Article Text

Statistics from Altmetric.com
Most youth sports around the world are classified on the basis of chronological age to guarantee equal chances within each of the different age groups. At the elite level, international sporting federations organise competitions in various age classes ranging from as low as under-13 up to under-21, depending on the sport. In August 2010, the International Olympic Committee (IOC) is conducting the first Youth Olympic Games in Singapore for 14–18-year-old athletes.
The standing of these youth competitions has increased to the stage at which there may be considerable rewards, individual fame or national prestige associated with winning, not only for the athlete but for the coach and his or her entourage. These competitions also represent important showgrounds for young athletes; in some sports, this is often where talented athletes are identified for a future professional career.
Unfortunately, in a number of sports it is suspected that the chronological age of the participating players is higher than the age stated on the official documents used to determine the eligibility of the individual. Players with a greater relative age are more likely to be identified as talented because of the likely physical advantages they have over their ‘younger’ peers.1
International sporting federations have uncovered several cases of document fraud, presumably aimed at allowing over-age athletes to gain a performance advantage by competing in a lower age class. At the other end of the spectrum, there are also documented cases of under-aged athletes competing in events in which there is a lower age limit (eg, the age of 14 years in the Olympic Games); particularly in sports in which late maturers may be at an advantage, such as in gymnastics.
It should be noted that the participation of over-age or under-age athletes is not always due to intentional cheating. To verify age, sports governing bodies rely on documentation such as birth certificates, documentation of hospital deliveries, passports, national IDs, school certificates and police documents among others. Although these documents are accurate in most countries (except for deliberate falsifications), their validity may be questionable in others. Some countries register births late for geographical, cultural or other reasons, sometimes not until school start. It is also important to note that the home country of a team cannot necessarily guarantee the accuracy of birth certificates, as many teams, particularly from Europe, field players originating from developing countries in Africa, Asia and South and Central America. In these cases, birth certificates and other documents require the same careful investigation as for teams originating in these countries. Reliance on birth certificates or other official documents is thus not always possible, and alternative, reliable methods for age determination are sought.
To a large extent, the performance of adolescent athletes is determined by their physical maturity and is thus related to age. However, although age is a linear factor, growth and maturation are not.2 The onset and rate of growth and maturation varies widely between individuals during adolescence, and consequently the maturational status of children of the same age also differs.3,–,5 Therefore using physical signs of maturity or skeletal age to determine chronological age may be difficult.
Whereas age discrepancies are against the spirit of sports and undermine the principles of fair play, the participation of over-aged or under-aged athletes in competition also raises other concerns. Prime among these is a concern of the risk of injury to the athlete, or to his or her opponents.6 7 Allowing over-age, more mature athletes to compete among younger athletes may cause an increased risk of injuries to their opponents, especially in contact or collision sports such as the various football codes and team handball.8 It is also conceivable that allowing under-age athletes to compete may subject them to loads and risks that are thought to be inappropriate for their age, not only physically, but in terms of the psychological and social development of the child.
The IOC and international sports governing bodies acknowledge a mandated duty of care to protect the physical and psychological health and safety of all athletes including elite adolescent athletes.9 10 As such, the development and use of appropriate methods for determining age is not only necessary to ensure a level playing field, but also to protect the health and safety of the adolescent athlete.
Ideally, a reliable solution to determine age should be applicable across all sports, all age levels should be accommodated in one policy (12–21 years) and the solution should identify over-age as well as under-age athletes equally well. The goal of this paper is to determine whether methods to determine chronological age are available.
To address these issues, the IOC assembled an expert group in December 2009 to review the current state of age determination in athletes, aiming to provide recommendations for sports governing bodies, as well as to outline the need for further research. The group considered the following issues regarding age determination: (1) youth sports performance—creating a level of playing field; (2) health and safety of the elite adolescent athlete; (3) pubertal status and skeletal age; (4) use of x-ray examinations in age determination; (5) use of radiation-free methods in age determination; (6) future directions.
Youth sports performance: creating a level playing field
Many aspects of youth sports performance improve with biological maturity. Changes in physiological parameters including strength and aerobic and anaerobic power appear to mirror biological age more closely than chronological age, with peak increases occurring at or around the time of the adolescent growth spurt.11,–,15
It has long been observed that there is a preponderance of early and on-time maturers in elite adolescent sports such as football, tennis and swimming, in which greater strength, power and speed give athletes a competitive advantage.2 6 16 17 In other sports, such as gymnastics and diving, however, short stature and leanness favour relative immaturity which probably accounts for the preponderance of late maturers in these sports.17 18
Longitudinal studies in boys demonstrate a pubertal spurt in aerobic power (peak oxygen consumption) and strength around the time of peak height velocity (PHV) and peak weight velocity.11 13 19 Increases in physical fitness and strength appear to be largely related to changes in body size, including body mass, stature and lean tissue mass.15 In girls there appears to be a more linear increase in aerobic and anaerobic power and strength with age, but the lack of longitudinal studies in girls makes it difficult to determine whether or not they have a similar growth spurt to boys in these parameters, coincident with puberty.
Aerobic power increases with age and maturation in both genders, but plateaus earlier in girls than in boys. When expressed relative to body weight, however, (ml/kg per min) aerobic power is relatively stable in boys and declines in girls from childhood to adolescence.20,–,22
When allometric modelling is used to control for the non-linear effects of body size, boys and girls experience an increase in aerobic power that extends from the prepubertal years until adulthood in boys and from prepuberty to puberty in girls.23
Anaerobic power also increases with age and maturity, but the existing literature does not allow us to determine conclusively whether maturation affects the development of anaerobic power independent of its effects on body size and composition.14 Anaerobic power in boys (and probably girls) continues to increase after adolescence. This may explain the improvement in sports performance that occurs after adolescence in sports reflecting anaerobic power, that is, in short high intensity performances.14 The reasons for the improvement in anaerobic performance observed beyond adolescence have not been identified, but may be related to improvements in neuromuscular control and muscle glycolytic capabilities.24 25
Marked increases in strength occur in both genders at puberty coincident with peak weight velocity.19 Before puberty there is little gender difference in strength. At puberty, the difference in strength (particularly upper body strength) between boys and girls becomes more pronounced, with these differences being reduced, but not eliminated, when strength is expressed relative to lean tissue mass. Increases in isokinetic strength that occur with maturation are not significant when changes in body mass and height are taken into account.26
The difficulty with interpreting studies examining the effects of age and maturation on physiological parameters of sports performance is in eliminating the contribution of changes in body size and composition that occur concurrently. A number of different scaling methods has been used in various studies in an attempt to achieve this aim. Ratio scaling (expressing variable relative to body mass) is still the most commonly used method in the literature, although it has significant limitations, namely assuming that the relationship between the performance variable and body mass is a linear one. Alternative approaches including allometric scaling have been used in an attempt to examine the relationship between body size and the measured variable. Allometric exponents for peak oxygen consumption vary for body weight and height in early, on-time and late maturing boys.27
A review of ultrasound record youth track and field performances in both ‘anaerobic’ (100 m) and ‘aerobic’ (1500 m) events highlight the difficulty of establishing a level playing field in youth competition. In both boys and girls, sports performance improves with age, reflecting the advantage that an over-age athlete may have when competing against younger opponents.28 29
Figures 1 and 2 demonstrate ultrasound record performance results for boys and girls in track events (100 m and 1500 m).28 29
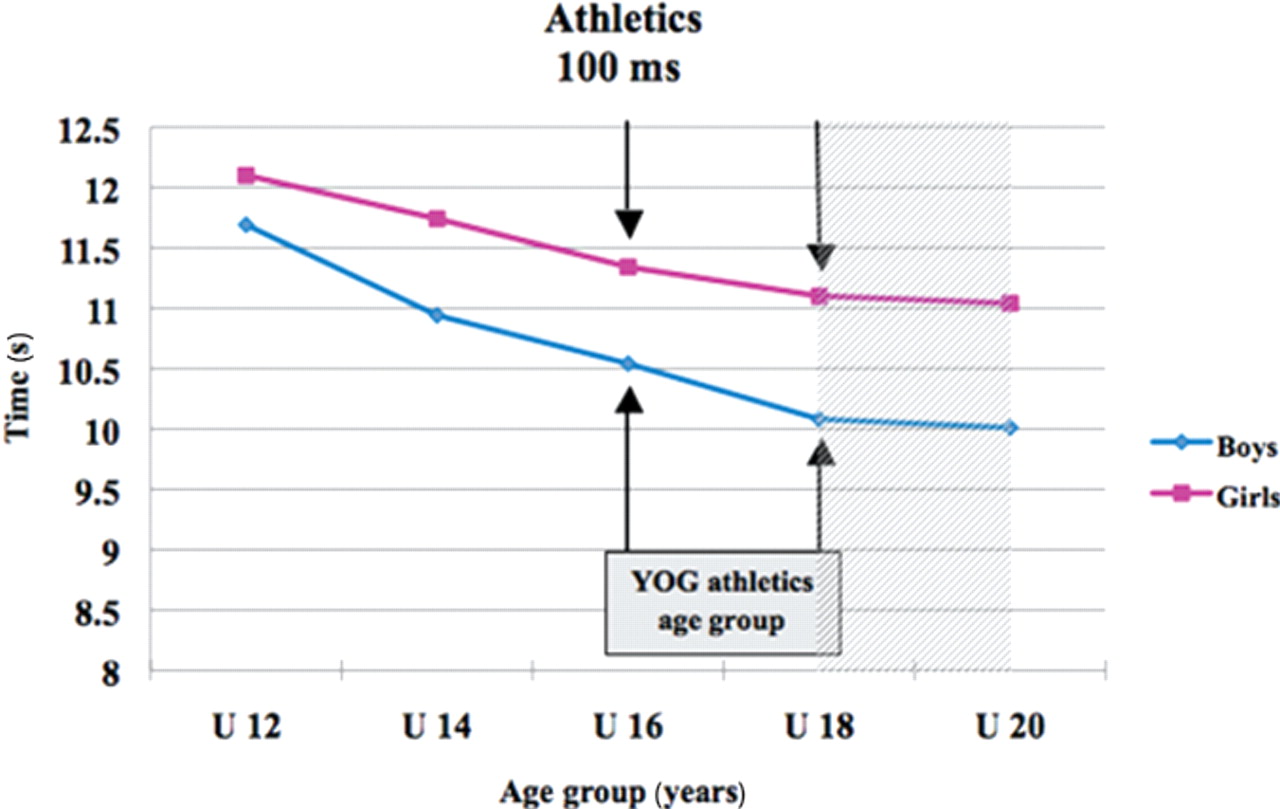
USA record youth performances in 100 m sprint.28

USA record youth performances in 1500 m.29
Growth and maturation are not linear factors; nor is the development of physical performance. The onset and rate of growth and maturation varies widely between individuals during adolescence, which explains why children of the same chronological age often differ markedly in body size and physiological capabilities and consequently in performance.
Health and safety of the elite adolescent athlete
The perception of experienced clinicians and an understanding of the unique physical and biomechanical characteristics of the adolescent athlete gives rise to significant concerns regarding the risk of injury when a discrepancy in chronological age or degree of maturation exists.8 Further concern arises when the potential for mismatch is magnified by the presence of over-age or under-age competitors. Despite a paucity of evidence for an increased risk of injury associated with discrepancies of age or maturation, the concern for the adolescent athlete's health has been great enough to move some sporting bodies to introduce weight for age classification in some junior contact sports, such as wrestling, American football and rugby union,30 31 and height for age classification for some junior gymnastics events in an attempt to reduce injury risk.10
There are a number of factors unique to the adolescent athlete during the period of growth and maturation that have the potential to increase injury risk.
Changes in the mechanical properties of cartilage and bone associated with growth and maturation make the young athlete more vulnerable to injury.32 33 Growth cartilage is known to be thicker and more fragile during adolescence and this may increase the risk of epiphysial and apophysial injury.32 34–36 Immature articular cartilage is thought to be relatively weaker and more susceptible to compressive forces.37 Finally, total bone mineral density decreases at the time of peak linear growth,38 with a known association between the peak fracture rate and the adolescent growth spurt.33
As well as changes to cartilage and bone with growth and maturation, changes in muscle mass and flexibility may also influence injury risk. The peak increase in lean tissue mass is known to precede decreases in bone mineral density,39 giving rise to a situation in which an increasingly stronger muscle is pulling against a relatively weaker bone. Reduced flexibility has also been considered a risk factor for injury during adolescence. It remains unclear, however, if flexibility is actually influenced by growth. Phillaeparts et al12 found that changes in flexibility were reduced at the time of PHV and peaked 12 months following PHV, whereas Feldman et al40 found that growth did not appear to be a cause of decreased flexibility during the peripubescent period.
The time of relative weakness of both bone and growth plate also corresponds to the time when increases in the torque are required to maintain a joint in a given position or move it through range. These changes are related to relative increases in limb length and mass with growth and maturation, which result in greater moments of inertia around any given joint. These biomechanical changes are also thought to be reflected in functional activities, with Hawkins and Metheny41 estimating that following the adolescent growth spurt a 30% increase in force is required to produce the same degree of acceleration during a kicking motion.
Both chronological age and maturity appear to have some influences on the incidence of injury in the adolescent athlete. Numerous studies across different sports have shown that injury incidence increases with chronological age.42,–,46
The evidence for the influence of biological maturity on injury risk is somewhat conflicting. Whereas a number studies demonstrate a higher incidence of injury with increased maturity,47,–,49 other studies have found either an increased risk of injury in less mature athletes,50 or no effect of maturation on overall injury incidence6 51 (table 1).
Effect of maturity status on injury risk
Pure injury incidence data, however, do not fully portray the potential threat to the under-age or immature athlete. Mismatches in biological maturity, assessed as the difference between chronological age and skeletal age, in young elite male football players are associated with a higher incidence of major injuries in biologically less mature individuals.6 In a study on elite male youth footballers, players younger than 14 years incurred more injuries in training and sustained more growth-related overuse injuries than older players.44 More recently, maturity status, playing and training time of male young elite football players assigned to a youth sports academy collectively explained 48% of the variation in injury rates.7
With these studies in mind, the concern for clinicians is that during a period of known skeletal vulnerability, the adolescent athlete may be exposed to excessive training and competition loads associated with high-level competition, which places the athlete at greater risk of injury. The potential involvement of under or over-age athletes in these competitions magnifies this fear.
Pubertal status and skeletal age
Puberty is the defining process in the transition from childhood to adulthood. As such, assessment of pubertal status and the influence of pubertal progression through the early teenage years is an integral part of the determination of physical maturity and fitness.
The influences on the timing of puberty are varied and many remain unknown. Delays in pubertal development may be related to constitutional (genetic) causes, nutritional status, energy expenditure, or more significant pathology. Precocious puberty may also be due to genetic predisposition, endogenous androgen or oestrogen excess or deliberate or accidental steroid hormone exposure.52
In sport, normal variations in the timing and progression of puberty can influence performance. Developmental variations may also complicate the issues of determining appropriate participation in age-determined sporting events. The normal age range for the beginning of the adolescent growth spurt in boys can range from 10.5 to 16.0 years, with completion of growth between 13.5 and 17.5 years chronological age. Similarly, for girls, the age of onset of the adolescent growth spurt can range from 9.5 years to 14.5 years and still be considered within the normal range (figure 3).53

Range and progression of pubertal development.53
The age range of onset of pubertal development is wide for both boys and girls. For girls, entrance into puberty is defined as the start of breast development, Tanner stage 2, reflecting oestrogen production (figure 4). This typically occurs between the ages of 8 and 13 years. An increase in longitudinal growth rate occurs in the early stages of pubertal development, with the peak rate of growth reached at Tanner stage 3 on average. This adolescent growth spurt is relatively short in girls, lasting approximately 1.5 years before declining below the prepubertal rate and progressing slowly to cessation of growth.54 Progression of growth to menarche typically takes on average 2.4 (SD 1.1) years, at which point the majority of longitudinal growth has been achieved.55

Tanner staging for breast development in girls (adapted from an image created by Michał Komorniczak, used under the Creative Commons Attribution—Share Alike 3.0 Unported licence).
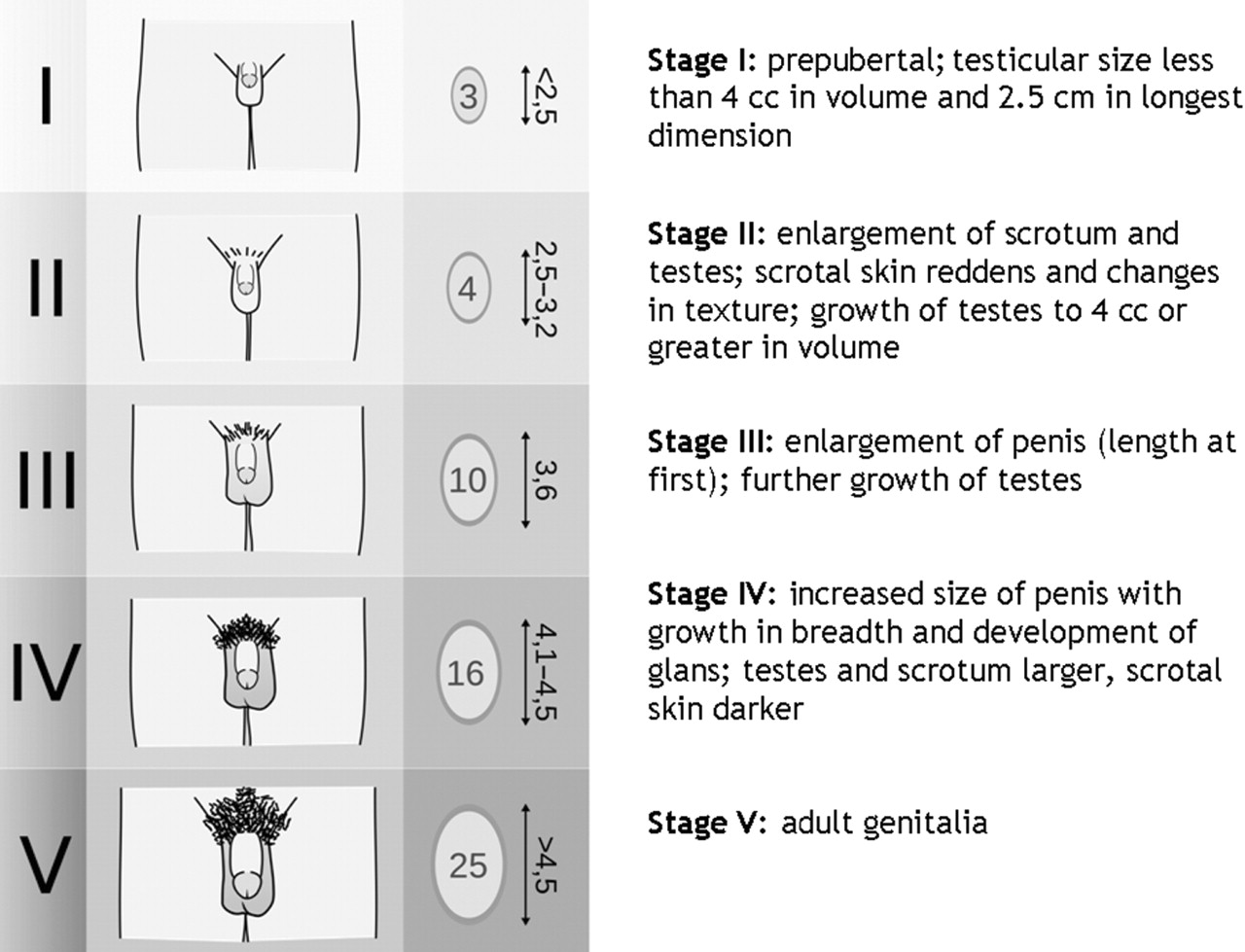
In boys, enlargement of the testes to greater than or equal to 4 cm3 represents the start of pubertal development and typically occurs between the ages of 9 and 14 years (figure 5). The longitudinal growth rate increases later in boys with the peak at Tanner stage 4–5 and with a longer duration than in girls, lasting approximately 3 years before quickly declining.54 The apex of increase in muscular strength typically occurs as growth velocity is declining. A period of 3.2 (SD 1.8) years is necessary to reach adult testicular volume.55

Tanner staging for genital development in boys (adapted from an image created by Michał Komorniczak, used under the Creative Commons Attribution—Share Alike 3.0 Unported licence).
Ethnic differences in the age of onset of puberty have been noted in both girls and boys.56 57 These differences add to the overall variation in pubertal timing when looking at large groups of mixed ethnic background. There may also be differences in the pace of progression of puberty in different ethnic groups, although these studies have not yet been performed.
Assessment of skeletal age is frequently used in the evaluation of growth and puberty in children in the adolescent age range. In children with conditions associated with delays or acceleration of pubertal development, the magnitude of skeletal advancement or delay generally matches the magnitude of pubertal advancement or delay.58 However, when evaluating children whose pubertal development falls within the normal range, the variability in bone age at onset of puberty was not less than the variability in chronological age and there was no clear association between skeletal age and the onset of pubertal development.59 60
Growth charts evaluating longitudinal growth patterns are commonly used in the assessment of growth and pubertal development (figures 6 and 7). These are illustrative of the variations in the timing of the pubertal growth spurt in both boys and girls, indicating different patterns of growth and the chronological age of attainment of final adult height within 2 SD above or below the mean. Whereas closure of the epiphyses and final adult height is achieved at a skeletal age of 17 years by the standards of Greulich and Pyle,61 there is no clear correspondence with chronological age due to the variability in pubertal development and sex steroid exposure. Children who reach physical maturity early may have a skeletal age that is several years advanced from their chronological age, with comparable delays seen in those with late maturation.

Longitudinal growth charts for girls (Bayer and Bayley 1959).54
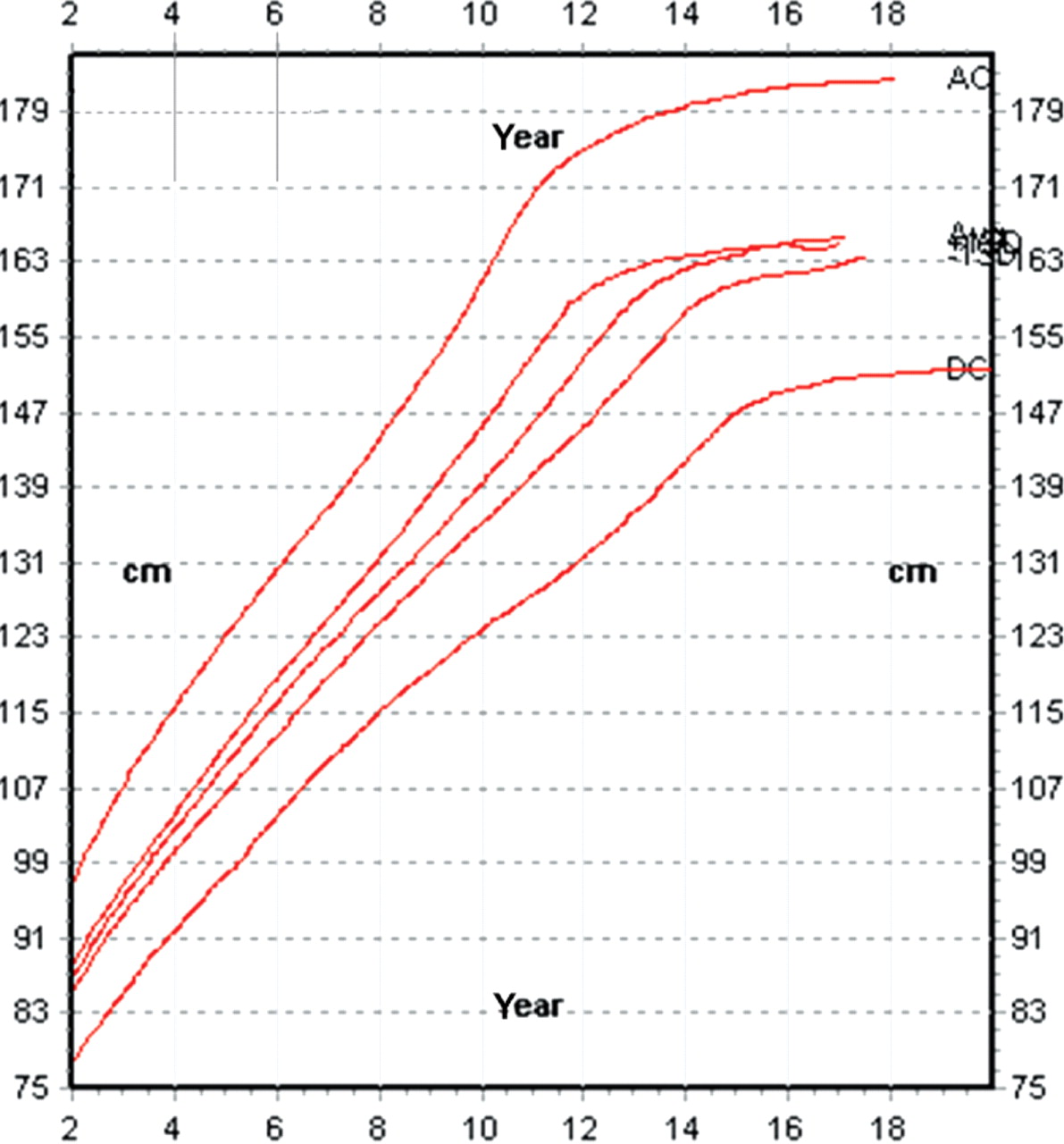
Longitudinal growth charts for boys (Bayer and Bayley 1959).54
In addition to the increases in testosterone and oestrogen levels that define the process and increase progressively throughout pubertal development, other hormonal factors also increase during this period. Insulin-like growth factor 1, insulin-like growth factor binding protein 3, dihydroepiandrostenedione and dihydroepiandrostenedione sulphate all rise with increasing age, and reference ranges for these hormones are noted as age dependent.62 It would be tempting to use these factors as a determinant of chronological age, but increases in these factors are not truly age dependent, but rather dependent on pubertal status. Increases in insulin-like growth factor 1 and insulin-like growth factor binding protein 3 are dependent on the rise in growth hormone, which itself is dependent on increases in testosterone during puberty. Dihydroepiandrostenedione and dihydroepiandrostenedione sulphate levels increase with maturation of the adrenal gland, which also has a great deal of variability in chronological timing. As a result, in clinical practice, these levels are interpreted not in terms of chronological age, but in terms of pubertal status and skeletal age. They are, therefore, no more useful than skeletal age for the determination of chronological age.
The fact is that the variability in skeletal age at the onset of puberty compounded by the wide variation in the timing of pubertal development makes the assessment of skeletal age useful for purposes of diagnosis and treatment, but less useful for the determination of chronological age.
Use of x-ray in age determination
Skeletal age is said to be the most accurate method of assessing biological maturity.63 The determination of skeletal maturity is important in a number of clinical conditions in the child. These include anisomelia, whether genetic or acquired, scoliosis, surgical interventions about the knee and hormonal conditions that affect maturation.64,–,69
At the end of each bone there is an ossification centre (epiphysis) with an adherent growth plate (physis) perpendicular to the long axis of the bone. The cartilage cells of the physis multiply and transform with mineralisation and new bone is produced, which contributes to diaphysial growth.
At the end of skeletal maturity the epihysis will fuse to the rest of the bone and the physis disappears. The timing of epiphysial ossification and fusion of bones does not happen synchronistically across the body. In some bones ossification starts directly after birth, in other bones between 14 and 17 years of age. The time period for epiphysial fusion and closure of the physis also varies; between 10 and 25 years of age, and girls are approximately 2 years earlier in their skeletal maturation than boys.2 70
The three most frequently used methods to assess skeletal maturity are the Greulich–Pyle,61 the Tanner–Whitehouse53 71 72 and the Fels method;73 all based on radiographs of the left hand and the wrist.
The left elbow (Sauvegrain method) has also recently been used to assess skeletal age, with a good resolution around the prepubertal period.74 75 However, the use of left hand x-rays61 72 still remains the gold standard for the determination of skeletal age (bone age) in the process of assessment of biological maturation.
Probably the most widely used method of determining bone age employs the Greulich–Pyle atlas of skeletal maturation, introduced in 1950.61 The atlas consists of radiographic images of the average skeletal appearance of the left hand and wrist of boys and girls, aged 8–18 years, which serve as reference images to determine the relative bone age of children in each age group.
A more detailed radiographic method was published in 1962 by Tanner, Whitehouse and Healy (TW1),53 and revised versions were introduced in 1975 and 1983 as TW271 and in 2001 as TW3.72 Relative maturity scores are assigned to the radius, ulna, carpal bones and phalanges and a composite score is used to determine skeletal age.
The Fels method is the third method used to assess skeletal maturity.73 It is based on a sample of north American children followed in the Fels longitudinal study. As with the previous two methods, a radiograph of the left hand and wrist is used. The subject child's radiograph is then scored using both relative maturation levels and measured ratios of epiphysial and diaphysial diameters of the appropriate bones of the hand and the wrist. The resultant scores are then entered into a computer program, which calculates the skeletal age.
Radiographic assessments are influenced by ethnic variations and living conditions (nutrition, diseases). The Greulich–Pyle method derives from examinations of 1000 upper-middle class children born in the 1930s and living in Cleveland, Ohio.61 The TW2 method is based on 2700 British lower and middle class children born in the 1950s and early 1960s.71 The Greulich–Pyle children matured more rapidly compared to the TW2 children, giving a difference of 9 months from the age of 6 years.
In order to compensate for ethnic variations, the TW3 reference population was updated and based on children from Great Britain, Belgium, Italy, Spain, Argentina, USA (Texas) and Japan. Since then, TW2 and TW3 have been tested in several countries and on different samples. In a Brazilian study by Ortega et al,76 the range of mean difference between skeletal age and chronological age with the TW3 method of different age groups was −0.7–0.3 in boys and −0.4–0.8 in girls, and with the TW2 method −0.7–1.4 in boys and 0.6–1.9 in girls. The difference between TW2 and TW3 in the adolescent children was more than 1 year. Another Brazilian study by Haiter-Neto et al77 confirmed these results. The authors found a good correlation between TW3 and chronological age, and also between Greulich–Pyle and chronological age. The figures in a German study by Schmidt et al78 for forensic age diagnostics (48 boys and 44 girls, 12–16 years of age) showed a range of difference of mean values between skeletal age and chronological age for the TW3 method of −0.4–0.2 years, compared with −0.1–1.4 years for TW2. In a Chinese study by Zhang et al79 of more than 17 000 children, the corresponding figures for TW3 minus chronological age were 1.0–1.3 years in Chinese boys in early adolescence and 0.2–1.0 years in girls. The Greulich–Pyle and TW3 methods were evaluated in a Turkish study by Büken et al80 (333 healthy children, 11–16 years of age). The difference between Greulich–Pyle and chronological age was −0.7–0.9 years in boys and 0.4–1.1 years in girls. The figures for TW3 were −0.4–0.1 years in boys and −0.6 to −0.1 years in girls, respectively (table 2).
Evaluation of the Greulich–Pyle and the Tanner–Whitehouse methods
Finally, there are studies evaluating the use of TW3 in young elite athletes. Malina et al81 studied the skeletal maturation in a group of Portuguese male elite football (soccer) players aged 12–16 years. The authors found that the players were, on average, advanced in skeletal maturation relative to chronological age. The conclusion was that football systematically favours early maturing participants.
A similar result was also found in an examination of 263 swimmers (178 boys and 85 girls, 12–14 years of age) using the TW2 method, in which the boys had a mean chronological age of 12.8 years compared with a bone age of 14.2 years. The figures for the girls were 12.7 and 13.5 years, respectively.82 A different pattern was seen by Claessens et al83 in adolescent elite female gymnasts. In some groups, for example adolescents 17 years of age, the chronological age was up to 3 years higher than the bone age measured by the TW2 method.
The major advantage of these methods based upon radiographs of the hand and the wrist is that they require a minimal amount of time and have demonstrated sufficient reproducibility in the setting of age determination. The disadvantage is that they entail the use of ionising radiation. Even if the ionising radiation dose with a left hand radiograph has been shown to be very small (radiation exposure of 0.00017 mSV) and almost negligible, corresponding to 1 h of background radiation from most major cities in the UK,84 85 ethical committees in many countries will not endorse the use of x-rays for the purpose of age determination in healthy children and adolescents.
Another limitation of using x-rays in the assessment of chronological age is the observed variation in skeletal maturity of 2 years within each gender. There may thus be a difference between the most skeletally immature boy and the most skeletally mature girl of 4 years in chronological age when skeletal growth is completed.7 16 As girls will complete their growth approximately 2 years earlier than boys, the upper limits for the assessment of skeletal maturity in boys and girls are 18 and 16 years of age, respectively.
As the radiograph images most used in the assessment of bone age are mainly based on children from Cleveland, Ohio, during the period 1931–42 (all white, European descents, relatively high socioeconomic class), it remains unknown if these data are representative of today's children in various populations.
Although skeletal age is said to be the most accurate method of assessing biological maturity, the assessment of skeletal age by x-ray scanning is limited and does not allow a precise determination of the chronological age. Variations up to several years in bone age have been observed in adolescents of the same chronological age.
Use of radiation-free methods in age determination
Use of MRI in age determination
The clinical use of MRI in the assessment of growth plate maturity is currently limited. There are a some preliminary studies using MRI for the assessment of (1) the extension of the growth plate;86 (2) specific closure patterns of the normal physis around joints87 and (3) physial arrest;88 however, none of these methods is widely used at present.
MRI assessment of the growth plate for age determination has been investigated by the Fédération Internationale de Football de Football Association—Medical Assessment Research Center (F-MARC).89 In an international under-17 (U17) football tournament, MRI was used to estimate the age of healthy adolescent football players, based on the degree of fusion of the left distal radial physis. The rationale behind this study was the requirement for a non-invasive technique, free of radiation risk, to ascertain the accuracy of the declared or documented age of adolescent players in football tournaments. A grading scheme of six different grades for epiphysial fusion was introduced upon analysis of the normal population: (I) completely unfused; (II) early fusion, minimal hyperintensity within physis; (III) trabecular fusion of less than 50% of radial cross-sectional area; (IV) trabecular fusion of more than 50% of radial cross-sectional area; (V) residual physis less than 5 mm on any one section; (VI) completely fused (figure 8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
MRI grading scheme after Dvorak et al90 using a T1-weighted SE sequence: (I) completely unfused; (II) early fusion, minimal hyperintensity within physis; (III) trabecular fusion of less than 50% of radial cross-sectional area; (IV) trabecular fusion of more than 50% of radial cross-sectional area; (V) residual physis less than 5 mm on any one section; (VI) completely fused.
A total of 496 healthy male adolescent football players between the ages of 14 and 19 years from different ethnic groups, geographical regions and altitudes (Switzerland, Malaysia, Algeria and Argentina) was selected.90 The selection criteria included being a national/regional club football player (one selected sport only) and having a valid birth certificate.
MRI assessment of the epiphysial growth plate showed a high interrater reliability (three readers) with r=0.95 (agreement with majority reading 0.98) and re-test reliability ranging between 0.95 and 0.98. The MRI physial closure grading showed a significant correlation with increasing age groups, with age accounting for approximately 48% variance in the fusion status (r=0.69). The age for any given fusion status varied quite widely, but only one player younger than 17 years (representing 0.8% of the total population under 17 years) was graded as completely fused (a Malaysian player). Nonetheless, a large number of players over 17 years of age (85%) was not completely fused either, suggesting that, while ‘complete fusion’ as an indicator of a player being 17 years or older was highly sensitive (96%; few false positives), this indicator was not very specific (59%; many false negatives). Therefore, the lack of complete fusion would still not necessarily rule out the fact that a player was older than 17 years of age. It did, however, suggest that the odds of a player being under 17 years of age and presenting complete fusion is likely to be very high.
In a second step, the F-MARC group applied the MRI of the wrist for age determination in international U17 football tournaments.89 A representative sample of 189 young elite football players from four international championships was examined; for two of the championships the players had to be under 17 years, for the other two tournaments, players had to be 17 years or younger.
The results of these assessments differed significantly from the initially published findings.90 In the first instance, there was a higher percentage of closed physial plate through all age groups; a total of 21% in the whole group examined compared with a proportion of 5% in the 16 and 17-year olds in the initial study. Furthermore, in contrast to the reference group, no significant correlation was observed between the age category and degree of fusion. Overall, the players in the international U17 tournaments appeared to be more mature skeletally than a reference population of footballers of a similar age.
On the basis of these two investigations, the authors suggested that: MRI was a viable tool for screening players in youth competitions, particularly the U16 and U17 groups and the documented ages of the participants in the U17 tournaments may not be accurate in all cases.
The authors recommended that the MRI approach should be extended to other ethnic groups, and that height and weight, and possibly also height and weight velocity, should also be documented for age determination. Conceivably, the incorporation of these influential factors and others such as gender, ethnicity and sporting skill level into an algorithm for predicting age might improve the accuracy of age prediction. Rather than challenging the MRI methodology per se, it appears that there is a need for further investigations on the basic premise upon which the imaging is based; whether with radiographs or MRI. Certainly the feasibility of the use of MRI as a screening tool at tournaments, including standardised protocol and patient positioning, was adequately demonstrated.89 90
There is currently no evidence to support the use of MRI studies of the wrist for age determination of athletes below 14 years and above 17 years of age. However, age determination by MRI bodes well for its future use, if a more accurate age prediction algorithm can indeed be developed.
Use of ultrasound in age determination
Ultrasound of the wrist and elbow is another radiation-free technique with the potential to be developed as a tool for age determination. Ultrasound has advantages over other methods in that it is relatively inexpensive and widely available. Ultrasound can easily be applied by using portable systems on-site at tournaments, and patient compliance is generally good.
The limitations of ultrasound include its operator dependence, the likely lower intrarater and interrater reliability of assessment, and the difficulties with standardisation of documentation and imaging transfer. There are few data available regarding age determination from the wrist, beyond a single preliminary report.91 Recently an application was introduced using a fixed transducer device (BonAge®, Sunlight Medical Ltd, Nashville, TN, USA), which measures a conductive velocity for age determination in the growth plate. So far, ultrasound as a method to assess skeletal maturity has been studied by Mentzel et al,92 followed by diverging evidence to its validity value when compared with Greulich–Pyle and TW3 methods.93
To gain further knowledge on the value of ultrasound for age determination, the use of ultrasound needs to be validated against the existing gold standard of radiological assessment.
Future directions and research
At present, radiographic methods for the assessment of bone age remain the gold standard. Further research is needed, however, to evaluate the reliability and validity of bone age assessments in the process of maturation.
There is benefit in extending the existing MRI studies performed in football89 90 to other sports or to the clinical setting. Comparisons of MRI assessments with established radiographic scoring systems (Greulich–Pyle, TW3) are needed to provide evidence on the validity of MRI assessments. These will clarify whether some of the apparent discrepancies revealed to date are attributable to differences in ‘skeletal maturation versus chronological age’ rather than the accuracy of the MRI method per se. As the distal epiphysis of the radius closes rather late in the process of maturity, the closure of other growth plates might be investigated in order to allow age determination and classification in younger age groups. The areas around the elbow and the shoulder have a broader time spectrum of epiphysial ossification and fusion in individuals between 14 and 18 years of age. Radiographic examination of these areas may offer a better discrimination of skeletal maturity in these age intervals of sports. The use of MRI in the elbow with well evaluated age distributions using the Sauvagrain method should be considered and tested. However, the use of x-rays for the present purpose contradicts the ethical rules of WHO and the International Atomic Energy Agency.
A validation of ultrasound for age determination could be carried out in institutes in which routine radiographs of the left hand are used for the assessment of bone age. Whenever such an x-ray is required for various reasons, a supplementary examination (MRI and/or ultrasound) should automatically be included in combination with registration of anthropometric and other data including age, weight, standing and sitting height, mother's and father's stature and sports activities including level of activity. Two other future non-radiological markers of age, although probably well into the future, are biomarkers of ‘cellular age,’ including the assessment of telomere shortening and the measurement of the expression of p16INK4a in peripheral blood T cells. The use of this in children has not been studied at present and as such remains theoretical, but in adults there is increasing evidence that this may be a good way of determining physiological/chronological age in the future.94 95
Conclusion
The development and use of appropriate methods for determining age is not only necessary to ensure a level playing field, but also to protect the health and safety of the adolescent athlete. However, the evidence for the influence of biological maturity on overall injury incidence is somewhat conflicting. Although the determination of chronological age has been the focus in sport to ensure appropriate participation, non-pathological variance in pubertal development is likely to be one of the ‘natural advantages’ in elite athletes that facilitates their achievement. The available methods to determine chronological age in youth elite athletes, including blood samples, x-ray, ultrasound and MRI, are not sufficient.
The large variation in the timing of puberty that is considered within the range of normal, not to mention the occurrence of significantly delayed or precocious puberty, makes it difficult to ‘level the field’ in sport in relation to physical maturity. As hormonal values, extracted from blood samples, are dependent on pubertal development, a ‘set of hormonal markers’ to determine age will not be feasible. The assessment of skeletal age by x-ray scanning does not allow a precise determination of the chronological age as variations up to 4 years in bone age have been observed in adolescents of the same chronological age. To summarise the current knowledge regarding the use of non-invasive (radiation-free) methods for age determination: (1) MRI allows a reproducible grading of epiphysial closure; (2) the MRI method of assessment established in football is so far sports (football) and age specific (<17 years), with international football players appearing to mature earlier than national/regional club players; (3) there is currently no evidence to support the use of MRI studies of the wrist for age determination of athletes below 14 years and above 17 years of age; (4) the validity and wider applicability of MRI in age determination should be examined; (5) the usefulness of ultrasound remains largely unknown. Age determination by ultrasound may have the potential to assess growth plates in the wrist or elbow, but further validation studies of ultrasound measurements are needed.
References
Footnotes
-
Funding The funding for the consensus meeting was supplied by the IOC.
-
Competing interests None.
Provenance and peer review Commissioned; not externally peer-reviewed.
Linked Articles
- Miscellaneous