Article Text

Abstract
Background: There is evidence that ultra-endurance exercise causes myocardial injury. The extent and duration of these changes remains unresolved. Recent reports have speculated that structural adaptations to exercise, particularly of the right ventricle, may predispose to tachyarrhythmias and sudden cardiac death.
Objective: To quantify the extent and duration of post-exercise cardiac injury with particular attention to right ventricular (RV) dysfunction.
Methods: 27 athletes (20 male, 7 female) were tested 1 week before, immediately after and 1 week after an ultra-endurance triathlon. Tests included cardiac troponin I (cTnI), B-type natriuretic peptide (BNP) and comprehensive echocardiographic assessment.
Results: 26 athletes completed the race and testing procedures. Post-race, cTnI was raised in 15 athletes (58%) and the mean value for the entire cohort increased (0.17 vs 0.49 μg/l, p<0.01). BNP rose in every athlete and the mean increased significantly (12.2 vs 42.5 ng/l, p<0.001). Left ventricular ejection fraction (LVEF) was unchanged (60.4% vs 57.5%, p = 0.09), but integrated systolic strain decreased (16.9% vs 15.1%, p<0.01). New regional wall motion abnormalities developed in seven athletes (27%) and LVEF was reduced in this subgroup (57.8% vs 45.9%, p<0.001). RV function was reduced in the entire cohort with decreases in fractional area change (0.47 vs 0.39, p<0.01) and tricuspid annular plane systolic excursion (21.8 vs 19.1 mm, p<0.01). At follow-up, all variables returned to baseline except in one athlete where RV dysfunction persisted.
Conclusion: Myocardial damage occurs during intense ultra-endurance exercise and, in particular, there is a significant reduction in RV function. Almost all abnormalities resolve within 1 week.
Statistics from Altmetric.com
There is concern that ultra-endurance exercise results in myocardial damage. Assessments completed soon after completion of endurance races of various sporting disciplines have reported biochemical and functional cardiac abnormalities. Increases in cardiac troponin I (cTnI) and B-type natriuretic peptide (BNP) as well as left ventricular wall motion abnormalities on echocardiography have been described.1–3 The reports have been inconsistent, however, with some studies reporting only very mild or no evidence of cardiac dysfunction.4–6 Few studies have combined both biochemical and functional assessments. Moreover, the consequence of acute dysfunction is currently unknown as there are no previous studies that assess the duration of post-exercise changes.
The importance of comprehensively assessing post-exercise changes in myocardial function is critical given the increasing speculation that ultra-endurance exercise may be associated with a predisposition to ventricular tachycardia and sudden cardiac death. Although there is a lack of longitudinal epidemiological data to support this premise, a number of case reports and cohort descriptions have raised concern.7–10 The largest series of endurance athletes presenting with ventricular tachycardia observed that a majority of athletes had right ventricular (RV) abnormalities which served as an arrhythmogenic focus.11 The most common abnormalities were enlargement and reduced contractility of the right ventricle. In the immediate post-exercise setting there is a paucity of data as to whether RV function is impaired. This assessment is of critical importance given the logical hypothesis that repeated RV insults may result in chronic RV dysfunction, providing a substrate for arrhythmogenesis.
In this study, the aim was to describe comprehensively the extent and duration of myocardial injury after an ultra-endurance triathlon race. To achieve this, established biochemical measures of myocyte damage and cardiac function (cTnI and BNP) as well as comprehensive echocardiographic assessments were used with an emphasis on measures of RV function. To define the temporal profile of any identified abnormalities, measurements were repeated at 7 days post-race.
METHODS
Study population and exercise stimulus
Twenty-seven (20 male, 7 female) of the 1574 athletes competing in the 2004 Australian Ironman ultra-endurance triathlon volunteered to participate in the study. A spectrum of age and experience was selected ranging from professional to relative novice (table 1). Written informed consent for participation was obtained, and the St Vincent’s Hospital Human Research and Ethics Committee approved the protocol.
The event involved a 3.8 km swim, 180 km cycle and 42.2 km run staged in a remote coastal town. A dedicated research team equipped a temporary facility at the race finish line for immediate post-race assessments.
Evaluation
Evaluations were performed at three time points—pre within 2 weeks before the event, post immediately after and delayed at 1 week after the event. Biochemical and detailed echocardiographic assessments were performed at each time point along with measurements of height, weight, blood pressure and a 12-lead electrocardiogram.
Serum biochemistry
Venous blood was collected from athletes. BNP was analysed immediately using a rapid fluorescence immunoassay (Biosite Diagnostics, San Diego, USA). The remaining blood samples were centrifuged, refrigerated to 4°C and transported to a central laboratory for analysis. Samples were analysed for cTnI (Abbott AxSYM, Illinois, USA), creatine kinase, creatine kinase MB isoform, urea, creatinine and haemoglobin. The laboratory lower limits for detection of cTnI and BNP were <0.16 μg/l and <5 ng/l, respectively.
Echocardiography
Images were obtained using a Vivid 7 echocardiograph (GE Medical, Horton, Norway) and stored in raw data format. Two observers, unaware of subject identity and study time point, analysed the data using Echo-Pac PC software (GE Medical). Cardiac dimensions were obtained from parasternal M-mode images, while two-dimensional images were obtained from the parasternal long and short-axis views and the apical two- and four-chamber views. Spectral pulsed-wave Doppler recordings were made of mitral inflow, pulmonary venous flow and left ventricular outflow tract profiles. Spectral tissue Doppler recordings were made of the septal and lateral mitral annulus and the tricuspid annulus in the apical four-chamber view. Colour tissue Doppler imaging recordings of the left and right ventricles were also made in the four-chamber view. The average value of three consecutive beats was used for each measure.
LV function
The wall motion score index was scored using a 16-segment model according to the recommendations of the American Society of Echocardiography.12 The presence of wall motion abnormalities (WMAs) was used to define an “abnormal” post-race population in whom other measures of myocardial dysfunction could be compared. WMA analyses were reported by two “blinded” cardiologists with an intra- and interobserver agreement of 97.8% and 96.7%, respectively, for scoring each segment.
The left ventricular ejection fraction (LVEF) was calculated according to a modified Simpson’s method. Mitral inflow parameters were measured from spectral Doppler recordings. Peak early (E) and late (A) mitral inflow velocities, E deceleration times and mitral inflow propagation velocity (Vp) were calculated. Pulsed-wave tissue Doppler of the septal annulus was used for the calculation of early peak diastolic mitral annular velocity (e′). Left ventricular filling pressures were approximated from the relationship E/e′.
New echocardiography techniques
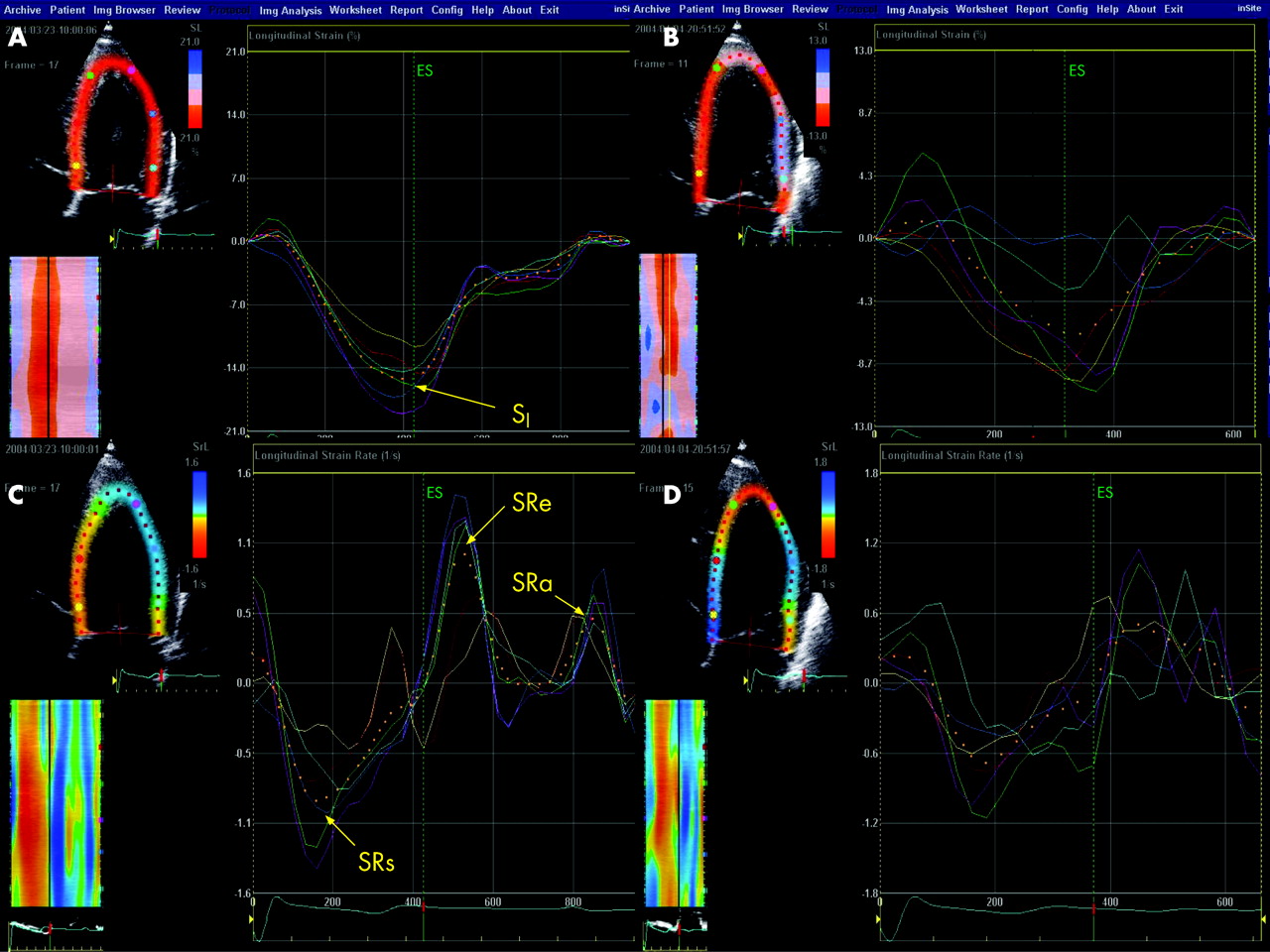
Longitudinal strain and strain rate measurements were obtained from four-chamber grey-scale images. After manually defining the endocardium and region of interest, a pixel tracking method automatically identified a unique cluster of pixels in the myocardium that could then be tracked through the myocardial cycle as previously described.13 Maximal integrated strain (SI) was calculated in a longitudinal plane from the variation in segment length using the tracked end points in each of six left ventricular segments (basal, mid and apical segments of the septal and lateral walls). The average of the six segments was recorded for three consecutive cardiac cycles. Strain rate (SR) was calculated as the temporal derivative of SI. Maximal longitudinal SR was calculated for each segment in systole, early diastole and late diastole (SRs, SRe, SRa). Figure 1 shows a representative example of SI and SR measurements for one athlete.
RV function
Right ventricular fractional area change (RVFAC) was calculated from the apical four-chamber view—the change in RV area between diastole and systole being expressed as a ratio of the diastolic area. Tricuspid annular plane systolic excursion (TAPSE) was obtained from colour tissue Doppler studies using tissue tracking to measure the excursion of the lateral annulus toward the apex during systole. Both techniques have been well validated against radionuclide angiography and MRI.14–16
Tissue Doppler imaging of the free wall tricuspid annulus was used to derive the annular velocity (TV S′); a value of <11.5 cm/s was used to identify athletes with abnormal RV function.17 The tricuspid regurgitant velocity (VTR) was obtained by continuous-wave Doppler from the four-chamber view. The pulmonary artery systolic pressure (PASP) was estimated from the VTR using the modified Bernoulli equation18 including an estimate of right atrial pressure.
Statistical analysis
Continuous variables are expressed as mean (SD) with the exception of age, which is expressed as median and range. Analysis of variance (ANOVA) was used to assess differences between the groups of values. Data with a non-normal distribution were normalised using a logarithmic transformation before ANOVA analysis. Post-ANOVA analysis was performed using Tukey’s honestly significance difference method. Categorical variables were compared using a χ2 test. All reported p values were calculated on the basis of two-sided tests, and a p value <0.05 was considered to indicate significance. Correlations were performed using the Pearson product-moment coefficient of correlation. Analyses were performed using Lumenaut software version 3.0 (Lumenaut Ltd., Hong Kong, China).
RESULTS
Baseline characteristics
Male athletes were heavier, taller and leaner than female athletes. However, the cardiac morphology was similar for both sexes (table 1). ECG voltage criteria for left ventricular hypertrophy19 was present in 9 (33.3%) of the athletes.
Twenty-six of the athletes completed the race in a mean (SD) time of 10 hours 50 minutes (1 hour 15 minutes). No athlete described adverse cardiac symptoms.
Effect of exercise
The ultra-endurance exercise stimulus resulted in a 1.1% reduction in body weight and a 33% increase in serum creatinine. Haemoglobin was not significantly increased. There was a ninefold increase in creatine kinase and a fourfold increase in creatine kinase MB isoform (table 2).
Cardiac troponin I was mildly raised in three athletes at baseline and undetectable in the remainder. After exercise, there was a significant increase in the number of athletes with a detectable cTnI (11.5% vs 57.7%, p<0.001; table 2). The extent of the post-race increase in cTnI was also highly significant (fig 2A). The BNP increased in every athlete (100%), resulting in a significant difference between the pre- and post-race values (fig 2B).

Echocardiography
LV function
Table 3 summarises the echocardiographic assessment of left and right ventricular function. Baseline evaluation demonstrated normal cardiac function with the exception of one athlete who had one hypokinetic wall segment in the presence of otherwise normal measures of systolic function. After exercise, seven athletes (26.9%) had segmental WMAs and the wall motion score index increased significantly. On average, there were 6.3 abnormal segments in each of the seven athletes with WMAs. In each case, the distribution of WMAs did not conform to a coronary artery territory. There was a 10.7% reduction in integrated strain (SI) and a trend toward reduced LVEF (p = 0.09). Conventional diastolic measures were unchanged in the post-race setting.
When the seven athletes with WMAs were considered in isolation, systolic impairment was demonstrated by reductions in LVEF by 20.6%, SI by 29% and SRs by 18.5%. Diastolic impairment was also evident with a post-race reductions in SRe of 32.6%. The measures of E/A ratio, e′ and E/e′ did not change significantly post-race.
RV function
Baseline RV function was normal in all athletes. Exercise resulted in significant impairment of RV function as demonstrated by a significant post-race reduction in RVFAC and TAPSE. The reduction in RVFAC was predominantly due to an increase in post-race RV systolic area (table 3). In athletes with left ventricular WMAs the reductions in RVFAC (38%, p = 0.001) and TAPSE (21%, p = 0.03) were greatest. However, they were also decreased significantly in those athletes without evidence of left ventricular dysfunction (fig 3).

{kind=link}
{kind=link}
{kind=link}
Doppler measures of RV function showed a significant increase in the number of athletes with abnormal RV function (table 3).
There was no significant difference in the estimated PASP in the pre, post and delayed studies.
Delayed measures
Measures of myocardial dysfunction returned to baseline at the delayed analysis performed at 1 week post-race. No significant difference existed between baseline and delayed measures in cTnI, BNP or the left and right ventricular function measures.
Although group comparisons showed complete recovery, one athlete developed chronic RV abnormalities. In this athlete, the left ventricular WMAs resolved (0/16 segments pre, 11/16 post and 0/16 delayed), whereas the acutely dilated and hypokinetic right ventricle failed to improve at 1 week with no increase in RVFAC (0.42 pre, 0.19 post and 0.22 delayed) or TAPSE (18.3, 11.2 and 11.0 mm). Further investigations disclosed no evidence of coronary artery disease on angiography and no serological evidence of acute viral infection. On repeated analyses over the subsequent 12 months, this athlete’s right ventricle remained dilated and hypokinetic.
Correlation between biochemical and morphological measures of cardiac damage
There was a strong correlation between the pre- and post-race differences in cTnI and BNP (r = 0.91, p<0.001). Echocardiographic measures of systolic dysfunction correlated with changes in cTnI and BNP. Wall motion index correlated strongly with both the change in cTnI (r = 0.77, p<0.001) and BNP (r = 0.70, p <0.001). SI and SRs also correlated significantly with the biochemical markers of myocardial injury (table 4).
DISCUSSION
This study demonstrates that myocardial damage occurs after intense and prolonged exercise. The findings of raised cTnI and BNP, and left ventricular WMAs confirm previous findings. For the first time, these abnormalities have been shown to correlate within the same cohort. In addition, this study identifies three important new findings: that myocardial dysfunction is transient, that strain and strain rate are reliable and sensitive measures in this clinical setting and that endurance exercise can induce significant RV dysfunction.
Post-race increases in cTnI were present in more than half of the athletes in our study. This exceeds the prevalence described in previous studies.1 2 The extent of the increase in cTnI is, however, consistent with previous descriptions. Although only mild to moderate, it does suggest that myocardial injury occurs. There is limited experience with BNP in the setting of endurance exercise. Studies using exercise treadmill testing have shown that BNP is raised in subjects with structural or ischaemic heart disease after acute exercise, but not in healthy controls and athletes.20 21 The more prolonged exercise stimulus undertaken in this study resulted in an increase in BNP in all athletes and, in some cases, to levels in excess of those used as a diagnostic cut-off point for left ventricular failure.22 The strong correlation between cTnI and BNP supports the premise that abnormal loading of ventricular myocytes may result in myocardial injury. Importantly, the increases in cTnI and BNP were not correlated with changes in creatinine confirming that they could not be explained by renal dysfunction.
The echocardiographic analyses provided functional confirmation of the cardiac dysfunction suggested by the biochemical abnormalities. Seven athletes had clear evidence of regional WMAs and in each case multiple segments were affected (mean 6.3 abnormal segments per athlete). In this group, the significant reductions in LVEF, SI and SRs provide confirmation of the impairment in systolic function after the race. When all the athletes were considered, a spectrum of cardiac effects was apparent, with many athletes showing a decrement in function while others showed either no change or an improvement in LVEF. The overall trend toward a reduction in LVEF suggests that some athletes may have evidence of LV dysfunction without clear segmental WMAs. This proposition is supported by the significant reduction in SI in the complete post-race cohort. The greater difference seen in SI than in LVEF may reflect the fact that it measures regional changes in myocardial thickening. Also, it is less dependent on ventricular loading conditions that may be expected to vary in the post-exercise setting. The diastolic measures (SRe and SRa) were significantly reduced in the seven athletes with WMAs, whereas there was no change in E/A ratios, Vp or E/e′. Again, this difference may reflect their relative independence of ventricular loading conditions.
The most profound abnormalities were those of right ventricular function. RVFAC and TAPSE are two of the best validated14–16 techniques for measuring RV function and were consistent in demonstrating a post-race reduction in RV function in athletes with and without evidence of LV WMAs. The RV diastolic area did not change at each time point, which is evidence that this reduction in RV function cannot be attributed to changes in athletes’ volume status. Rather, the reduction in RV systolic area shows a true reduction in RV function, suggesting either a reduction in contractility or an increase in after load. Though a less well-validated measure, tricuspid annular systolic velocity (TV S′) identified seven athletes in whom the reduction in RV function was sufficiently profound to be classified as abnormal.
The cause of this RV dysfunction remains speculative. It is feasible, however, that the RV is less capable than the LV at compensating for the sustained massive cardiac output demanded of prolonged physical efforts. Second, PASP has been shown to increase during exercise in athletes,23 hence increasing after-load demands on the right ventricle. In our study PASP did not increase post-race. Possibly, however, increases in PASP during exercise resolved before measurement soon after the event while the RV impairment did not.
This echocardiographic evidence of cardiac dysfunction provides functional validation of the biochemical abnormalities, and the measures are strongly correlated. In addition to the established relationship between LV injury and increases in cTnI and BNP, increases can also result from isolated right ventricular strain.24 Thus, the echocardiographic and biochemical results are complementary and consistent. They provide a clear advance in the understanding of the acute changes after ultra-endurance exercise.
More important than the description of the myocardial dysfunction is an understanding of the prognosis and implications of the changes. Like many physiological models, particularly in relation to exercise, it is quite possible that the acute myocardial damage is followed by repair as a result of myocyte hyperplasia and hypertrophy. The baseline characteristics of the athletes’ hearts are consistent with previous descriptions of endurance-trained athletes. That is, they are dilated and hypertrophied. Possibly, this reflects a physiological adaptation resulting from recurring episodes of cardiac damage and subsequent “supercompensation”—a process analogous to the well-documented response to training in skeletal muscle.25 To this extent it is very significant and reassuring that all measurable changes resolved by 1 week after the event. There is, however, a potential for generation of scar tissue that may have serious long-term sequelae, including a predisposition to ventricular arrhythmias.26 27 There is histological evidence of reactive scar tissue formation after intense exercise in animal models.28 29 Histological evidence in humans is scarce, although at least one case report describes multiple unexplained foci of fibrosis in an elite marathon runner at necropsy after sudden cardiac death.30
The possibility of incomplete or pathological remodelling after recurrent intense exercise bouts was raised in a large case series of elite athletes presenting with ventricular tachycardia. Heidbuchel et al reported a high incidence of RV abnormalities in these athletes and proposed that this may represent a new entity—“exercise-induced RV dysplasia”.11 The prognosis in this group was poor with an incidence of sudden cardiac death of nearly 25%. These findings highlight the significance of our current study where the most profound acute cardiac dysfunction was seen in the right ventricle. One may speculate that repeated RV insults may predispose to the chronic RV pathology identified by Heidbuchel et al. Supporting this is the finding that one athlete developed chronic RV dysfunction which failed to improve in the 12 months after the race. Although these hypotheses are clearly speculative, they highlight the need for improved understanding of the pathophysiological process and chronic consequences of post-exercise myocardial damage.
In conclusion, our study demonstrates that myocardial damage occurs after ultra-endurance exercise and that the resulting myocardial dysfunction most commonly affects RV function. Although these changes have been shown to resolve within 1 week, there remains the possibility that the process of repair may result in chronic subclinical myocardial fibrosis with a risk of resultant complications.
Acknowledgments
Rhonda Sanders, Joanne Wishart and Dr Joe Ferris provided invaluable logistical assistance in data collection.
REFERENCES
Footnotes
Competing interests: None.
Funding: This project was primarily funded by the St Vincent’s Hospital Research and Grants Unit (protocol No HREC 004/04). KAC is funded by a National Heart Foundation Australia postgraduate research scholarship. GE Australia assisted in providing transport costs for the echocardiographic equipment.
Ethics approval: Approved by the St Vincent’s Hospital Human Research and Ethics Committee.