Article Text

Statistics from Altmetric.com
In a well controlled and designed study, Baker et al1 clearly showed the effects of ingesting large volumes of water or a carbohydrate/electrolyte sports drink (CES) on serum Na+ concentration ([Na+]) during exercise in older, active adults (54–70 years). The data show that ingesting any hypotonic fluid, be it water or a Na+-containing sports drink (about 18 mmol/l), in volumes that are similar to or more than weight losses produces a fall in [Na+]—a finding that mirrors the study of Twerenbold et al published in this journal.2 Readers should know that any fluid of concentration less than 150 mmol/l is considered to be hypotonic to the plasma.
In the study of Baker et al,1 the ingestion of a CES produced a lower rate of fall in [Na+], as also found by Twerenbold et al2 and also by Barr et al.3 However, the authors failed to conclude that the consumption of any hypotonic fluid at these rates nevertheless causes a steady decline in serum [Na+]. Instead, Baker et al1 concluded that a CES better restores plasma volume and is therefore a more effective fluid replacement in older adults during intermittent exercise. This conclusion ignores the fact that, in their trial, serum [Na+] in both the men and women fell during exercise, regardless of the type of fluid they were ingesting, and that a falling serum [Na+] will eventually lead to hyponatraemia and its associated symptoms and medical complications.
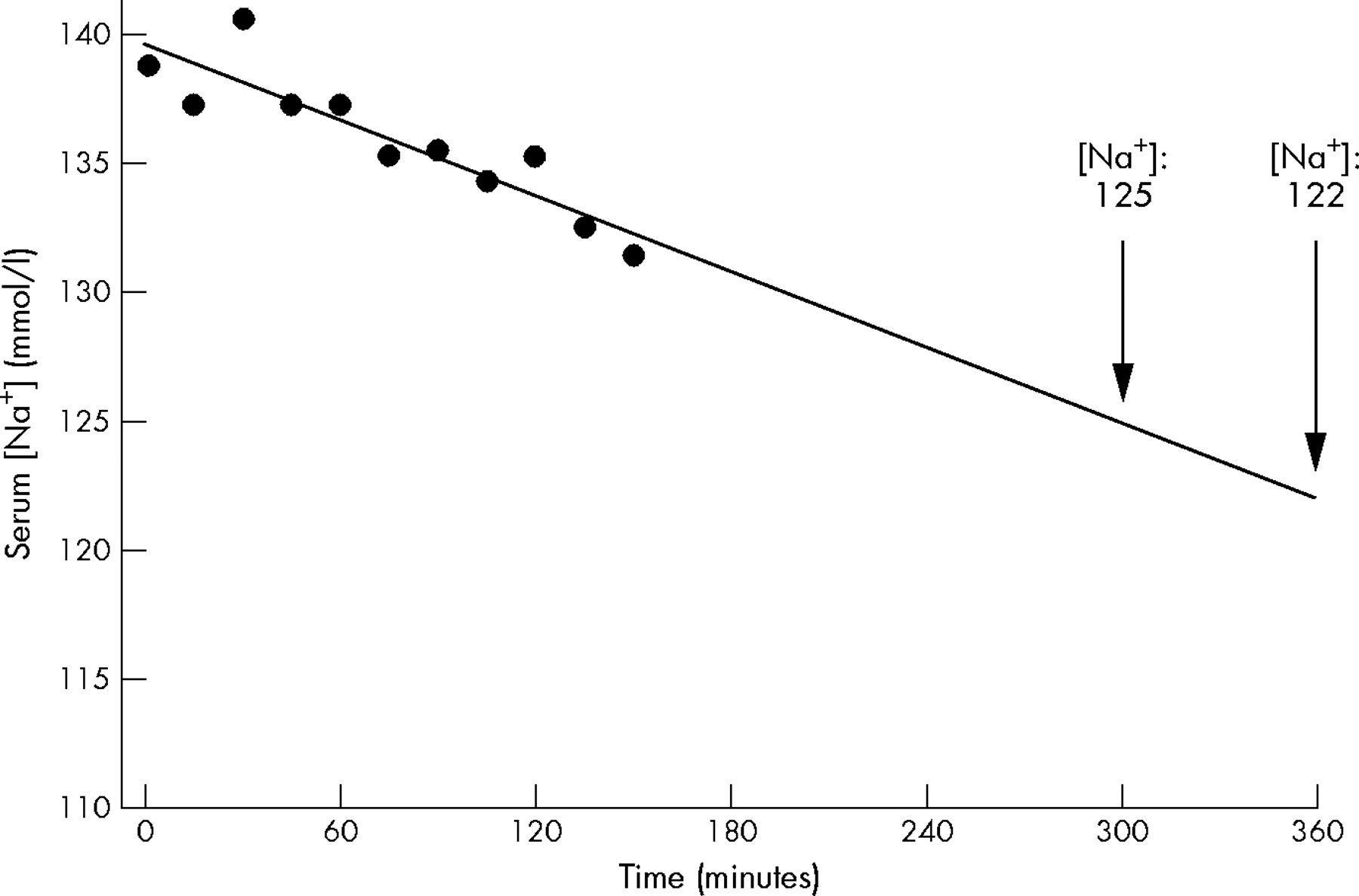
One female subject in the study of Baker et al1 lowered her [Na+] by nearly 10 mmol/l in just 150 minutes when voluntarily consuming 2.7 litres of CES. I have replotted her data to show that, had she continued drinking the CES at that rate and given a relatively constant rate of decline, after four hours her serum [Na+] would be about 128 mmol/l. After five hours it would have reached 125 mmol/l, and after six hours it would likely have been 122 mmol/l (fig 1). As these are serum Na+ concentrations at which cerebral and pulmonary oedema develop,4 and at which emergency medical treatment is necessary, this finding is of particular significance.

{kind=link}
Linear regression (r2 = 0.81; p<0.05) of the fall in [Na+] during exercise in one female subject in the study of Baker et al.1 The rate of decline is approximately 3.3 mmol/l Na+/l per hour when a carbohydrate/electrolyte sports drink is ingested at a rate of approximately 1.1 litres/h.
In 2000, the average 42.2 km marathon finishing time for women in North America was 4:57 (h:min). In the 2005 San Diego marathon alone there were 9069 women finishers, of whom about 2985 finished in 4–5 h, 2379 finished in 5–6 h, and 2531 in 6–9 h.5 If these marathon finishers were to consume CES at the rates advocated by Baker et al and elsewhere6 to prevent “voluntary dehydration,” the number of hyponatraemic cases and their associated medical complications would be sure to increase, placing undue pressure on medical directors and their staff who must diagnose and treat this preventable yet complicated condition.
Of particular concern is the fact that sports drink companies, as well as the American College of Sports Medicine (ACSM) drinking guidelines,6 currently advocate that sports drinks that contain Na+ should be consumed to prevent hyponatraemia during prolonged exercise. However, the data of Baker et al clearly show that the consumption of any hypotonic fluid in quantities to prevent “voluntary dehydration” will inevitably produce a fall in serum [Na+], which can eventually lead to symptomatic hyponatraemia.
To help prevent any further increase in the number of cases of this preventable condition, I feel that this alternative interpretation of the data of Baker et al should be brought to the attention of the readers of this journal.
Footnotes
-
Competing interests: none declared