Article Text

Statistics from Altmetric.com
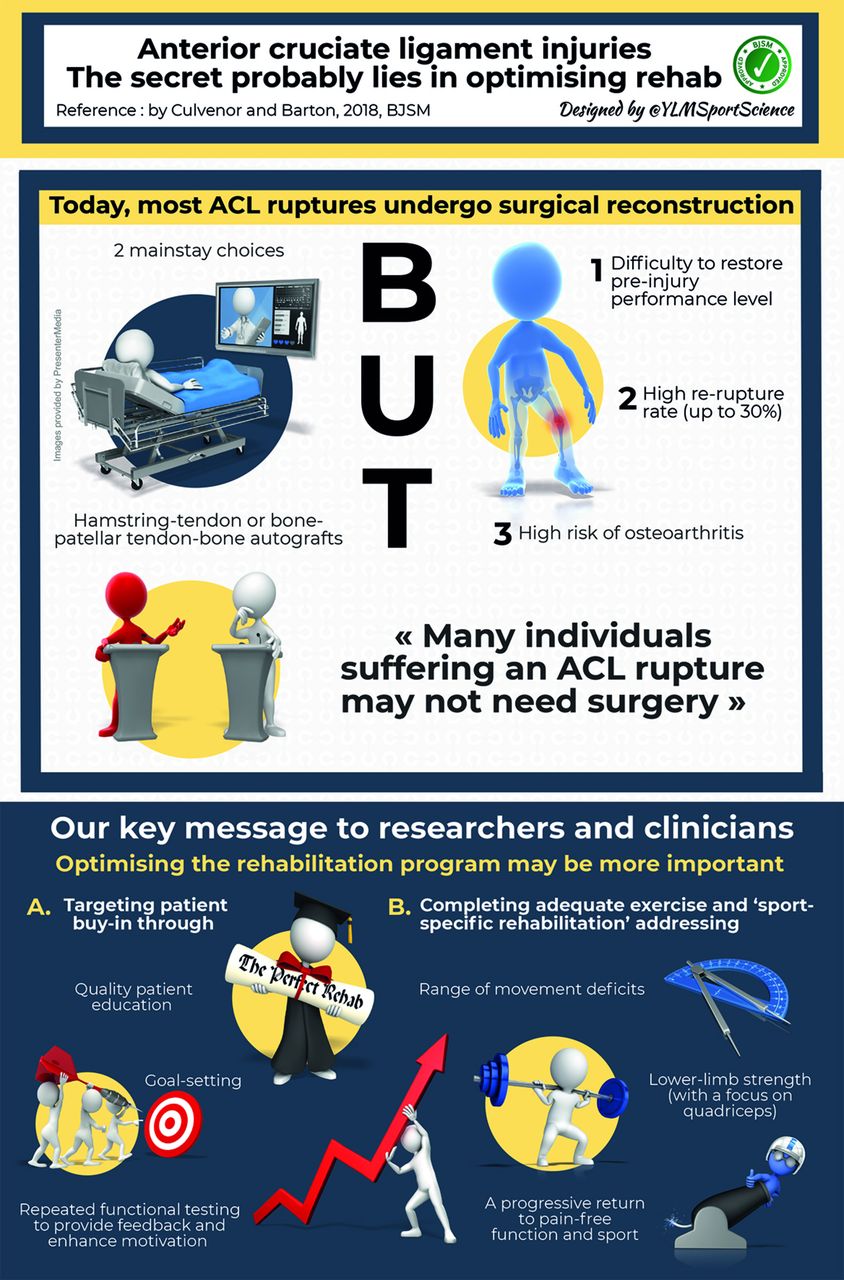
Since the first report of surgical repair for a ruptured cruciate ligament in 1895, a great deal of research has attempted to identify the optimal surgical technique. Today, the two mainstay choices are hamstring–tendon and bone–patellar tendon–bone autografts, with preferences differing around the globe.1
Systematic reviews of randomised controlled trials have identified very few differences in outcomes more than 2 years postoperatively between these two popular graft choices.2 Similarly, variations of surgical technique, such as double-bundle reconstruction, while potentially providing greater passive stability, offer no proven superior clinical or functional outcomes.3
Clinician’s and researcher’s quest for the Holy Grail—a quick return to sport without re-injury or increased osteoarthritis risk—has led to less conventional management approaches. This includes an alarming resurgence of synthetic ligaments as described in a recent BJSM blog (http://blogs.bmj.com/bjsm/2017/07/06/synthetics-ligaments-knee-deja-vu-innovation/). Do we really need to pursue unconventional surgical interventions that have failed to stand the test of time?
Perhaps the secret for clinicians and researchers lies not in chasing the next sexy surgical trend but in ensuring completion of an outstanding rehabilitation programme. Dare we say it: many individuals suffering an ACL rupture may not need surgery.4 Optimal non-operative management may even fast track a return to competitive sport. A recent BMJ Case Report detailed an elite English Premier League player’s return to full competition within 8 weeks of a complete ACL rupture with a problem-free follow-up at 18 months.5 And importantly, you cannot re-rupture a graft that does not exist.
Evidence for considering a progressive non-operative approach to ACL injury management is not isolated to case studies of patients with access to elite medical teams. The prominent KANON trial—the only high-quality randomised controlled trial comparing early reconstruction to rehabilitation alone (with the option of delayed reconstruction if indicated) for acute ACL injury—clearly demonstrated that functional, symptomatic, radiographic and activity level outcomes do not differ up to 5 years postinjury in non-elite athletes.4 If surgery is to continue in practice, perhaps research endeavours to identify those who might benefit should be the focus, rather than what seems to be less rewarding efforts to identify better graft and surgical approaches.
If surgery did not make a difference in outcomes, what did?
The difference in achieving outstanding functional outcomes, irrespective of surgical or non-surgical management, was physical performance (one-leg rise).6 Preventing a delayed ACL reconstruction in those starting with rehabilitation alone was also related to higher physical performance (vertical hop).6
With evidence clearly showing the benefits of (at least) trialling a non-operative approach for ACL injury management in most scenarios, and in cases of ACL reconstruction, completing a well-designed progressive postoperative rehabilitation programme, do we need to make rehabilitation and exercise therapy more appealing? Is it any wonder that patients often wish to avoid the arduous, dull and boring sounding ‘conservative management’ when they can get a ‘quick fix’ from the surgeon? But with re-rupture rates so high and no apparent benefit based on current high-quality research, this surgical ‘fix’ is not necessarily a fix.
Optimising rehabilitation programmes
The best exercise is the exercise that gets done. It is time we translated evidence-based rehabilitation programmes into clinical practice. There is an alarming underutilisation of rehabilitation, with 45% of community-level athletes discontinuing supervised rehabilitation by 3 months post-ACLR.7 Achievement of physical resilience before return-to-sport is unlikely and may be a key contributor to failed return-to-sport with or without surgery.
Targeting patient buy-in through quality individualised patient education, goal-setting and repeated functional testing to provide feedback and enhance motivation to complete adequate exercise and ‘sport-specific rehabilitation’ based on accepted resistance training principles should be a priority for all clinicians. In particular, identification of individual patient needs, co-creation of patient-specific goals and co-design of rehabilitation between clinician and patient, as opposed to prescriptive approaches dictated by clinicians, may optimise patient engagement and adherence. The world leaders in this field use these approaches successfully to achieve outstanding outcomes.8
Based on current research, we propose the first-line treatment for people following ACL injury should be ensuring adequate exercise rehabilitation involving addressing range of movement deficits, lower-limb strength (with a focus on quadriceps) and a progressive return to pain-free function and sport. Surgery may remain relevant in some if unable to achieve adequate function with rehabilitation alone, but may not be the key determinant of return-to-sport or prevention of osteoarthritis. In light of these points, it is time to shift clinical and research focus from ‘sexy’ new synthetic graft and other surgical innovation research to understanding who needs any form of surgery and ensuring all patients receive adequate (and wherever possible, intense and progressive) exercise rehabilitation.
{kind=link}
Acknowledgments
The authors would like to thank Yann Le Meur (
@
YLMSportScience)
for creating the infographic and Jorge Rodriguez (
@
fisioterapianet)
for creating the animation video, both of which summarise the key information on this topic in highly engaging formats.
Footnotes
Contributors AGC and CJB conceived the concept for the information and call to action in this manuscript and approved final versions of the infographic and video. YLM produced the infographic. JR produced the video.
Funding AGC is a recipient of a National Health and Medical Research Council (NHMRC) of Australia Early Career Fellowship (Neil Hamilton Fairley Clinical Fellowship No. 1121173).
Disclaimer The funding sources had no involvement in any aspect of this educational review.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; internally peer reviewed.