Promoting physical activity to patients
BMJ 2019; 366 doi: https://doi.org/10.1136/bmj.l5230 (Published 17 September 2019) Cite this as: BMJ 2019;366:l5230
- Christine Haseler, general practitioner1,
- Ranulf Crooke, general practitioner2,
- Tobias Haseler, general practitioner specialty trainee3
- 1Hucclecote Surgery, Gloucester, UK
- 2Hilary Cottage Surgery, Fairford, UK
- 3The Bloomsbury Surgery, London, UK
- Correspondence to C Haseler christine.haseler{at}nhs.net
What you need to know
Benefits to health start at just 30 minutes of physical activity a week, but more than a quarter of UK adults fail to achieve this
Physical activity can reduce all cause mortality more effectively than medication
Risk of harm from moderate physical activity is small, while the adverse effects of inactivity and sedentary time are clear
The health benefits of physical activity are proved and wide ranging, exceeding that of any drug. The Academy of Medical Royal Colleges has described physical activity as a “miracle cure.”1 Meanwhile, inactivity contributes to as many deaths in the UK as smoking2 and is the fourth leading risk factor for mortality worldwide.3 More than 25% of adults in the UK are inactive, doing less than 30 minutes of physical activity a week.2 Clinicians are uniquely placed to help their patients to become more physically active, and even a brief discussion within a consultation can lead to change.
This article offers a practical guide to help clinicians discuss physical activity within a consultation, including how to address concerns patients may have about becoming more active and how to help them overcome barriers to change.6
What do we mean by “physical activity”?
Although exercise and physical activity are sometimes used interchangeably, they have distinct meanings. In practice, although exercise may be a more familiar term to people, it can also be off putting to some: you don’t need to be doing exercise to be active.
Physical activity, defined by the World Health Organization, is “any body movement performed by skeletal muscles that expends energy,” whereas exercise is “physical activity with the primary purpose of improving or maintaining physical fitness or performance.7” Moderate intensity physical activity “requires a moderate amount of effort and noticeably accelerates the heart rate,5” leads to faster breathing and feeling warmer,15 and requires 3 to 6 times the metabolic rate of being at rest.57
Health benefits of being physically active
Strong evidence shows that individuals who are more active have lower rates of all cause mortality, cardiovascular disease, metabolic disease, colon and breast cancer, and depression, with additional benefits to bone health from weight bearing and resistance activities (fig 1).178 Any level of increased physical activity is beneficial.9 People doing just 15 minutes of moderate intensity physical activity a day have a three year greater life expectancy than those who are inactive, one large cohort study found.10 A recent systematic review and meta-analysis found that all intensities of physical activity, including light intensity, are associated with a substantially reduced risk of death in a dose-response manner (fig 2).9

The health benefits of walking and achievement of recommended levels of physical activity, adapted from Public Health England ‘10 minutes brisk walking each day in mid-life for health benefits and towards achieving physical activity recommendations’4 and UK Department of Health ‘Start Active Stay active’5
{kind=link}

Dose-response associations between total physical activity (top left), light intensity physical activity (LPA) (top right), low LPA (middle left), high LPA (middle right), moderate-to-vigorous intensity physical activity (MVPA) (bottom left), and sedentary time (bottom right).9 cpm=counts per minute
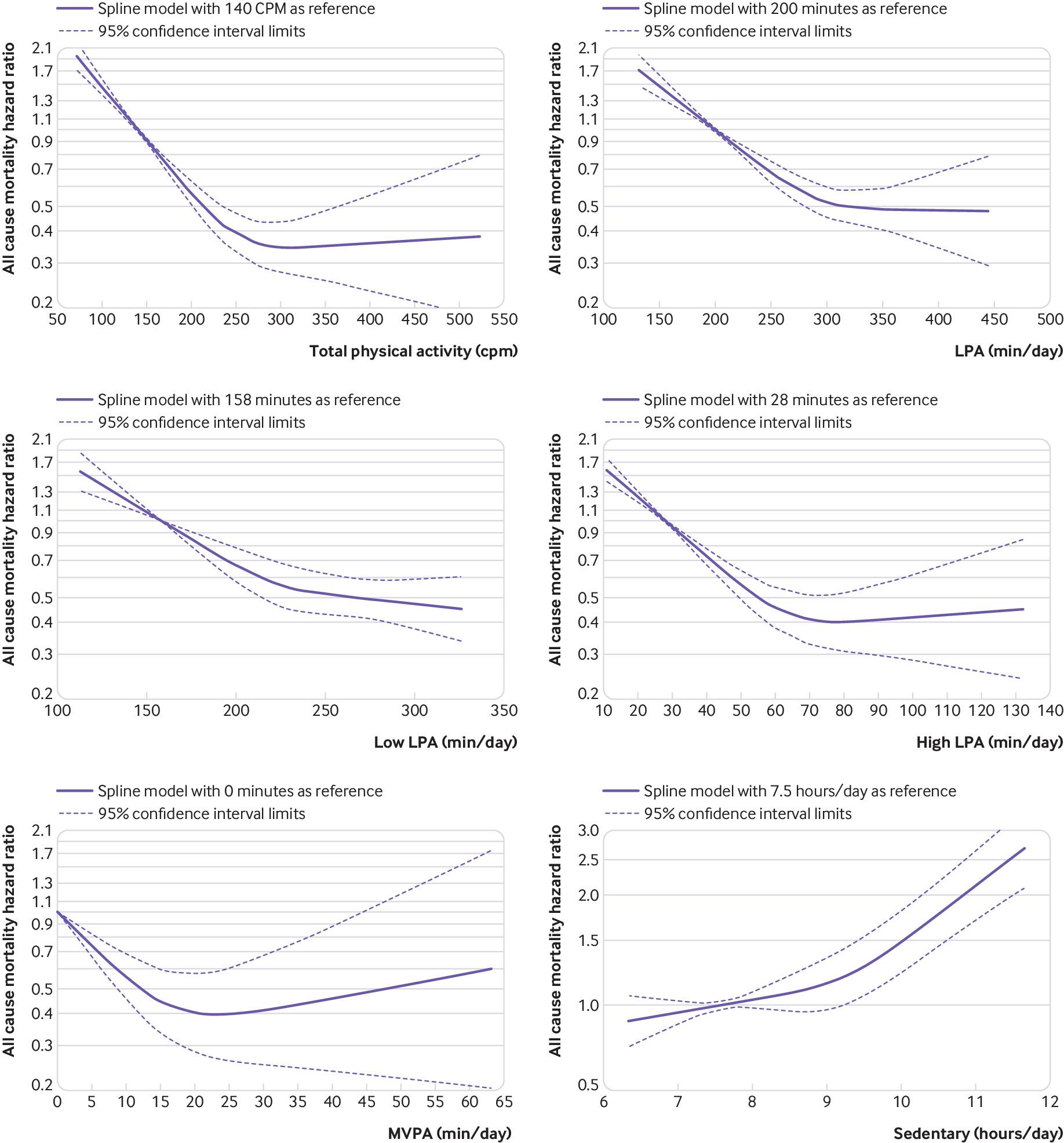{kind=link}
Guidelines from the UK and World Health Organization recommend that adults undertake 150 minutes of moderate intensity physical activity per week in bouts of at least 10 minutes duration, with muscle strengthening activities on at least two days. In the UK 33% of men and 45% of women do not achieve this level of physical activity.2 There is evidence of further benefit from spreading this across the week, with 30 minutes of physical activity on at least five days.7 Even in sufficiently active individuals, daily sedentary time is an independent risk factor for all cause mortality, cardiovascular disease, and diabetes.11
Examples of moderate intensity physical activity157
Brisk walking or cycling
Household chores such as cleaning or gardening, stair climbing, home improvement works
Manual work
Games and sports such as dancing, swimming, or team sports; individual sports such as tennis, martial arts, skateboarding
Jogging, running
Exercise machine run/row/cycle at home or in the gym
Outdoor activities
Charity or event participation that requires keeping to a training schedule
Sexual activity.
Examples of moderate intensity physical activity for people with low exercise capacity, such as frail individuals57
Same relative intensity but lower absolute intensity:
Sitting exercises
Community activity groups, such as strength and balance classes, Tai Chi, and dance classes
Walking, cycling, or moving at normal or lower than normal pace.
How does physical activity improve health?
Regular physical activity produces beneficial changes in body composition such as reduced visceral adiposity. It improves metabolic dysfunction and has anti-inflammatory effects that result in reduced measures of systemic inflammation.1213 These changes are protective in chronic conditions, as visceral adiposity is linked to impaired glucose and lipid metabolism, and low grade systemic inflammation is associated with metabolic syndrome, cognitive dysfunction, and depression.13
Beneficial adaptations from regular physical activity are found in the sympathetic nervous system and the hypothalamic-pituitary axis, leading to increased resilience to physical and psychological stress. Chronic conditions where dysregulation of these systems is observed, such as autoimmune, metabolic, and cardiovascular diseases, and stress related health problems, such as depression, are reduced.13 Increased neuroplasticity and growth factor expression in the brain may further improve both mood and cognition.13
Discussing physical activity in the consultation
When to ask about activity
Any contact with a patient is an opportunity for a discussion about physical activity, and even a brief discussion can help someone to become more active. In one randomised controlled trial of 255 patients, a 3-5 minute discussion in a routine health appointment, with a brief booster call after two weeks, increased physical activity levels 4-6 weeks later by 37 minutes per week, 30 minutes more than controls.14 Opportunities for discussion can be found in new patient appointments, NHS health checks, or chronic disease reviews, and can be prompted by waiting room questionnaires, promotional posters, and videos.15
Screening for inactivity
One approach to discussing physical activity in a consultation is to use “ask-assess-advise,” outlined in figure 3. This is a simple framework for discussing activity adapted from National Institute for Health and Care Excellence (NICE) guidance and NHS Health Scotland’s physical activity screening and brief intervention scripts.1315 “Ask-assess-advise” begins with a validated single question: In the past week, on how many days have you done a total of 30 minutes or more of physical activity, which was enough to raise your breathing rate? This may include sport, exercise, and brisk walking or cycling for recreation or to get to and from places, but should not include housework or physical activity that may be part of your job.1617 The question is followed by an assessment of the patient’s ideas about becoming more active, followed by goal setting and making a plan.

The ‘Ask-Assess-Advise’ structure for discussing physical activity behaviour change in the consultation. Adapted with permission from NHS Health Scotland’s Physical activity screening and brief intervention script and NICE guidance: Physical activity; brief advice for adults in primary care (PH44)1315
{kind=link}
Becoming more physically active
Inactivity may be due to several factors, such as lack of awareness, uncertainty about the benefits of physical activity, difficulty in self motivation, or other personal barriers (box 1).18192021 Encouraging people who are inactive to simply move more is a good start,27 and for many people, incorporating walking or cycling into day-to-day life can be the easiest change to make.57 There is benefit from limiting sedentary time to 20 minutes.11 Those who are sufficiently active but have long periods of sedentary time may be encouraged to take regular breaks from sitting. Motivational interviewing techniques can be particularly useful in helping people to identify and overcome barriers.22 See examples of activities listed above for patients to consider.
Common barriers to increasing physical activity18192021
Lack of motivation
Lack of leisure time
Lack of money
Lack of transport
Illness or disability
Perceived lack of benefit
Lack of provision of open spaces in environment
Lack of safe places to exercise
Lack of physical activity culture in ethnic group
Fear of racial or religious discrimination
Get to know what local physical activity promotion services are available to direct or refer people. Services that offer advice and counselling to promote physical activity can be more effective than those for smoking cessation.23 Remote or web based interventions can be as effective as face-to-face discussions.24
Social prescribing initiatives are another way to help support people who want to get active. These can increase use of local services and encourage increased physical activity levels.25 Activities that include a supportive network or a “social contract,” such as a club or local parkrun, can help, as can smartphone apps or a pedometer.15
Risks of physical activity
Physical activity is safe and beneficial for almost everyone.526 A safeguard against doing too much physical activity too soon is to “start slow and build up,” beginning with approximately 10 minutes’ activity and gradually building up by about 10% per day. Physical activity recommendations are valid for people with disabilities and chronic conditions, taking into account the individual’s capacity or limitations.7
An exercise prescription, a specific set of exercises aimed to improve fitness, is distinct from physical activity advice and has defined contraindications. These include increased cardiovascular demand in unstable angina, severe aortic stenosis, or uncontrolled severe hypertension.27 In pregnancy, impact activities causing trauma, prolonged supine lying, high altitude, or underwater activities are not advised.28 Activity moderation and psychological support are required for exercise addiction, characterised by obligatory and excessive exercise.29
Physical activity in people with long term conditions
Availability of exercise interventions for people with long term conditions vary locally. For those interested in thinking more about how to get more active, resources such as Moving Medicine (see resources box) provide condition specific, evidence based advice.
Osteoarthritis
Physical activity is a core treatment for osteoarthritis.30 Osteoarthritis has been unhelpfully referred to as “wear and tear,” with descriptions such as “bone on bone,” leading to people fearing that physical activity will make it worse. It can instead be described as a “flare and repair” process. The pain from osteoarthritis is multifactorial,31 mainly from synovial inflammation trying to repair a joint, but also from capsule, muscle, ligament stiffness, and bony pain.
Explain that physical activity improves muscle control and tone, which support the joint while it heals. Physical activity also improves range of movement and stiffness, improving function and optimising recovery.
Chronic obstructive pulmonary disease and cardiovascular disease
People with chronic obstructive pulmonary disease or cardiac disease who increase physical activity by completing structured rehabilitation programmes have reduced hospital admissions, greater quality of life, and increased exercise capacity. The benefits in severe disease are just as pronounced as in mild to moderate disease.3233
Advising patients that exercise can be as effective as medication in some chronic diseases can be powerful: a 2013 meta-analysis found that exercise interventions (which were variable between all the studies, including structured rehabilitation and home or community exercise programmes) are often similar to medications in terms of their mortality benefits in the secondary prevention of coronary heart disease, rehabilitation after stroke, treatment of heart failure, and prevention of diabetes.34
Frailty
In older people, decline in muscle power and speed, cardiorespiratory function, and standing balance contribute to frailty. Objective measures of strength and balance, such as grip strength, chair rise, and standing balance, are predictors of all-cause mortality.35 Conversely, preserved muscle strength is associated with reduced cardiovascular mortality, fewer hospital admissions, improved mental health, and a lower risk of falls and fall related injuries.836 There is evidence that improving fitness (strength, stamina, suppleness, and skill) improves cognitive ability and reduces the risk of dementia.36
Resources for patients
Active 10 app—monitors activity, flags 10 minutes done, and weekly achievement. https://www.nhs.uk/oneyou/active10/home
Couch to 5k app or podcast—structured sessions, increasing walking and running to 5k over 9 weeks. https://www.nhs.uk/live-well/exercise/couch-to-5k-week-by-week/
Parkrun—weekly 5k run or walk for all abilities. http://www.parkrun.org.uk
• NHS choices. Exercise: information and physical activity suggestions. https://www.nhs.uk/live-well/exercise
Activity alliance supporting disabled people get more active. http://www.activityalliance.org.uk/
Be inspirational—encouraging joining in with sports. http://www.beinspireduk.org/
Walking for health—free local health walks. https://www.walkingforhealth.org.uk/
Macmillan Cancer Support—guide on keeping active. https://www.macmillan.org.uk/information-and-support/coping/maintaining-a-healthy-lifestyle/keeping-active
British Heart Foundation—guide on staying active with heart disease. https://www.bhf.org.uk/informationsupport/support/healthy-living/staying-active
Age UK—exercise and physical activity advice with links to local classes. https://www.ageuk.org.uk/services/in-your-area/exercise/
Asthma UK—advice on physical activity with asthma. https://www.asthma.org.uk/advice/living-with-asthma/exercise-and-activities/
Professional resources
Moving Medicine—provides a range of evidence based, condition specific information to help professionals advise patients on physical activity. http://movingmedicine.ac.uk/prescribing-movement/
RCGP physical activity and lifestyle webpages—a selection of e-learning and information for GPs, and resources for patients and practice waiting rooms. https://www.rcgp.org.uk/clinical-and-research/resources/a-to-z-clinical-resources/physical-activity-and-lifestyle.aspx
Prescription for Exercise—An NHS web resource for condition specific exercise advice. http://prescription4exercise.com/health-professional/
BMJ learning on physical activity in long term conditions. https://learning.bmj.com/learning/course-intro/physical-activity.html?courseId=10051913
BMJ learning on motivational interviewing in brief consultations. https://learning.bmj.com/learning/module-intro/motivational-interviewing.html?moduleId=10051582
RCGP parkrun practice pages—links to find out more about how GP practices can become a parkrun practice. https://www.rcgp.org.uk/clinical-and-research/our-programmes/clinical-priorities/parkrun-practice.aspx
Education into practice
How do you describe to your patients what constitutes physical exercise?
How do you explain the benefits of physical activity to your patients?
What one thing can your practice do that will lead to increased physical activity in your patients?
How might you develop a system to follow up on activity advice within resource constraints? Consider what systems within your workplace might allow telephone or face-to-face reviews, or how you might use available technologies such as SMS.
How patients were involved in the creation of this article
We contacted patients through social media, our patient participation groups, and surveys handed out in our practices. Their responses and ideas have been incorporated throughout the article. The sections on benefits of physical activity and discussing physical activity in the consultation were developed reflecting patients’ enthusiasm for information and guidance on how to become more active.
Footnotes
Competing interestsThe BMJ has judged that there are no disqualifying financial ties to commercial companies. The authors declare the following other interests: none.
Further details of The BMJ policy on financial interests are here: https://www.bmj.com/about-bmj/resources-authors/forms-policies-and-checklists/declaration-competing-interests.
Provenance and peer review: commissioned; externally peer reviewed.