Fortnightly review: Plantar fasciitis
BMJ 1997; 315 doi: https://doi.org/10.1136/bmj.315.7101.172 (Published 19 July 1997) Cite this as: BMJ 1997;315:172
- Dishan Singh, senior lecturera,
- John Angel, consultanta,
- George Bentley, professorb,
- Saul G Trevino, associate professorc
- a Foot and Ankle Unit, Royal National Orthopaedic Hospital, Stanmore, Middlesex HA7 4LP
- b Institute of Orthopaedics, Royal National Orthopaedic Hospital
- c Baylor College of Medicine, Houston, TX 77030, USA
- Correspondence to: Mr Singh
Introduction
Plantar fasciitis is the most common cause of inferior heel pain (fig 1). Its aetiology is poorly understood by many, which has led to a confusion in terminology.1 It is said to affect patients between the ages of 8 and 80, but is most common in middle aged women and younger, predominantly male, runners.2

{kind=link}
The role of the doctor in the management of plantar fasciitis is to make an appropriate diagnosis and to allow enough time for the condition to run its course, with the aid of supportive measures. If treatment is begun soon after the onset of symptoms, most patients can be cured within six weeks.3
Methods
This article is based largely on our experience and recent concepts that have changed our management of inferior heel pain. Reviews written by experts have been supplemented by selected original articles cited in Medline between 1976 and 1995 and published in high quality journals. We used the following keywords for the Medline search: plantar fasciitis, inferior heel pain, heel spur, calcaneodynia.
Aetiology
The plantar fascia is a strong band of white glistening fibres which has an important function in maintaining the medial longitudinal arch: spontaneous rupture or surgical division of the plantar fascia will lead to a flat foot.4 5 The plantar fascia arises predominantly from the medial calcaneal tuberosity on the undersurface of the calcaneus, and its main structure fans out to be inserted through several slips into the plantar plates of the metatarso-phalangeal joints, the bases of the proximal phalanges of the toes and the flexor tendon sheaths.
Just after heel strike during the first half of the stance phase of the gait cycle, the tibia turns inward and the foot pronates to allow flattening of the foot. This stretches the plantar fascia. The flattening of the arch allows the foot to accommodate to irregularities in the walking surface and also to absorb shock.
Summary points
Plantar fasciitis is the commonest cause of inferior heel pain, but other diagnoses must be excluded
The patient classically presents with symptoms that are worst when taking the first steps after getting out of bed or prolonged sitting
Patients should be advised to wear shoes that have arch supports and soft heels
Treatment with Achilles tendon stretching exercises, oral anti-inflammatory drugs, shoe inserts, and night splints should be started early
The condition is usually self limiting
If there is a predisposing or aggravating factor (box), the repetitive traction placed on the plantar fascia during walking or running may lead to microtears (fig 2), which induce a reparative inflammatory response.6 Biopsy specimens of the inflamed fascia show fibroblastic proliferation and chronic granulomatous tissue.1 6 A normal plantar fascia has a dorsoplantar thickness of 3 mm; in plantar fasciitis this can be 15 mm.7
Risk factors in plantar fasciitis
Sudden gain in body weight, or obesity
Unaccustomed walking or running
Shoes with poor cushioning
Increase in running distance or intensity
Change in the walking or running surface
Tightness of Achilles tendon
Occupation involving prolonged weight bearing

Microtears lead to chronic inflammatory response and thickening of plantar fascia
{kind=link}
Tightness of the Achilles tendon will predispose to plantar fasciitis because limited dorsiflexion of the foot strains the plantar fascia.8 9 10 11 Furthermore, in plantar fasciitis the foot tends to remain in an equinus position during the night and the fascial tissues contract. In the morning, putting weight on the foot puts the plantar fascia under tension, aggravating the pain. This cycle of heel cord tightness and plantar fasciitis should be interrupted as soon as possible by exercises to stretch the heel cord and by using night splints.
The skin and fat in the heel are specialised for friction and shock absorbency.12 The skin is thicker on the sole of the foot than anywhere else; a honeycombed pattern of fibroelastic septae anchored to one another, the calcaneus, and the skin encloses the subcutaneous fat globules. This structure cushions heel strike and allows the skin to resist forces up to twice body weight during long distance running. The thickness of adipose tissue decreases after the age of 40, with loss of shock absorbency. A small percentage of the population has an adventitious subcalcaneal bursa, which may become inflamed and cause heel pain.13
In some cases the plantar tubercle extends forward enough to be called a spur.14 In the general population, 15-25% of people have spurs, and this proportion increases with age and obesity.2 3 15 The greater pull of the plantar fascia was thought to lead to periosteal haemorrhage and inflammatory reaction, and to laying down of new bone and heel spur formation,14 but the heel spur is more often associated with the flexor digitorum brevis muscle than the plantar fascia.2 13 Though the term “heel spur syndrome” seems unjustified, the role of the heel spur in plantar fasciitis is controversial. Half of patients with plantar fasciitis have heel spurs1; the inflamed, thickened fascia may be more painful if it abuts against a heel spur.
Heel pain was recently reported to involve the nerve to abductor digiti quinti, the first branch of the lateral plantar nerve.16 This nerve passes immediately beneath the calcaneal tuberosity, supplies a motor branch to the abductor digiti quinti, and supplies sensory branches to the periosteum and plantar fascia. In a fifth of cases of inferior heel pain, the pain may be caused by this nerve being trapped between the abductor digiti quinti muscle and the quadratus plantae muscle, or affected by inflammation of the plantar fascia.16
Some authors have proposed that plantar fasciitis may be due to lack of cushioning in a rigid, high arched foot (pes cavus), by increased stretching in a flat foot, or by stretching during over pronation of the foot.1 These hypotheses have not been proved.
Diagnosis
All too often the patient with inferior heel pain is diagnosed as having plantar fasciitis without specific features being elicited and other diagnoses considered. The diagnosis is made on history and physical examination; investigations are used only to rule out other disorders that cause inferior heel pain (fig 1).
The pain initially may be diffuse or migratory; with time it usually localises to the area of the medial calcaneal tuberosity. The patient often gives a history of a gradual onset of pain which is worst on first weight bearing in the morning: the pain may become so incapacitating that the patient limps to the bathroom or hobbles around with the heel off the ground. After a few steps, the heel pain will decrease during the day but will worsen with increased activity (such as jogging) or after a period of sitting. Worse pain in the morning is typical of plantar fasciitis and is usually not a feature of calcaneal stress fractures (in which pain increase with more walking) or nerve entrapment. Nocturnal pain should raise the suspicion of other causes of heel pain such as tumours, infections, and neuropathic pain (including tarsal tunnel syndrome).
The patient may describe an aggravating factor (box) with the discomfort gradually increasing over subsequent weeks. An accurate history of footwear should be obtained: often patients wear shoes with poor cushioning or inadequate arch support, or they walk barefoot on hard floors. Plantar fasciitis is usually unilateral, but it is bilateral in up to 15% of patients17; patients sometimes describe contralateral pain when weight is shifted to the other leg. Bilateral disease in young patients may indicate Reiter's syndrome. Patients should also be asked about other features of seronegative arthritides.1 17
The history should include the patient's general medical condition. Obesity in patients with plantar fasciitis occurs in 40% of men and 90% of women.1 18
Examination
Physical examination in a patient with plantar fasciitis shows localised tenderness on the anteromedial aspect of the heel; firm finger pressure is often necessary to localise the point of maximum tenderness. Slight swelling in the area is common.8 Tightness of the Achilles tendon (dorsiflexion at the ankle limited by 5° or more) is found in 78% of patients.1 8

Lateral radiograph of the os calcis showing erosion due to bursitis in Reiter's syndrome
{kind=link}
There is usually no other clinical finding in the foot and ankle, and if the tenderness is not specific to the calcaneal tuberosity the diagnosis of plantar fasciitis should be questioned. Tenderness in the centre of the posterior part of the heel may be due to bruising or atrophy of the heel pad or to subcalcaneal bursitis.1 Positive percussion (Tinel's sign) on the medial aspect of the heel should lead to a suspicion of entrapment of the nerve to abductor digiti quinti or a tarsal tunnel syndrome. Tenderness on mediolateral compression of the heel (squeeze test) should lead to a suspicion of a stress fracture of the calcaneus.
Investigation
A plain lateral radiograph of the heel is usually taken to rule out a stress fracture, erosions due to bursitis (fig 3), or rare bony causes of inferior heel pain. A heel spur has no diagnostic value.2
Isotope scanning–Williams et al reported that uptake of tracer was increased in 60% of 52 painful heels at the insertion of the plantar fascia or more diffusely over the calcaneus on delayed scanning, but they did not clearly differentiate between stress fractures of the calcaneus and true plantar fasciitis.18 They had no false positive scans in patients without heel pain. Intenzo et al could distinguish between plantar fasciitis and calcaneal stress fractures on the three phase bone scan.19 Isotope scanning is of questionable value early on, and later the diagnosis can usually be made clinically; scanning should be used only when stress fractures are suspected and plain radiographs are normal.
Magnetic resonance imaging and ultrasonography–Magnetic resonance imaging is rarely indicated but may show thickening and inflammation of the fascia.7 Ultrasound examination too may show increased thickness of the plantar fascia and appearances of inflammatory changes.20
Blood tests–A full blood count and erythrocyte sedimentation rate are recommended in patients with bilateral disease or an atypical clinical picture.1 17
Electrophysiological studies–The tarsal tunnel syndrome may sometimes be confirmed,1 but the studies are difficult to perform and interpret. Compression of the nerve to abductor digiti quinti has been shown in research studies,16 but the tests are not clinically useful in most cases.
Treatment
Plantar fasciitis can be a frustrating disorder to treat successfully; success is more likely with a comprehensive treatment programme than with the automatic injection of steroids and prescription of heel cushions. Most authors agree that plantar fasciitis is generally self limiting and that non-operative management hastens recovery, most successfully when treatment is started within six weeks after the onset of symptoms.1 3
Orthoses: heel pads and arch supports–Various rigid, semirigid, and soft shoe inserts are available commercially. Rigid plastic orthoses rarely alleviate the symptoms and often aggravate the heel pain.1 Orthoses made of softer materials provide cushioning by reducing the shock on walking by up to 42%. Because the plantar fascia is stretched during flattening of the foot, we prefer orthoses designed to maintain the medial longitudinal arch during ambulation and prescribe full length or 3/4 length accommodative inlays of medium density plastazote (fig 4).

An accommodative insole of a soft material will provide shock absorption and decrease stretching of the fascia during ambulation
{kind=link}
Advice on footwear–Patients should be advised not to walk barefoot on hard surfaces. Shoes should have an arch support and cushioned heels.21 Worn shoes may aggravate plantar fasciitis because of lack of cushioning. A laced sports shoe is better than open sandals.
Non-steroidal anti-inflammatory drugs–Oral anti-inflammatory drugs provide pain relief and are useful in decreasing the inflammation1; they should be prescribed for acute pain and should be withdrawn as the pain subsides, with monitoring for complications. Some patients say that topical non-steroidal anti-inflammatory creams or gels are useful.
Local steroid injection—A steroid injection alone or a combination of steroid and local anaesthetic can provide pain relief in an exquisitely tender area. An injection is best given from the medial rather than the inferior aspect of the heel22; a series of minor withdrawals and reinsertions are necessary so as to infiltrate the whole breadth of the superior aspect of the inflamed fascia, avoiding the inferior surface so as not to cause fat pad atrophy.
Steroid injections are not without complications. Cushioning may be lost through fat pad atrophy, and they may lead to osteomyelitis of the calcaneus23 or iatrogenic rupture of the plantar fascia.4 A prospective randomised study found no significant difference between lignocaine alone and lignocaine plus steroid.24 We no longer advocate steroid injections for first line management but occasionally use them in patients with refractory symptoms.
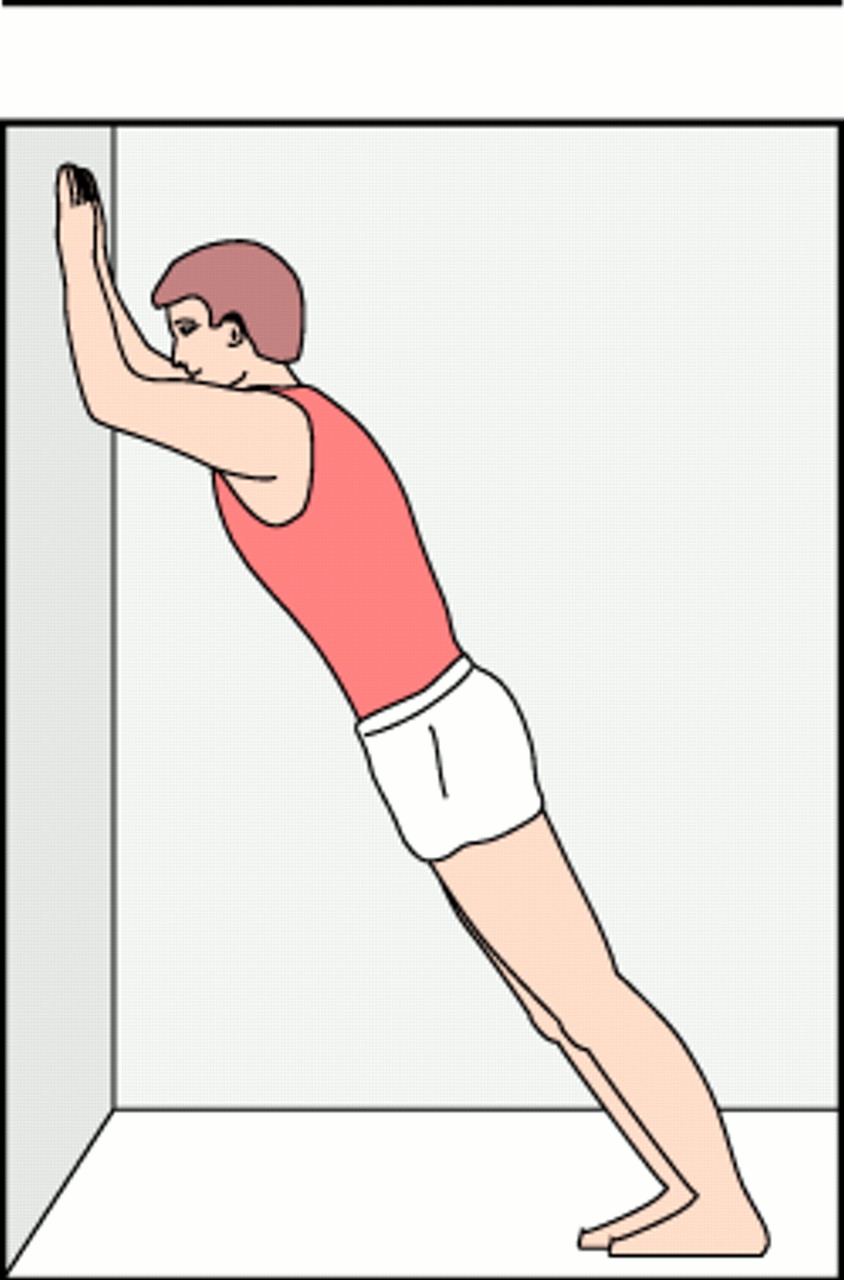
Exercises for stretching the Achilles tendon–Most patients with plantar fasciitis have tightness of the Achilles tendon1 6 11 16; stretching it interrupts a cycle in which the two disorders aggravate each other. Patients should be instructed to stretch the gastrocnemius and soleus components of the triceps surae independently: the gastrocnemius is stretched by keeping the knee extended while passively dorsiflexing the foot (fig 5), whereas the soleus is stretched by flexing the knee while dorsiflexing the foot. Patients should be encouraged to repeat the gentle, sustained stretches at least 10 times, five or six times daily.16

Gentle, sustained stretching of the Achilles tendon by leaning onto a wall while keeping heels on the ground and knees straight
{kind=link}
Night splints–A moulded ankle-foot orthosis is used to hold the plantar fascia and Achilles tendon in a relative position of stretch during the night. It holds the ankle fixed in 5° of dorsiflexion and the toes slightly dorsiflexed. For most patients this orthosis reduces morning pain considerably; Wapner and Sharkey had a 79% cure rate after patients used the splint for an average of four months.25
Below knee casts–Patients with severe pain and marked limitation of activity are best treated with a moulded, below knee, walking cast for three to four weeks. It provides relative rest, reduces pressure on the heel at heel strike, provides an arch support, and prevents tightening of the Achilles tendon.
Other non-surgical measures–Strapping the foot to hold the plantar fascia in a favourable and relaxed position during weight bearing has been proposed,26 and intrinsic muscle exercises have been advocated.1 26 We have not used ultrasound, contrast baths, acupuncture, or radiotherapy. Athletes often find relief with ice massage of the area before and after exercise.1
Surgery–Surgical intervention should be considered only for intractable pain which has not responded to 12 months of proper conservative treatment.16 Reports describe various surgical procedures, including plantar fascia release with or without calcaneal spur excision, Steindler stripping, neurolysis, and endoscopic procedures.13 26 All authors claim success with their chosen method; others believe that surgery provides satisfactory results in only 50-60% of cases1 and that complications are substantial. The surgical procedure should be individualised for each patient.26 Baxter recommends that only 40% of the plantar fascia should be incised to avoid flattening of the arch and recommends division of the deep fascia of abductor hallucis to decompress the nerve to abductor digiti quinti.16 Our management plan (box) uses multiple conservative modes of treatment with an aim of hastening recovery without harming the patient. It is important, but difficult, to make the patient understand that treatment consists of several methods and that a total, not a fragmented, effort is necessary. The patient is reassured that the condition is generally self limiting over a course of several months; we also often have to allay the patient's anxiety that the bone spur is causing the symptoms and should be removed.
Management plan
Initial visit:
Explanation of the disorder
Identification of risk factors
Advice on footwear
Oral anti-inflammatory drugs
Exercises for stretching the Achilles tendon
Orthoses (generally over the counter ones)
Night splints
Later visits:
Injection of lignocaine plus corticosteroid
Customised orthotic device
Total contact (below knee) cast
Davis et al reported resolution of pain in 90% of 132 painful heels in 11 months of using a similar regimen, which did not include night splints or occasional casting.27 Stretching was rated as the most effective treatment.
Acknowledgments
We are grateful to Mrs Colleen Power and Mr Richard Hudson for the illustrations.
Funding: None.
Conflict of interest: None.