Article Text

Abstract
Objectives: To determine the effectiveness of eccentric exercise (EE) programmes in the treatment of common tendinopathies.
Data sources: Relevant randomised controlled trials (RCTs) were sourced using the OVID website databases: MEDLINE (1966–Jan 2006), CINAHL (1982–Jan 2006), AMED (1985–Jan 2006), EMBASE (1988–Jan 2006), and all EBM reviews – Cochrane DSR, ACP Journal Club, DARE, and CCTR (Jan 2006). The Physiotherapy Evidence Database (PEDro) was also searched using the keyword: eccentric.
Review methods: The PEDro and van Tulder scales were employed to assess methodological quality. Levels of evidence were then obtained according to predefined thresholds: Strong–consistent findings among multiple high-quality RCTs. Moderate–consistent findings among multiple low-quality RCTs and/or clinically controlled trials (CCTs) and/or one high-quality RCT. Limited–one low-quality RCT and/or CCT. Conflicting–inconsistent findings among multiple trials (RCTs and/or CCTs). No evidence–no RCTs or CCTs.
Results: Twenty relevant studies were sourced, 11 of which met the inclusion criteria. These included studies of Achilles tendinopathy (AT), patella tendinopathy (PT) and tendinopathy of the common wrist extensor tendon of the lateral elbow (LET). Limited levels of evidence exist to suggest that EE has a positive effect on clinical outcomes such as pain, function and patient satisfaction/return to work when compared to various control interventions such as concentric exercise (CE), stretching, splinting, frictions and ultrasound. Levels of evidence were found to be variable across the tendinopathies investigated.
Conclusions: This review demonstrates the dearth of high-quality research in support of the clinical effectiveness of EE over other treatments in the management of tendinopathies. Further adequately powered studies that include appropriate randomisation procedures, standardised outcome measures and long-term follow-up are required.
- AT, achilles tendinopathy
- CCT, clinically controlled trial
- CE, concentric exercise
- EE, eccentric exercise
- FAOS, foot and ankle outcome score
- LET, lateral elbow
- PED, physiotherapy evidence database
- PT, patella tendinopathy
- RCT, randomised controlled trial
- RR, relative risk
- VAS, visual analogue scale WMD, weighted mean difference
- tendinopathy
- eccentric
- systematic review
Statistics from Altmetric.com
- AT, achilles tendinopathy
- CCT, clinically controlled trial
- CE, concentric exercise
- EE, eccentric exercise
- FAOS, foot and ankle outcome score
- LET, lateral elbow
- PED, physiotherapy evidence database
- PT, patella tendinopathy
- RCT, randomised controlled trial
- RR, relative risk
- VAS, visual analogue scale WMD, weighted mean difference
Tendinopathy is the preferred term used to describe various tendon pathologies, including paratendinitis, tendinitis and tendinosis in the absence of biopsy-proven histopathologic evidence.1 Tendinopathy of the Achilles tendon (AT) alone has been reported to constitute 7–9% of total injuries in top-level runners.2 Other tendinopathies are also prevalent:1–2% of the general population have been reported as experiencing tendinopathy in the common wrist extensor origin of the lateral elbow (LET),3 and 20% of all knee injuries (n = 266) assessed in a sports clinic setting over six months were diagnosed as patella tendinopathy (PT).4 Other common sites of tendinopathy include the proximal hamstring insertion, the rotator cuff tendons, and the wrist flexor tendon insertion at the medial elbow.5 Considering the prevalence of these tendinopathies, the determination of modalities effective in treating tendon pathology remains important.3,6
Various modalities have been recommended as appropriate treatment options for tendinopathy, depending upon the phase of presentation. In the acute phase of treatment, reduction of risk factors such as training errors,6 flexibility issues6,7,8,9,10 and biomechanical abnormalities,6,8,11along with symptom reduction using relative rest,9,10,12 ice,7,8,10 and physical modalities such as ultrasound and laser have been suggested.6,7,8,9,10 In chronic, long-standing cases, a complete rehabilitation programme incorporating strengthening,6,7,9,11–19 flexibility,6 proprioception,6 massage9,11,12 and endurance6 has been recommended. Eccentric exercise (EE) strengthening programmes have been emphasised recently as a key element of strength training in rehabilitation,6–9,11–13,15,17–24 in part due to literature supporting their use in the treatment of AT.25–27 In more recent, non-systematic reviews, EE has been recommended as a treatment modality for other tendinopathies such as PT and LET.6,19,28
It has been proposed that EE may counteract the failed healing response which apparently underlies tendinopathy, by promoting collagen fibre cross-linkage formation within the tendon, thereby facilitating tendon remodelling.19,21 However, as the basic pathophysiology of tendinopathy is still poorly understood, the mechanisms by which EE may help resolve tendinopathy remain hard to determine. Beyond this, it is essential that the clinical effectiveness of physical modalities such as EE is established as a matter of priority.
To date no systematic review has investigated EE and its effectiveness in tendinopathy rehabilitation. Therefore, this systematic review was undertaken to evaluate the current evidence for the effectiveness of EE programmes in the treatment of common tendinopathies.
METHODOLOGY
Aim
The aim of this systematic review was to evaluate the evidence for the effectiveness of EE programmes in the treatment of common tendinopathies.
Search strategy
The following databases were searched using the OVID website:29 MEDLINE (1966–Jan 2006), CINAHL (1982–Jan 2006), AMED (1985–Jan 2006), EMBASE (1988–Jan 2006), and all EBM reviews – Cochrane DSR, ACP Journal Club, DARE, and CCTR (Jan 2006). A defined search strategy was implemented incorporating the first two phases of a highly sensitive search strategy for OVID MEDLINE.30 Keywords used in the initial phase of the search included: tend*, eccentric*, Achill*, patell*, epicondyl*, tennis elbow, and rotator cuff (table 1). The Physiotherapy Evidence Database (PEDro)31 was also searched using the keyword: eccentric; and a hand search of three prominent sports medicine journals was undertaken: the British Journal of Sports Medicine (1995–Jan 2006), the American Journal of Sports Medicine (1995–Jan 2006) and the online resource of the Scandinavian Journal of Medicine and Science in Sports (2000–Jan 2006).
Predefined search strategy used for OVID databases
Inclusion and exclusion criteria
Randomised controlled trials investigating the use of EE to treat tendinopathy of the Achilles tendon, patella tendon, common wrist extensor tendon origin, or rotator cuff tendons were included. Other less common tendinopathies fell outside the scope of this review. Studies where at least one treatment group received an EE programme as the mainstay of treatment were included. Study participants must have been diagnosed clinically with tendinopathy of the studied tendon. Both mid-portion and insertional tendinopathies were included.
There were no restrictions placed on age, gender or activity level of the study participants, and non-English studies were eligible for inclusion. Co-interventions were allowed alongside EE in the intervention group as long as they were standardised. Studies that included participants who had previously ruptured, or had undergone surgery of, the involved tendon were excluded as were studies that compared two different types of EE programmes without a control group.
Outcome measures
The clinical outcome measures of interest in this review were pain, function and patient satisfaction/return to activity.
Pain has been defined by the International Association for the Study of Pain (IASP) as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage and described in terms of such damage”.32 All pain scales were included in the review, but with conclusions based on the reliability and validity of pain scale used. A recent review of pain measurement methods recommended the visual analogue scale (VAS)33 and the McGill Pain Questionnaire34 as the most reliable and sensitive tools for pain measurement.35
Function may be defined as an activity that is natural to, or the purpose of, a person or thing.36 Functional assessment has also been defined as “any systematic attempt to measure objectively the level at which a person is functioning, in any of a variety of areas such as physical health, quality of self-maintenance, quality of role activity, intellectual status, social activity, attitude towards the world and self, and emotional status”.37
Therefore, outcomes that objectively measured any part of function were included in the review: e.g. strength, or range of movement.
The third outcome measure of interest was patient satisfaction/return to sport/return to activity, which are now accepted widely as a necessary part of outcome assessment;38 for the purposes of this review these were analysed together as one dichotomous outcome.
Studies that reported at least one of these three clinically orientated outcomes were included in the systematic review.
Quality assessment
The PEDro31 and van Tulder39 scales were used to assess methodological quality.
The PEDro scale is based on the Delphi list,40 and its reliability has been reported as being “fair” to “good” in a recent assessment;41 Maher et al (2003) therefore concluded that the PEDro scale had sufficient reliability for its use in systematic reviews of physiotherapy randomised controlled trials (RCTs). The PEDro scale consists of 11 criteria, of which the first is not included in the final internal validity score. The answer to each criterion is a simple yes/no and the score is expressed as a mark out of 10. To achieve a ‘yes’, it must be explicitly clear upon reading the article that the criterion has been satisfied.
The van Tulder scale is the methodological quality scale utilised in the updated guidelines for systematic reviews of the Cochrane Collaboration back review group.39 The internal validity portion of this scale consists of 11 criteria and the answer to each may be yes/no/don’t know. In the case of a ‘don’t know’, the authors were contacted to help clarify the answer. If there was no reply or it remained unclear, the answer stayed as a ‘don’t’ know’.
Three assessors (BW, DB and RNW) independently reviewed the included articles and a consensus was reached to determine the final quality scores. The PEDro scores for articles found in the PEDro database were subsequently compared to those available on the website.
Methodological scores were calculated for each study and the two scales were then compared to determine whether these were consistent measures of quality. The studies were then rated as high or low quality based on definitions used in a previous systematic review using the van Tulder scale.42 A high-quality study was defined as satisfying six or more of the 11 quality criteria in the van Tulder scale, and six or more of the 10 criteria in the PEDro scale. Studies that did not meet this level were rated as low quality.
Levels of evidence were then determined using the following criteria:39Strong–consistent findings among multiple high-quality RCTs. Moderate–consistent findings among multiple low-quality RCTs and/or clinically controlled trials (CCTs) and/or one high-quality RCT. Limited–one low-quality RCT and/or CCT. Conflicting–inconsistent findings among multiple trials (RCTs and/or CCTs). No evidence from trials–no RCTs or CCTs.
Data management and statistical analysis
Where possible, the mean differences between pre-treatment scores and post-treatment scores were calculated for continuous data sets: a standard deviation was then obtained for the mean differences assuming a covariance of zero. For dichotomous data, the numbers of events in each group were extracted along with the groups’ sample sizes. If a study reported data that were not adequate for inclusion in the analysis, all efforts were made to obtain it from the relevant author. Values were then entered for analysis into Review Manager 4.2.8 software,43 which is commonly used for meta-analysis of data in Cochrane Collaboration systematic reviews.
The results are expressed as a weighted mean difference (WMD) or relative risk (RR) and 95% confidence intervals (CI), depending on the type of data entered, and are based on the random effects model. The statistical significance level was set at p = 0.05 for all results. Sample size calculations were obtained using an online calculator,44 in collaboration with a biostatistician.
RESULTS
Selection of studies
The initial search resulted in 450 titles from the included databases (fig 1); of these, 252 were discarded as duplicate references, leaving a total of 198. The hand search of three sports journals resulted in no further inclusions. Of these 198 articles, 185 were excluded based on the title and/or abstract: eight were reviews, four did not have EE as a treatment group and 173 did not investigate tendinopathy, leaving 13 potential articles.27,45–56 The articles’ reference lists were then checked for additional studies and a further seven potential articles were found.57–63 At this stage a second eligibility screening was done on the 20 articles and a further nine were excluded: three were not randomised,47,48,64 two included treatment and control groups that both received EE programmes,49,56 one did not report any of the included primary outcome measures adequately58 and three investigated strength programmes other that eccentric training.58,60–62 Thus, a total of 11 articles were included in the current review.

Study selection process. Flow-diagram based on the QUOROM guidelines.65 RCT, randomised controlled trial; EE, eccentric exercise.
Description of studies
The characteristics of each included study can be found in table 2. In total, 443 tendons from 250 males and 172 females were included in the 11 trials. Seven studies reported drop outs,45,46,50,52,54,55,63 with a mean percentage drop out rate of 12.5% (range 6.5–17.4%). All studies gave descriptive statistics on age of subjects with an overall mean of 36.5 years. The duration of symptoms were reported in nine studies with a mean of 19.7 months. Four studies investigated subjects diagnosed with AT,27,50,52,59 four investigated subjects with PT45,53,55,57 and the remaining three investigated subjects with LET.46,54,63 Randomised studies investigating the effect of EE on rotator cuff or other less common tendinopathies were not found.
Characteristics of included studies
Studies included interventions of EE programmes of varying lengths: a 12-week exercise programme was undertaken in eight studies,27,45,50,52,54,55,57,59 while two other studies implemented a four-week programme53,63 and one study implemented a six-week programme.46 Comparison groups included concentric exercise (CE) programmes,27,45,46,52,57,59 stretching,46,54 ultrasound,53,63 frictions,53 splints,50 or normal training.55 The length of follow-up varied from six weeks46 to one year.50,52,54 The most common follow-up time point was immediately after the conclusion of treatment at 12 weeks.27,45,55,57,59
Various outcome measures were used in the included studies. The most common was patient satisfaction or return to activity outcomes, with seven of the 11 studies reporting this outcome.27,45,52,54,57,59,63 Six studies used a pain VAS as their pain outcome measure;27,45,46,52,54,57 however, three of these studies27,54,57 failed to report the VAS data in sufficient detail to be used in statistical analysis. Other studies utilised either a ten-point numerical rating scale59 or a five-point ordinal rating scale.53 Functional outcome measurement varied significantly amongst the trials with no consistency between studies: measures included Victorian Institute of Sport Assessment (VISA)66,67 scores,45,55 muscle strength,54 disabilities of the arm, shoulder and hand (DASH)68 scores,46 Foot and Ankle Outcome (FAOS)69 scores,50 Ko70 scores,63 and peak muscle torque values.57
Methodological quality
The internal validity scores for the included studies are shown in figs 2 and 3. The median score for methodological quality of the included studies was 7 out of 11 for the van Tulder score (range of 5 to 9), and 6 out of 10 for the PEDro score (range of 5 to 8). Using the cut-off point of 6 in both scales for high-quality studies, six studies attained a high-quality rating.46,50,52,55,57,63

PEDro31 scores for included studies. Studies are ordered by PEDro score. Criteria 1 omitted as not included in internal validity scores. ▪ = criteria met; □ = criteria not met.

van Tulder39 scores for included studies. Studies are ordered by van Tulder score. ▪ = criteria met; □ = criteria not met; ? = don’t know.
The PEDro scale results showed that in all studies subjects were randomly allocated to groups (criteria 2), and between group statistical comparisons were reported for at least one key outcome (criteria 10). The van Tulder scale scores showed the timing of outcome assessment was identical for all intervention groups for all important outcomes (criteria J), and high levels of allocation concealment (criteria B) and drop-out rate description (criteria I) were achieved throughout the studies (92%).
The most common methodological failings of the studies under the van Tulder rating were inadequate therapist (100%), subject (92%) and assessor (67%) blinding, and a lack of intention-to-treat analysis (58%). The PEDro scale showed a similar pattern with inadequate therapist (100%), subject (92%) and assessor (58%) blinding, and a lack of intention-to-treat analysis (50%) being commonly reported problems.
The PEDro values were compared to the online scores available and were found to fall within one point of each other. The quality rating of only one study would have changed from high to low quality if online scores were used.52 Upon further deliberation it was decided that the score for this study should remain at 6/10 as we felt the measurement of at least one key outcome was obtained from more than 85% of the subjects initially allocated to groups.
Outcome measures
Summary statistics for the included studies can be found in table 3. Comparisons between tendinopathies for the outcome measures of pain and satisfaction/return to activity are shown in figs 4 and 5.
Results of included studies for clinical outcome measures. Incomplete data were not included

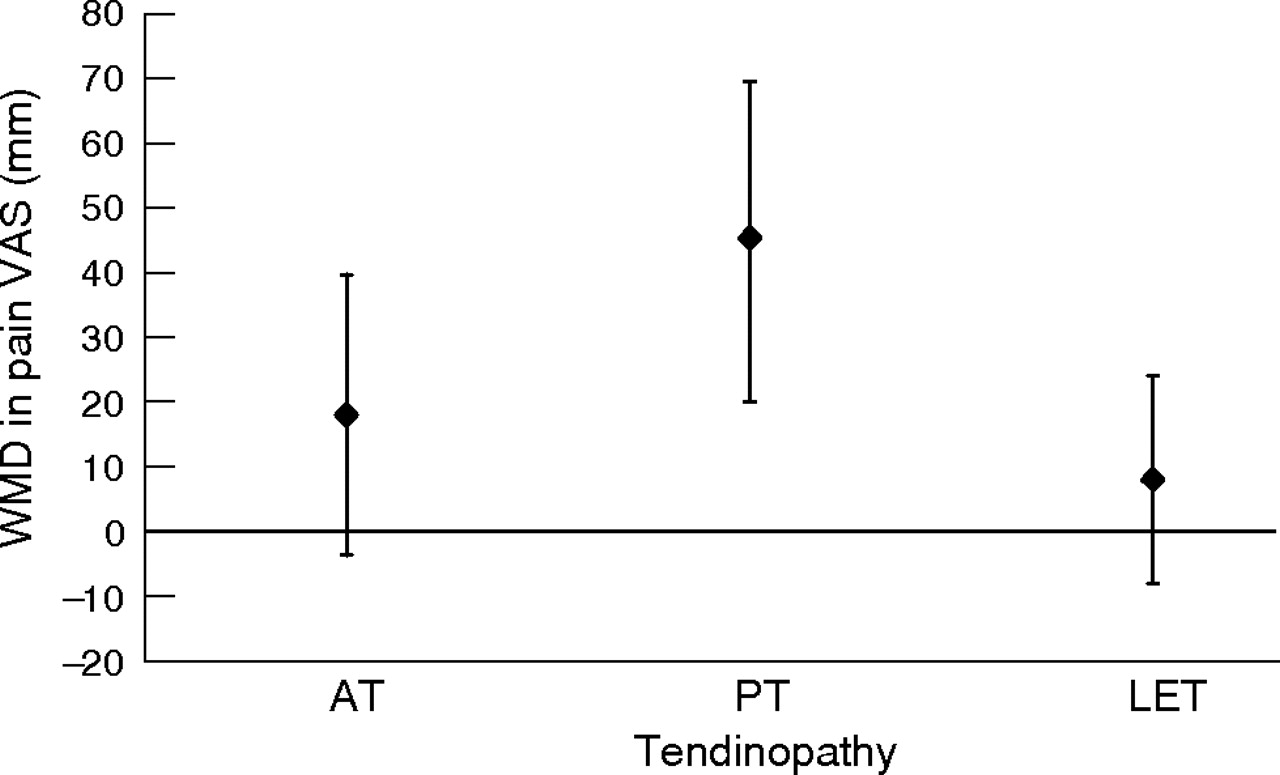
Summary of findings. Pain VAS changes in the treatment of three tendinopathies, EE compared to CE (WMD±95% CI are shown). AT, Achilles tendinopathy; CE, concentric exercise; CI, confidence interval; EE, eccentric exercise; LET, lateral elbow tendinopathy; mm, millimetres; PT, patellar tendinopathy; VAS, visual analogue scale; WMD, weighted mean difference.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
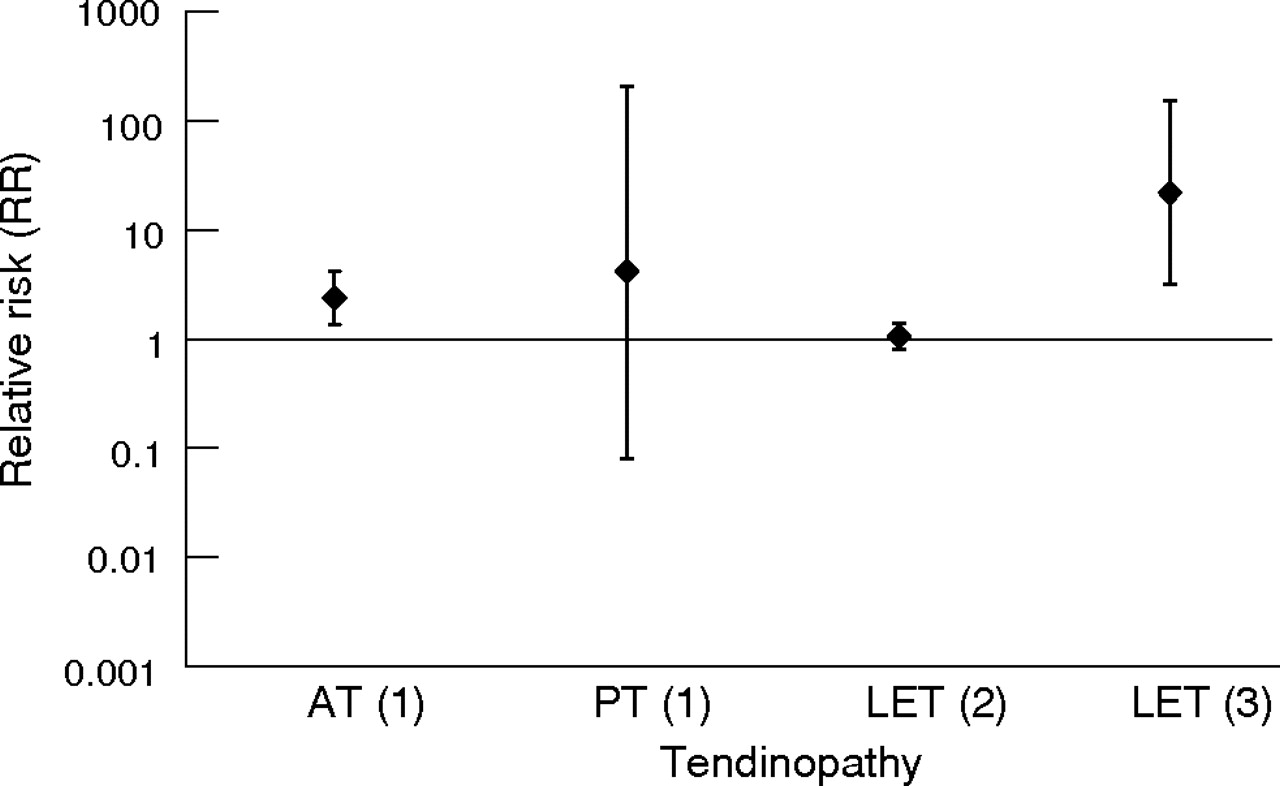
Summary of findings. RR of Satisfaction/Return to Activity in EE groups compared to controls (±95% CI): (1) eccentric vs concentric -12 weeks; (2) eccentric vs st. >6 months; (3) eccentric vs US >6 months. AT, Achilles tendinopathy; CI, confidence interval; EE, eccentric exercise; LET, lateral elbow tendinopathy; mm, millimetres; PT, patellar tendinopathy; RR, relative risk; st, stretching; US, ultrasound; VAS, visual analogue scale.
Pain
Only three studies using the pain VAS as an outcome measure were able to be included in data analysis;45,46,52 no pooling of data was achievable due to the low number of studies.
Silbernagel et al52 found an 18 mm (95% CI −3.68 to 39.68) difference in VAS favouring EE to CE intervention at the 12-week stage of rehabilitation in AT; however, this was not statistically significant (p = 0.10). In PT, Jonsson et al45 found a WMD of 44.8 mm (95% CI 20.09 to 69.51) between the eccentric and concentric exercise groups at 12 weeks. This result was statistically significant (p = 0.0004) but the study was found to be of low methodological quality. Martinez-Silvestrini et al46 studied three different interventions for LET: eccentric, concentric and stretching groups. The WMD for pain VAS comparing eccentric to concentric was 8.00 (95% CI −8.02, to 24.02), and for eccentric compared to a stretching group was −1.00 (95% CI −16.46 to 14.46). Overall, this study showed no statistically significant differences between EE and any comparison group. Stasinopoulos et al53 investigated PT and used a scale dividing subjects into two groups, either ‘much better/no pain’ or ‘worse/no change/slightly better’;53 they found a RR of 21 (95% CI 1.40 to 315.98) at 16 weeks comparing EE to ultrasound, and a RR of 5 (95% CI 1.45 to 17.27) at 16 weeks comparing EE to frictions. Although these results were statistically significant in favour of EE (p = 0.03 and 0.01 respectively), the pain scale had not been validated and the study was of low methodological quality. Roos et al50 used the FAOS69 pain sub-score to determine a change in pain in AT and found no statistically significant differences at 12 weeks comparing EE to a control group (WMD 1.40; 95% CI −19.16 to 21.96) or EE to a splint group (WMD 14.00; 95% CI −6.56 to 34.56).
In summary, only two of the 11 included studies, both investigating PT, reported statistically significant results using a validated outcome measure of pain.45,53 Due to the low methodological quality and heterogeneity of these two studies, only a limited level of evidence exists to suggest that EE is clinically effective in reducing pain in PT. Owing to small trial numbers and very large confidence intervals, there is no evidence available to suggest whether EE is effective in reducing pain in either AT or LET.
Function
Various measures of functional outcome were used to determine whether EE was effective in increasing function in tendinopathy, and due to this variation, pooling of data was not possible.
In AT, Roos et al50 reported function at 12 weeks using the FAOS subscale of sport and recreation. The study compared EE to a control group (WMD 17.00; 95% CI −8.87 to 42.87) and EE to a splint group (WMD 20.00; 95% CI −5.87 to 45.87); both of these differences were not statistically significant. Other outcomes, including plantarflexion range of motion (WMD 2.00; 95% CI −3.36 to 7.36), a jumping test (WMD 0.00; 95% CI −4.89 to 4.89), and a toe raise test (WMD −2.00; 95% CI, −14.55 to 10.55), also failed to show statistically significant differences between EE and comparison groups.52
Two studies examined function in PT using the VISA66,67 scale, a functional pain-rating scale specifically designed for AT and PT, and found quite different results.45,55 Jonsson et al45 showed that EE intervention increased VISA scores significantly compared to a CE programme (WMD 45.90; 95% CI 24.54 to 67.26); in contrast, Visnes et al55 found a WMD of 0.10 (95% CI −14.38 to 14.58) comparing EE to a control of normal training in elite volleyball players. Cannell et al57 also investigated PT, and measured hamstring and quadriceps moments as a functional outcome. No statistically significant difference was found between the two intervention groups for either hamstrings moment (WMD 5.00; 95% CI −133.98 to 143.98) (p = 0.94), or for quadriceps moment (WMD 106; 95% CI −73.74 to 285.74) (p = 0.25). Martinez-Silvestrini et al46 used the DASH68 functional outcome measure for LET and found no significant difference in function comparing EE to CE (WMD 0.00; 95% CI −9.76 to 9.76) (p = 1.00), and comparing EE to stretching (WMD −3.00; 95% CI −12.71 to 6.71) (p = 0.54). The same study also assessed grip strength as a functional measure, but again there were no statistically significant results. Selvanetti et al63 also studied the common extensor tendon origin to determine the effect of EE compared to ultrasound, and found a significant difference in Ko70 scores at 4 weeks (WMD 38.70; 95% CI 29.75 to 47.65; p<0.00001) and at 11 months (WMD 39.20; 95% CI 30.32 to 48.08; p<0.00001). This scale was taken from a previous study that investigated another type of treatment for LET, but had not been validated.70
No firm conclusions can be derived from these studies regarding the effect of EE on function due to the variety of outcome measurement used and the small number of available studies. The only two statistically significant results reported were either from a study of low quality,45 or were obtained using a non-validated functional outcome measure.63
Patient satisfaction/return to activity
Patient satisfaction/return to activity was significantly different for AT (p = 0.003) when 12-week data were pooled from two studies (RR 2.38; 95% CI 1.36 to 4.18).27,59 These studies, however, were both of low methodological quality. In contrast, a significant risk ratio in favour of EE was not found in a high-quality study measuring satisfaction after 12 months (RR 1.56; 95% CI 0.73 to 3.32) (p = 0.25).52 Pooling of data was completed for satisfaction/return to activity at the 12-week stage of rehabilitation in PT for EE compared to CE (RR 4.17; 95% CI 0.08 to 206.41).45,57 This result was more pronounced and statistically significant at a follow-up point of 32.6 months (mean) in another study (RR 17.27; 95% CI 1.15 to 260.07; p = 0.04), although this was of low quality.45 In LET, satisfaction/return to activity for EE intervention compared to ultrasound was statistically significant at six months post-treatment (RR 21.97; 95% CI 3.17 to 152.20; p = 0.002),63 whereas the RR for EE compared to stretching at the same time point was 1.06 (95% CI 0.81 to 1.39).54
In summary, moderate evidence exists to suggest satisfaction/return to activity is more likely with 12 weeks of EE therapy compared to CE intervention in AT, but this is based on small study numbers. There is also moderate evidence to suggest that EE therapy is associated with increased satisfaction/return to activity at six months post-treatment in LET when compared to ultrasound therapy. Only limited evidence exists to support the effectiveness of EE on satisfaction/return to activity in PT.
DISCUSSION
This systematic review was undertaken with the aim of determining the effectiveness of EE in the treatment of various common tendinopathies. Eleven RCTs met the inclusion criteria; they included studies of AT, PT and LET. RCTs investigating the effect of EE on rotator cuff tendinopathy were not found using the defined search strategy. Since the time of data analysis, a small non-randomised pilot study has been published investigating rotator cuff tendinopathy and the effect of EE therapy; however, it would not have satisfied the inclusion criteria used here, and would not, therefore, have affected the results of this review.71
Due to the lack of high-quality studies with clinically significant results, no strong conclusions could be made regarding the effectiveness of EE (compared to control interventions) in relieving pain, improving function or achieving patient satisfaction. A limited level of evidence exists suggesting EE reduces pain in PT at the 12-week stage of treatment when compared to CE. There is also limited evidence suggestive of an increase in function using EE compared to ultrasound in the treatment of LET, although the validity of the outcome measure used in this study is unclear.63 Patient satisfaction/return to activity results were more positive for EE, with moderate evidence suggesting EE intervention may increase patient satisfaction/return to activity compared to CE in AT, as well as to support EE compared to ultrasound in LET; limited evidence exists supporting EE compared to CE in PT. Another systematic review known to have investigated the effect of different physical interventions in the treatment of LET came to similar conclusions regarding the effectiveness of exercise therapy.72 This group found insufficient evidence to determine the effectiveness of exercise therapy in the treatment of LET but concluded that results from preliminary studies warranted further evaluation in this area. Other systematic reviews investigating exercise therapy in PT or AT were not found.
Overall, the methodological quality was considered high in only six studies of the 11 included in this review. It was assumed that the risk of misclassification was low, as reliable and valid measures of methodological quality were used.39,41 The most common deficits in methodology were the lack of blinding of subjects, assessors and therapists. The blinding of subjects and therapists will always remain difficult when implementing exercise therapy interventions in research.73 Liddle et al (2004) omitted the van Tulder item of ‘blinding of care provider’ in a systematic review of exercise and chronic low back pain as they felt the item was inapplicable to exercise interventions. If this item was deleted in both methodological scores used in this review, quality ratings of all included studies would not have changed.
Treatment effects are found to be overestimated in low-quality systematic reviews where non-randomised studies such as prospective cohorts are included.74,75 This may be due to non-randomisation and inadequate allocation concealment methods contained within these prospective studies.74 For this reason, prospective, non-randomised studies were not included in this systematic review. However, many non-randomised trials have been undertaken to investigate the effectiveness of EE in common tendinopathies.25,26,47,48,64,76,77 One non-randomised prospective study investigating AT compared EE to a surgical intervention and found a larger, significant treatment effect on pain VAS than reported here (WMD 25.8; 95% CI 11.36 to 40.24).25 This result should be viewed with caution due to the low methodological quality of the study concerned.
Findings from this review are limited by the fact that included trials were based upon small sample sizes, and these numbers were often too small to reach adequate statistical power. Heterogeneity of the studies included in the review was considered another problem, with differences in study population, interventions, controls and outcome measures. Only a few studies reported similar outcomes, making the pooling of data impossible for the majority of outcome measures. The lack of long-term follow-up in research in this area is also an issue, as only three studies included a one-year outcome measurement.50,52,54 This makes any potential longer-term clinical benefit of EE hard to determine.
The treatment regime most commonly used in the included studies was derived from an initial study of AT.25 This comprised three sets of 15 repetitions, done twice daily, seven days a week for 12 weeks. Upon correspondence with one of the authors of this study, it was found that the regime was based on clinical experience, rather than derived from any empirical evidence; e.g. data from ‘dose response’-type studies. However, the lack of understanding about the basic pathophysiology of tendinopathy makes determining the optimal dosage of intervention difficult. A recent review of EE in AT tried to address the issue of treatment dosage21 and concluded that because the studies in this area have not used an underlying rationale to determine loading parameters, progressions and frequency of treatment, further research needs to be undertaken before an optimal dosage can be determined.
In summary, there is a dearth of high-quality research available to establish the effectiveness of EE therapy in the treatment of three common tendinopathies. Due to low sample numbers, large confidence intervals were present in many studies, making the majority of results inconclusive. Limited to moderate levels of evidence exist in a number of areas, thus warranting further research in this field. Although clinical benefits of EE could not be fully determined due to the lack of quality research with adequate follow-up, the overall trend suggested a positive effect of EE, with no study reporting adverse effects. However, a recent study suggests that sedentary subjects with AT may show less promising results with EE therapy compared to athletic subjects.78 Further determination of variations between population sub-groups such as these will also require high-quality RCTs to be undertaken before any firm conclusions can be made.
Randomised controlled trials are commonly accepted as the ‘gold standard’ way to investigate the effectiveness of a particular healthcare intervention.79 Thus, further RCTs in this area must be adequately powered and include appropriate randomisation procedures, standardised outcome measures and long-term follow-up. As a precursor to this, RCTs should be undertaken to determine the ‘dose-response’ effect of various EE programme durations and intensities. It is only then that the clinical benefit of EE in the treatment of tendinopathy may be fully elucidated compared to other treatment modalities. While clinicians may opt to continue to utilise EE programmes in the treatment of common tendinopathies, they should be aware of the lack of evidence for the superior effectiveness of this approach in comparison with other active modalities such as concentric exercise and stretching.
What is already known on this topic
-
Tendinopathy is a non-inflammatory degenerative condition that may take 6–12 months to resolve with conservative intervention.
-
The pathogenesis of tendinopathy remains unclear.
-
EE programmes have been emphasised in recent literature as a key part of tendinopathy rehabilitation.
What this study adds
-
There is a lack of evidence supporting the effectiveness of EE programmes over other active modalities such as CE and stretching.
-
Further adequately powered RCTs with standardised outcome measures and long-term follow-up are required to ascertain the clinical benefits of EE programmes in the treatment of tendinopathy.
Acknowledgments
Dr Melanie Bell from the Department of Preventative and Social Medicine, University of Otago, Dunedin, New Zealand for statistical support, and the administration staff at the School of Physiotherapy, University of Otago, Dunedin, New Zealand.
REFERENCES
COMMENTARY 1
Treatment of tendinopathy is an important clinical issue, and treatment modalities have been long discussed. Working our way away from surgical intervention, training intervention with eccentric exercise has been a magic phrase based on some very early studies. With this review it is easier to understand where we are regarding the evidence for this treatment.
COMMENTARY 2
Chronic tendinopathy is a challenging condition. Recently, there has been considerable interest in using eccentric training to treat these conditions. Unfortunately, the studies examining the effects of eccentric training have been varied in terms of methodology and protocol, making the evidence difficult to interpret. This review critically examines the available research. Unfortunately, there remains a paucity of high-quality evidence surrounding eccentric training and tendinopathy. The authors are able to make some weak conclusions about the efficacy of eccentric training, but they reasonably conclude that more studies using better randomisation, larger sample sizes and more standardised outcome measures are necessary before stronger conclusions can be made.
Footnotes
-
Published Online First 24 October 2006
-
Competing interests: None identified.