Article Text

Statistics from Altmetric.com
Norway’s Professor Roald Bahr recently highlighted that screening does not predict which athlete will sustain an injury.1 Some interpreted this to mean screening is useless for injury prevention. However, screening remains essential in our efforts to protect athletes’ health. To extend what has been a robust discussion, we argue how screening can be important for an individual athlete, and offer potential reasons why and how individual screening tests still lack clinical utility.
Positive predictive value and the prevention paradox
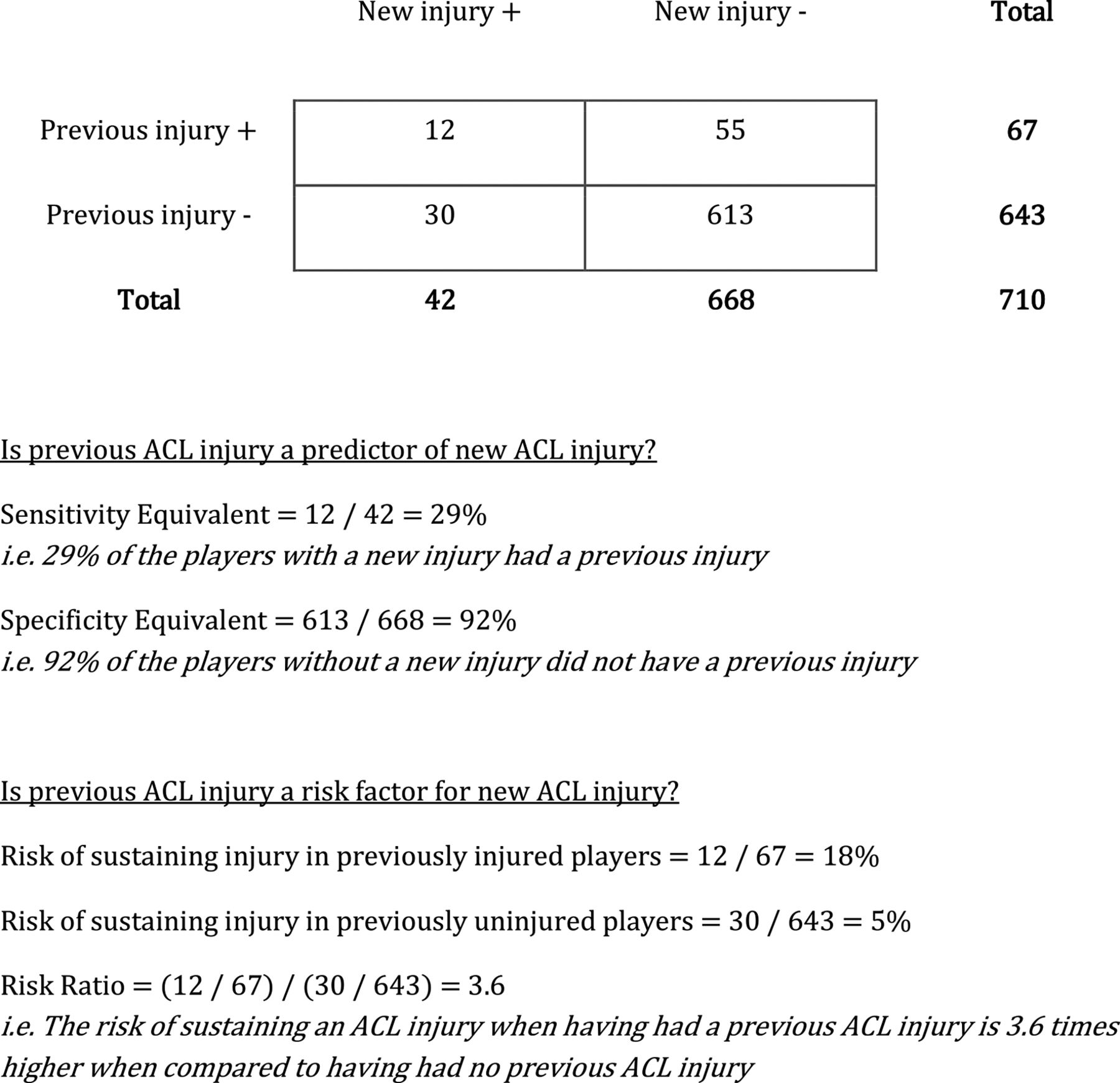
Previous injury is a well-established injury risk factor. Figure 1 shows data on ACL (re)injuries from Krosshaug et al.2 Applying a traditional (predictive) diagnostic test on these data yields unimpressive results; a positive predictive value of only 29%, with most injuries occurring in previously uninjured athletes. If effective interventions target only previously injured athletes, it would be withheld from the majority of athletes who could benefit. Consequently, we agree with Bahr,1 that all athletes receive effective interventions.

The relationship between unilateral ACL injuries and ACL reinjuries in a multiseason prospective cohort study in female football and handball players. (Based on original data from Krosshaug et al.2
But consider another perspective on the same risk factor ‘previous injury’. Regardless of the low predictive value, previous injury is associated with a 3.6-fold reinjury risk. Does this mean we should give all athletes a knee injury prevention programme regardless of their individual injury histories? We know this does not usually happen in clinical practice. Diligent clinicians will perform a battery of tests based on the athlete’s injury history, and implement interventions customised to the athlete’s impairments and activity limitations. Such interventions are provided to previously injured athletes over and above any universal prevention efforts already in place for the entire team.
Enter the prevention paradox, as first described by London epidemiologist Geoffrey Rose.3 The majority of injuries are sustained by athletes who are at low to moderate risk for injury—high-risk athletes sustain only a minority of injuries. The paradox is that a universal prevention approach in a low-risk population will in absolute terms benefit more athletes than a targeted approach in high-risk individuals. In sports medicine, we can use both approaches where appropriate, and for that we need to better understand the value and limitations of identifying injury risk through screening.
Predicting injury versus estimating risk of injury
Screening is a strategy to identify an unrecognised disease in individuals with or without symptoms.4 Analytical approaches towards screening are designed to establish if a test suggests or contradicts a particular diagnosis. In sports, the analogous context would be to determine if a screen confirms if an athlete is injured. However, the goal of injury prevention is to intervene before the injury occurs. This is a very different context. In risk factor screening, to facilitate appropriate decision-making and potential intervention, one is looking for individuals who possess exposures or traits that increase their likelihood of sustaining an injury. However, there are two limitations to paradigms commonly used in screening that are expected to show weak results even if the risk factors were truly associated with injury. These are (1) complexity and (2) temporality of injury risk factors.
Complexity: sports injuries do not arise in isolation
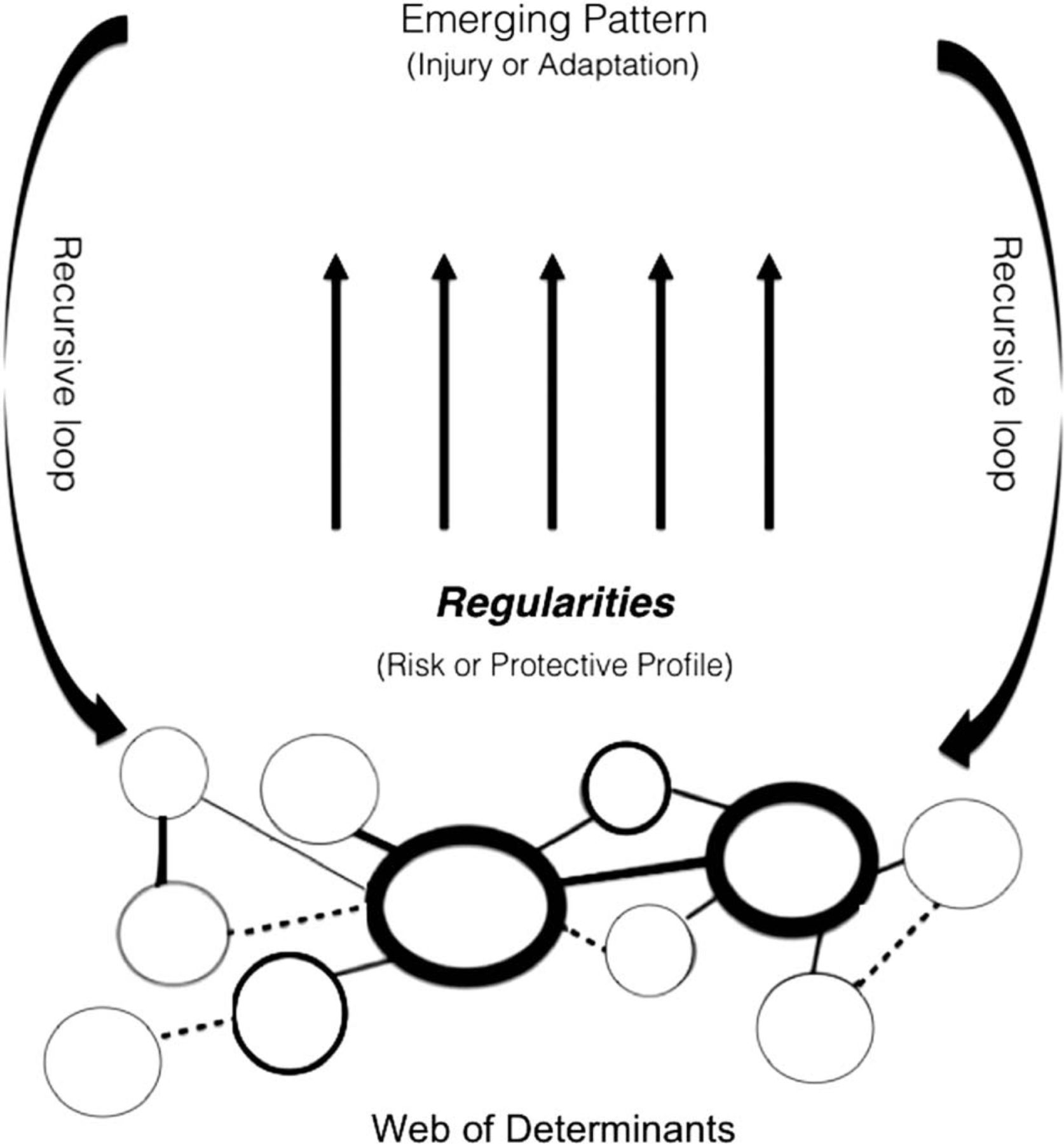
The latest iteration of Meeuwisse’s aetiological model touched upon the complexity of injury aetiology (figure 2).5 An injury occurs when different intrinsic and extrinsic injury risk factors interact with a timely injury mechanism. As such complex situations are unpredictable, and analytical strategies must reflect this reality or ‘screening’ will appear useless. Unfortunately, current strategies assume that individual risk factors can identify which athlete will encounter such complex situations by which any single risk factor will have ‘poor’ diagnostic test properties. The reasoning is similar to why single physical examination tests perform poorly. Swelling, for example, is not diagnostic as multiple different injuries can cause it. Nonetheless, a combination of physical examination tests remains useful when properly interpreted.6 Therefore, even though individual screening tests have seemingly limited value when analysed in isolation, they may provide meaningful information when interpreted in combination with other factors out of a physical examination. It is the responsibility of those advocating tests to perform the appropriate studies toidentify which combination of tests is useful in which context.

{kind=link}
{kind=link}
Complex model for sports injuries.5
Temporality: risk factors do not stand still
Risk factors are temporal—they vary over time. The interpretation that screening tests are useless (because they cannot predict injury) is based on results that did not account for this temporal nature. Most studies aim to identify injury risk factors by screening athletes at a set point in time and measure injury rates over the following months or years. If we could repeatedly perform ‘screening tests’ we would note that the test results would fluctuate over time due to several different factors, including training and match demands. Such mediating factors might affect the variables tested during screening, or alter them altogether.7 Also, importantly, those athletes with risk factors identified at baseline are likely to be treated so their risk should decline. Therefore, the heightened risk is temporary, and ‘static snapshot’ screening outcomes will fail to identify risk factors for injury even if it were indeed risk factors. We recommend analytical approaches that incorporate repeated measures and monitoring of variables over time, adjusted appropriately for interventions that occur after screening test results.8
Keep the baby, throw out the bathwater
Recent debate questions the effectiveness and efficiency of screening as part of the injury prevention process.1 We feel this instigated fruitful discussion, but we must develop a greater appreciation for the underlying complexity of injury prevention concepts. If we simply disregard the value of screening based on the findings of current studies with methodological limitations, we will be at risk of oversimplifying a complex problem. Instead, there is a need to continue to improve the methods we apply, to have a greater appreciation for the clinical context of the questions we aim to answer and to interpret the results accordingly.
Footnotes
Contributors EV conceptualised the manuscript. All authors contributed in writing of the editorial.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.