proportion of black patients with genuine hypertensive heart disease were misclassified as having HCM. However, there were striking similarities in the electrical and structural manifestations of HCM between the hypertensive and normotensive black patients. Furthermore, the lack of any reversal of ECG repolarisation changes and regression of LVH despite good BP control in the great majority of subjects make this inference less likely.27 The additive effect of hypertension on mortality in patients with HCM was probably underestimated by this study, as the majority of hypertensive patients had well-controlled BP. The authors appreciate that the number of patients in this study was relatively small and limits the degree to which the outcomes can be generalised to the entire population of black patients with HCM or to black patients with differing ethnic origins. Finally, the natural history of HCM reported in this study applies only to black patients referred for investigation and treatment.
Conclusion
Ethnicity is an important determinant of the phenotypic expression of HCM. Apical and concentric LVH are more common in black patients and, coupled with a higher incidence of hypertension, may potentially contribute to a lower detection rate of HCM in the black population. T-wave inversion is almost universal in black patients with HCM, suggesting the need for comprehensive investigation and follow-up of black individuals exhibiting marked repolarisation anomalies (T-wave inversion), regardless of co-existing hypertension. These findings are not dissimilar to those observed in a smaller cohort of black American patients with HCM.23 Our results indicate that HCM in black patients is associated with a similar prognosis as white patients. However, a history of hypertension has an adverse impact on mortality, regardless of ethnicity.
Key messages
What is already known on this subject?
There are limited data on the clinical phenotype and outcomes in black patients with hypertrophic cardiomyopathy (HCM). The high prevalence of ECG repolarisation changes and left ventricular hypertrophy (LVH) in black individuals may result in diagnostic challenges between HCM and other causes of LVH.
What might this study add?
One-third of black patients with HCM exhibit apical or concentric LVH and almost all have T-wave inversion. The high prevalence of co-existing hypertension may result in HCM being mistaken for hypertensive heart disease in black individuals, leaving them vulnerable to complications of the disease. HCM in black patients is not associated with higher risk or poorer outcomes. However, a history of hypertension is associated with a twofold increased risk of adverse events, irrespective of ethnicity.
How might this impact on clinical practice?
The diagnosis of HCM should be considered in any black hypertensive individual with LVH on imaging studies who exhibits marked ECG repolarisation anomalies. Given the high risk of adverse outcomes associated with hypertension, maintaining good blood pressure control should be an important aspect of the management of all patients with HCM.
Acknowledgments
The authors would like to thank Sue Brown, Teofila Bueser, Kate Dougal and Nina Edwards for their invaluable help with data collection.
References
Footnotes
Twitter Follow Nabeel Sheikh at @nabeelsheikh99, Michael Papadakis at @MichaelPapadak2, Paolo Adami at @paolo_emilio, Mathew Wilson at @Prof_MatWilson and Sanjay Sharma at @SSharmacardio
Contributors NS, MP and SS: study design, data collection and interpretation, quality control, statistical analysis, manuscript preparation and manuscript revision; VFP: data interpretation, quality control, statistical analysis, manuscript preparation and manuscript revision; KP, LM, PA, AZ, SG, MW, GC-W and ERB: data collection and interpretation, quality control and manuscript preparation; MTET: study design, data interpretation, quality control, statistical analysis, manuscript preparation and manuscript revision.
Funding NS, MP, KP, LM, AZ and SG were funded by research grants from the charitable organisation Cardiac Risk in the Young. NS, ERB and SS have also received research grants from the British Heart Foundation.
Competing interests None declared.
Ethics approval Ethical approval was granted by the local research ethics committee in accordance with the Declaration of Helsinki and patients provided oral consent for their anonymised data to be used for this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All additional unpublished information is kept on a secure server in the institution and only available to the first, second and senior authors of the manuscript.