Article Text

Statistics from Altmetric.com
Introduction
Elite-level athletic training and competition is accompanied by the recovery of a series of physiological stressors. The physiological stress will vary considerably depending upon the specific exercise type, duration and intensity and also on the athletes' familiarisation to the exercise insult. It is well documented that when the exercise stress incorporates a novel eccentric component or the exercise is of considerable intensity or duration,1 athletes will likely experience numerous signs and symptoms of fatigue and cellular disturbance that have the potential to reduce performance.
Physiological stress induced by intense exercise is associated with energy substrate depletion, hyperthermia, mechanical muscle damage, oxidative stress, inflammation and nervous system fatigue. The resulting symptoms manifest as reduced performance potential, likely due to increased muscle soreness and decreased muscle function,2 disturbed muscle position sense and reaction time3 as well as increased stiffness and swelling that can last for several days.4 The aetiology of reduced performance potential will vary depending upon the exact physiological stress being recovered from. For example, eccentric exercise is associated with a large mechanical stress and relatively low metabolic cost,5 whereas intermittent sprint exercise may involve both a large mechanical stress and a heightened metabolic cost.6 It is possible that the underlying time course of recovery between different exercise stressors is different, and this consequently may influence how recovery strategies could be implemented. For the purpose of this review, exercise will be subdivided into two categories: ‘eccentric exercise’ that refers to the stress caused from exercise incorporating high mechanical stress (eg, eccentric contractions) and ‘high-intensity exercise’ that refers to stress caused from exercise with a high metabolic cost as well as some elements of eccentric muscle contractions (eg, repeat sprint sports).
Given the potential for physiological stress to compromise training and/or competition performance, there has been significant attention in both applied practice and research to identify optimal recovery strategies in these scenarios.7,–,9 Cold water immersions (CWI) are a frequently used and popular recovery modality. The mechanisms of CWI are speculated to be related to temperature- and pressure-induced changes in blood flow and reduced muscle temperature per se,10 11 subsequently reducing post-exercise inflammation.12 13 This proposed reduction in inflammation might be related to attenuated delayed-onset muscle soreness (DOMS) and enhanced recovery of muscle function.14
Attempting to increase rate of recovery may be beneficial to the elite athlete. For example, following high-intensity intermittent sprint sports, it is common for athletes to experience elevated muscle soreness and reductions in muscle function of up to 20% for several days after the exercise insult.15,–,17 This physiological impairment provides rationale to attempt to enhance rate of recovery in the elite athlete, especially when repeated performance is required in tournament scenarios or multi-day competition (eg, cycling stage races). In recent years, there has been an increase in the quantity of research focusing on CWI, yet findings remain unclear and have been proposed to be related to inconsistencies in exercise modalities, CWI protocols and dependent variables measured. A systematic review of the research findings will provide clarity on the efficacy of water immersions as suitable recovery strategies following strenuous physical activity. Therefore, the aim of this investigation was to systematically review and discuss the literature regarding the efficacy of CWI following the two categories of physiological stress precipitated from eccentric and high-intensity exercise insults.
Methods
Systematic review/literature search strategy
The systematic review with meta-analysis was completed in accordance with the recommendations outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.18 A computerised literature search was conducted, ending in May 2010, using Medline (PubMed), SportDiscus and ISI Web of Knowledge. The following key phrases and their combinations were used: CWI, ice bath, recovery strategy, recovery modality and exercise-induced muscle damage. Reference lists of all articles were examined for identification of further eligible studies.
Outcome variables
The research literature was examined for the effects of CWI on recovery from physiological stress caused by eccentric and high-intensity exercise, using four outcome variables: muscle power, muscle strength, muscle soreness (DOMS) and creatine kinase (CK). (1) Muscle power was defined as an exercise test that measures explosive muscular power (eg, a vertical jump or a 5 m sprint). (2) Muscle strength was defined as a test of isometric/isokinetic knee extension or elbow flexion only. The rationale for inclusion of these tests of muscle strength was to provide consistency in comparison of muscle groups and contractions. They are also the most common tests, resulting in the maximal amount of comparable muscle strength data for meta-analysis. (3) DOMS was defined as a participant's perception of muscle soreness, using visual analogue scales or algometry. (4) Measurements of CK were defined as venous or capillary CK. The rationale for inclusion of these four outcome variables was that they have been shown to reflect the presence of exercise-induced muscle damage, albeit with different levels of accuracy19 and are commonly used by researchers and applied practitioners to indentify a recovery profile following strenuous exercise.
Study inclusion and exclusion criteria
Studies meeting the following criteria were considered for review: (1) The study design was randomised into an intervention group and a control group; (2) a minimum of one of the four outcome variables were reported; (3) only outcome variables measured at 24 h, 48 h, 72 h or 96 h post exercise were included; (4) CWI was applied within 1 h post exercise and permitted to be repeated on subsequent days and (5) participants could be male or female and of any athletic training status. Studies were excluded when (1) the control group received an intervention with rationale to improve recovery; (2) the observed effect could not specifically be attributed to intervention group (eg, CWI group received multiple interventions, such as active recovery and CWI) and (3) there were insufficient data to report an effect size.
Data extraction and assessment of risk of bias
For the meta-analysis, data were extracted in the form of mean, standard deviation and sample size. In some cases, data were calculated using raw baseline values with subsequent percentage changes. When insufficient raw data were provided to deduce an effect size, data were extrapolated from figures and graphs. Risk of bias (figure 1) was calculated according to the Cochrane Collaboration's guidelines.20
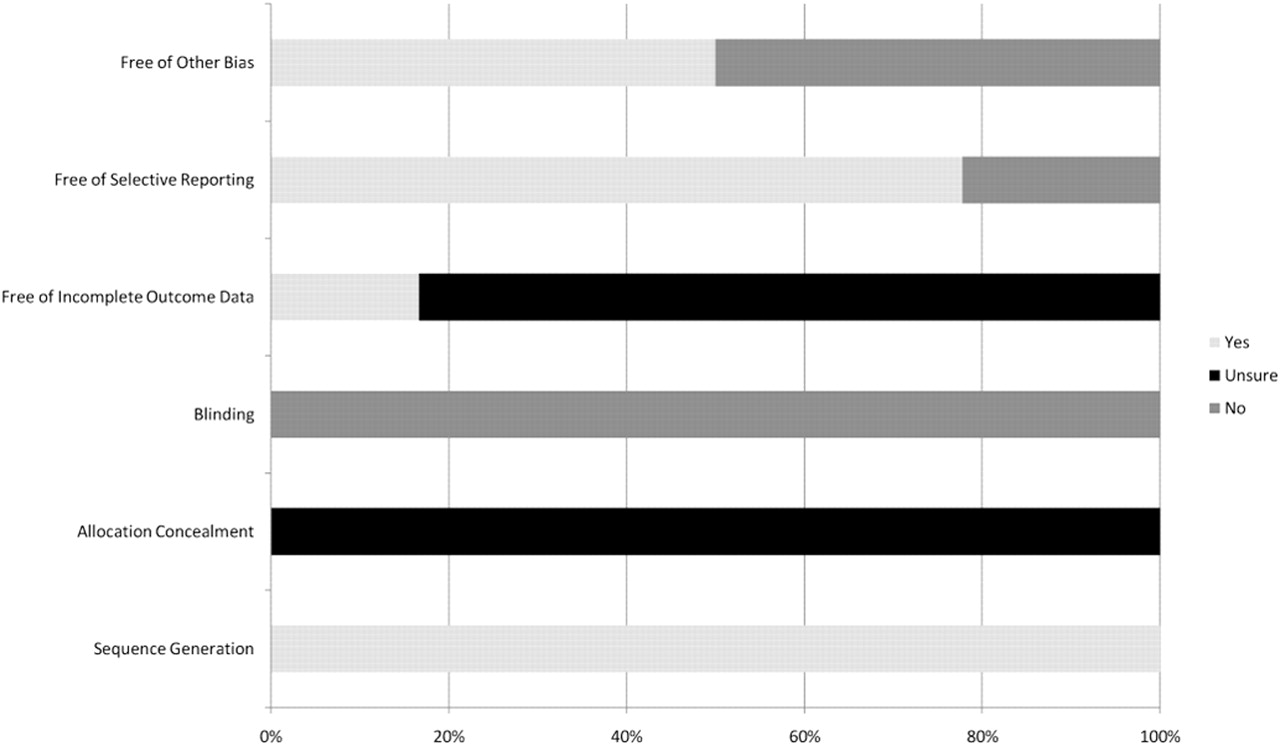
Analysis of risk of bias according to Cochrane Collaboration guidelines.20
Meta-analysis
All meta-analyses calculations were conducted with the Comprehensive Meta-Analysis software (Version 2.2.057; Biostat Inc., Englewood, New Jersey, USA). The standardised mean differences were calculated (Hedges' g) and 95% CI for trials with sufficient data.21 The analysis of pooled data was conducted using a fixed-effect model, so that any heterogeneity between studies could be determined.22 Heterogeneity was assessed using the I2 statistic,23 which describes the percentage of variability in effect estimates that is due to heterogeneity rather than chance. When I2 was >30% (30–60% represents moderate heterogeneity),21 a subgroup meta-analysis of time of measurement post exercise was completed to investigate source of heterogeneity. If heterogeneity still existed, a further subanalysis of exercise type (eccentric or high intensity) was completed. Significance was set at p<0.05.
Results
Fourteen studies meeting the inclusion criteria (table 1) had data extracted for meta-analysis from an original search of 7 193 (figure 2). Participants' level of physical activity ranged from untrained to elite athlete groups, with a mean age of 23.2 ± 3.5 years. The total number of participants was 239 and the distribution of gender was not equal (male, n = 182; female, n = 57). The main findings from the assessment of risk of bias in the included studies revealed that none of the included studies was able to effectively blind participants from the treatment (figure 2).
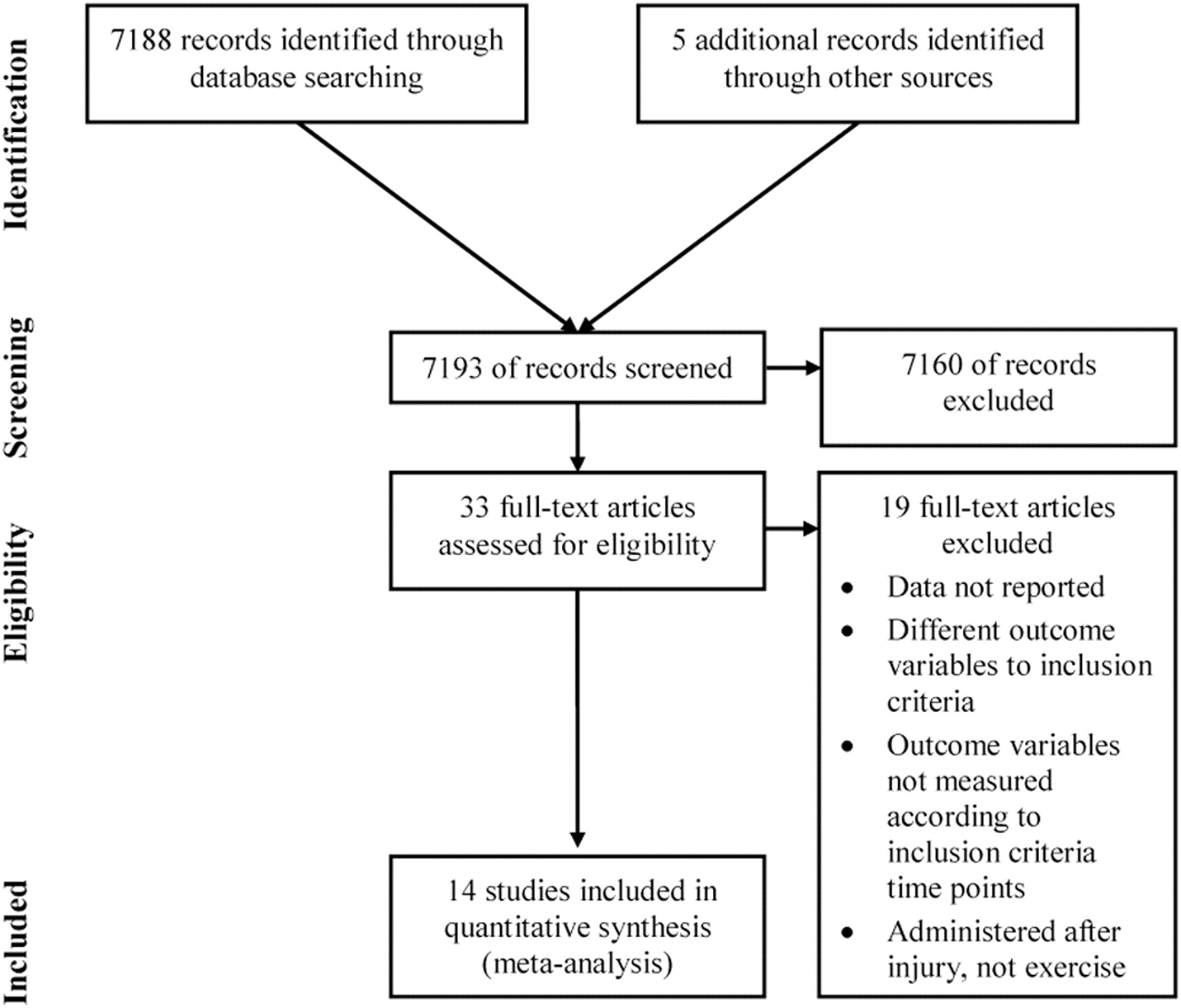
Schematic of selection of studies from initial identification to final inclusion.
Summary of relevant peer-reviewed sources of data included for meta-analysis
DOMS meta-analysis
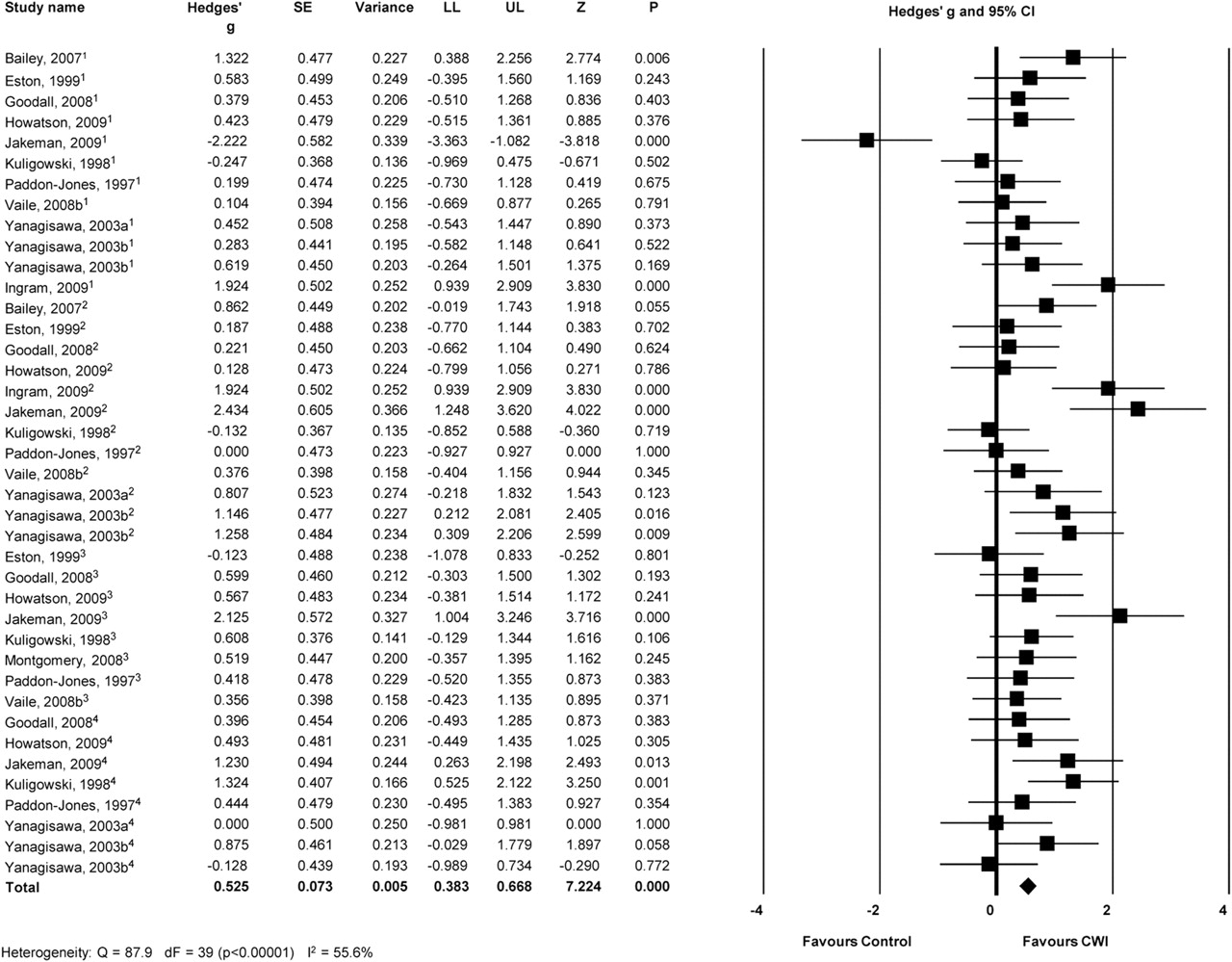
CWI had a moderate effect in alleviating DOMS post exercise (Hedges' g = 0.525, p < 0.001; figure 3) from a total of 40 extracted data points. The I2 statistic of 55.6% revealed moderate to high heterogeneity in the results. Consequently, a subgroup meta-analysis of time post exercise was completed (table 2). CWI was effective in alleviating DOMS at all time points up to 96 h post exercise. Substantial heterogeneity still existed at 24 and 48 h post exercise (70.5 and 60.8%, respectively) so a further subgroup analysis of exercise type (eccentric or high intensity) was completed to further investigate the source of heterogeneity. Table 2 shows that CWI was highly effective in alleviating DOMS following high-intensity exercise at 24 and 48 h (Hedges' g = 1.675 and 1.391, respectively, p < 0.001). CWI did not reduce DOMS at 24 h post eccentric exercise (Hedges' g = 0.116, p = 0.440) but had a moderate effect at 48 h post eccentric exercise (Hedges' g = 0.532, p = 0.001).

Forest plot of meta-analyses illustrating comparison of cold water immersion (CWI) versus control for measures of delayed-onset muscle soreness (DOMS). 1–4 refer to studies measuring at 24, 48, 72 and 96 h post exercise, respectively. Squares represent individual study Hedges' g and the lines represent 95% CIs. The size of the square is proportional to the weight of the study within the meta-analysis. The diamond represents the overall Hedges' g, with the width of the diamond signifying the 95% CIs. LL, lower limit and UL, upper limit of 95% CIs; dF = degrees of freedom.
CK meta-analysis
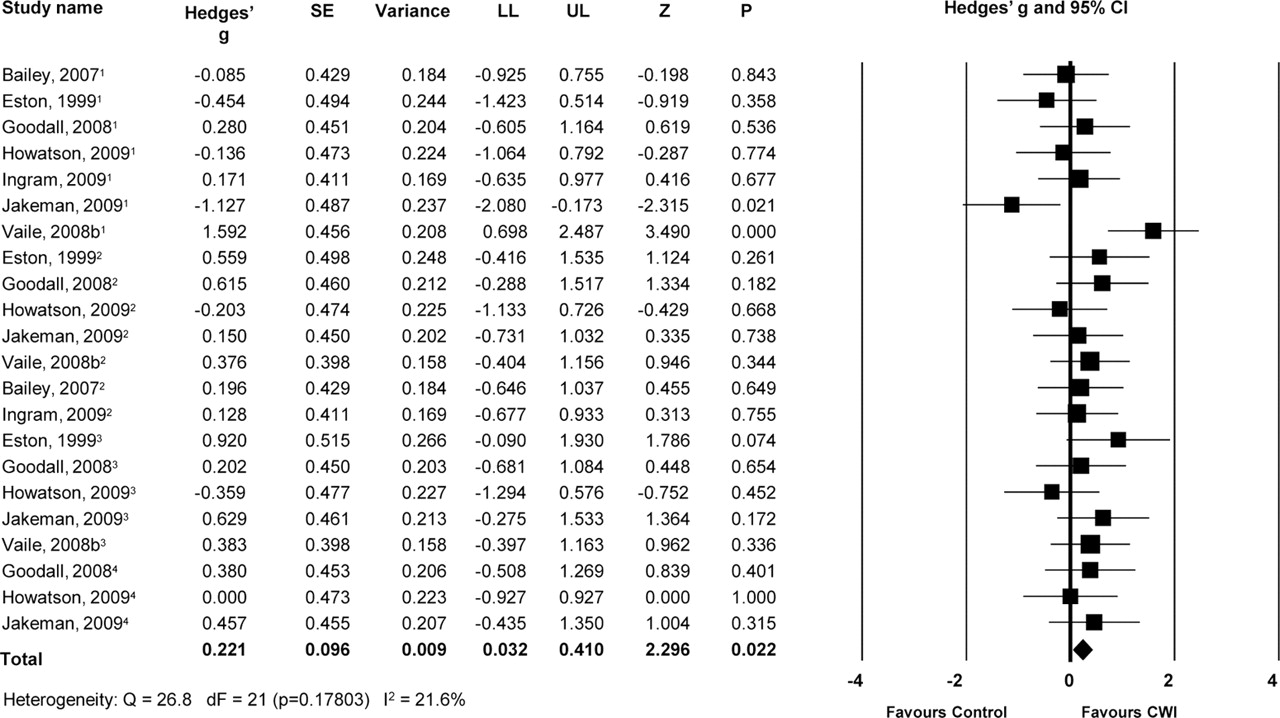
Figure 4 shows CWI was effective in reducing efflux of CK in the blood post exercise from a sample of 22 extracted data points. Although this finding was significant (p = 0.022), a Hedges' g of 0.221 revealed a small effect (figure 4). The I2 statistic revealed minimal heterogeneity (21.6%) so no further subgroup meta-analyses of time post exercise or exercise type were completed.
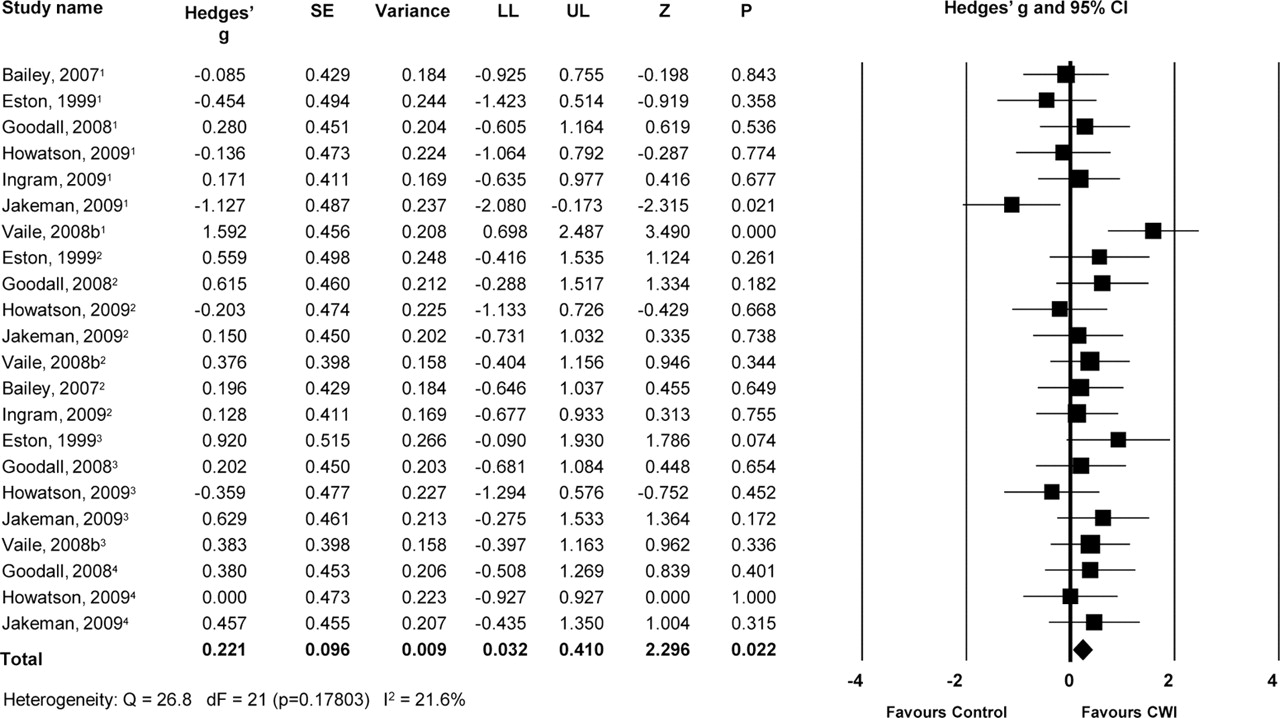
Forest plot of meta-analyses illustrating comparison of cold water immersion (CWI) versus control for measures of creatine kinase (CK). 1–3 refer to studies measuring at 24, 48 and 72 h post exercise, respectively. Squares represent individual study Hedges' g and the lines represent 95% CIs. The size of the square is proportional to the weight of the study within the meta-analysis. The diamond represents the overall Hedges' g, with the width of the diamond signifying the 95% CIs. dF, degrees of freedom; LL, lower limit and UL, upper limit of 95% CIs.
Muscle strength meta-analysis
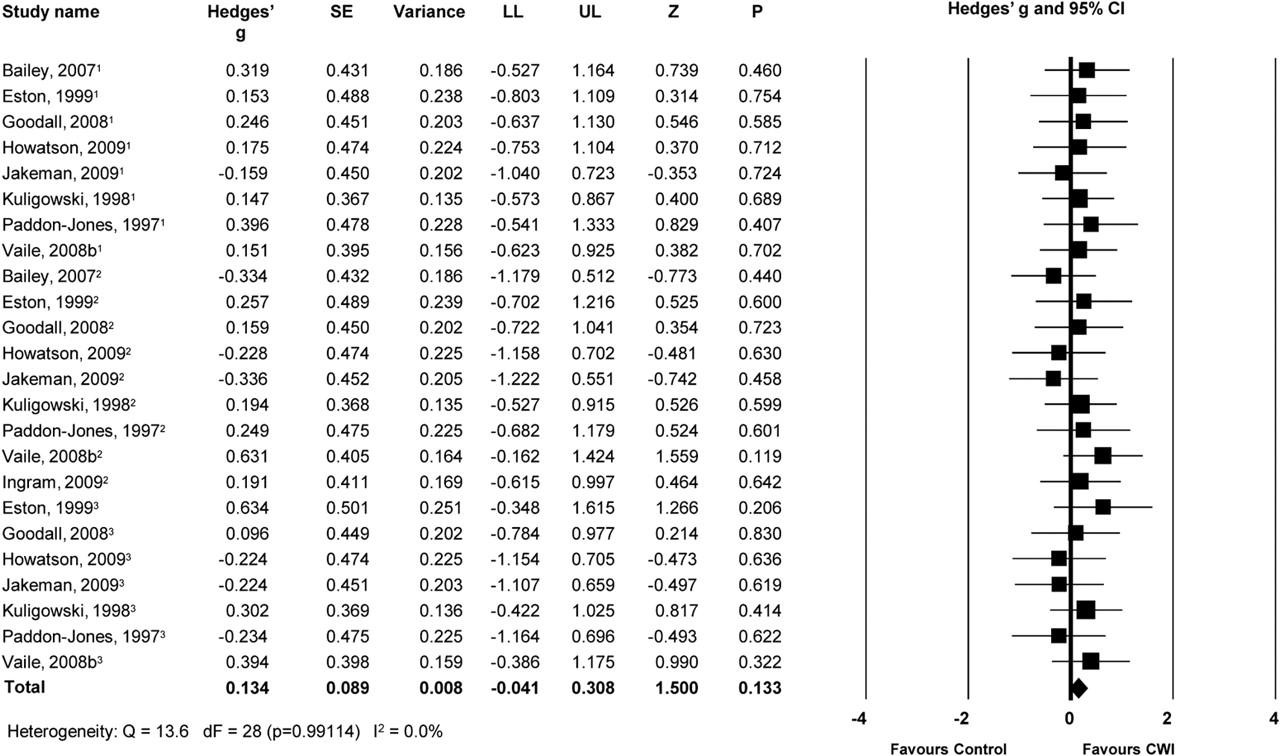
Figure 5 shows CWI was not effective in improving rate of recovery of muscle strength post exercise from a sample of 29 extracted data points (Hedges' g = 0.134, p = 0.133). The I2 statistic revealed minimal heterogeneity (0.0%) so no further subgroup meta-analyses of time post exercise or exercise type were completed.
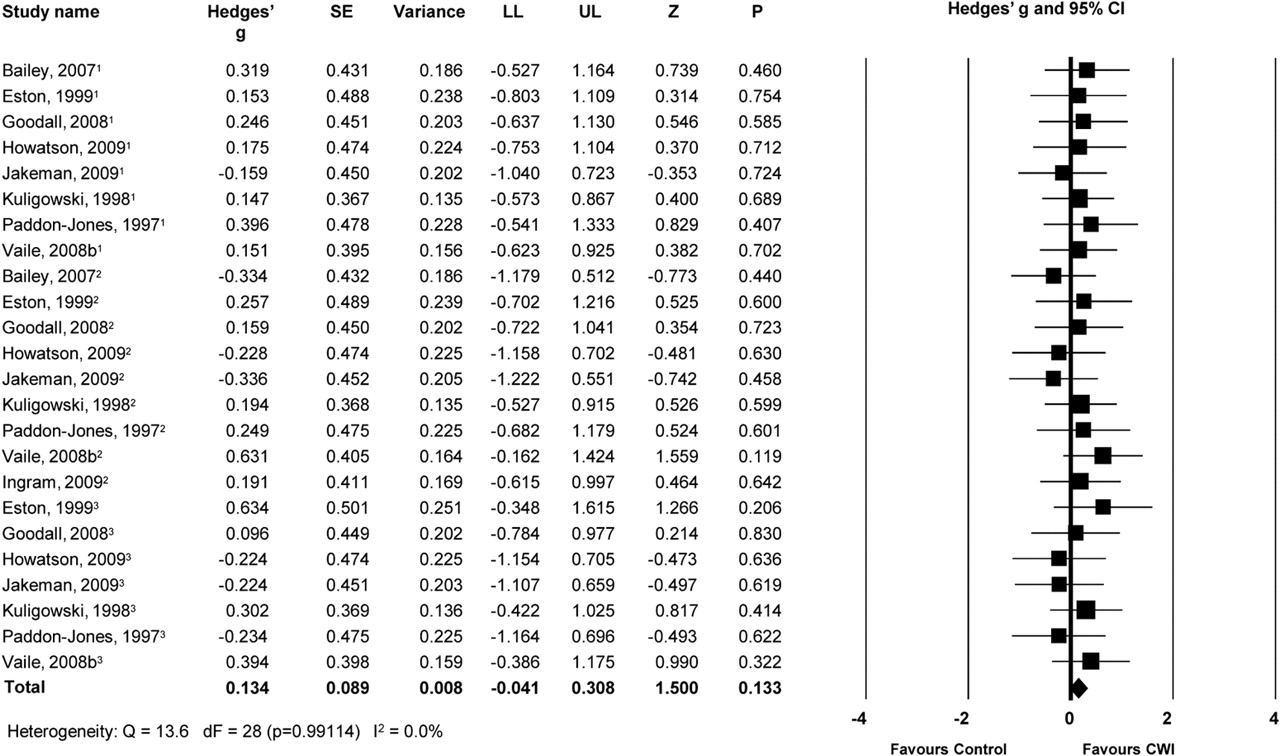
Forest plot of meta-analyses illustrating comparison of cold water immersion (CWI) versus control for measures of muscle strength. 1–3 refer to studies measuring at 24, 48 and 72 h post exercise, respectively. Squares represent individual study Hedges' g and the lines represent 95% CIs. The size of the square is proportional to the weight of the study within the meta-analysis. The diamond represents the overall Hedges' g, with the width of the diamond signifying the 95% CIs. dF = degrees of freedom; LL, lower limit and UL, upper limit of 95% CIs.
Muscle power meta-analysis
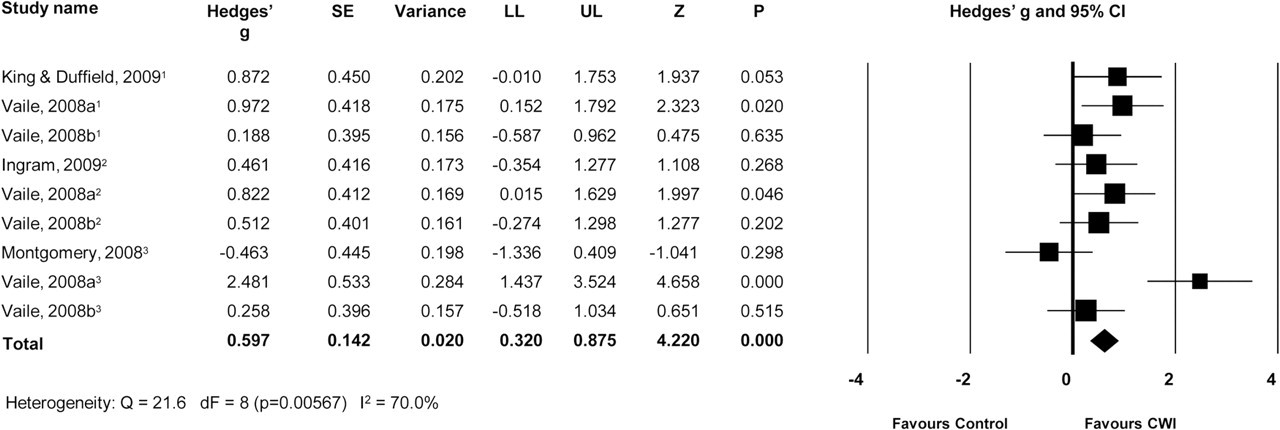
Figure 6 shows CWI was effective in improving rate of recovery of muscle power post exercise from a sample of nine extracted data points (Hedges' g = 0.597, p < 0.001). The I2 statistic of 70.0% revealed moderate to high heterogeneity in the results. Consequently, a subgroup meta-analysis of time post exercise was completed (table 2). CWI was effective in improving recovery of muscle power at all time points (24, 48 and 72 h post exercise), with heterogeneity reduced at 24 and 48 h post exercise (table 2). No further subanalysis of heterogeneity was conducted at 72 h post exercise (I2 = 89.4%) due to an n of only three studies.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of meta-analyses illustrating comparison of cold water immersion (CWI) versus control for measures of muscle power. 1–3 refer to studies measuring at 24, 48 and 72 h post exercise, respectively. Squares represent individual study Hedges' g and the lines represent 95% CIs. The size of the square is proportional to the weight of the study within the meta-analysis. The diamond represents the overall Hedges' g, with the width of the diamond signifying the 95% CIs. dF, degrees of freedom; LL, lower limit and UL, upper limit of 95% CIs.
Discussion
The efficacy of CWI has not been clearly established despite the large volume of research, therefore this systematic review of literature has provided insight into the potential benefits conferred by such interventions that allow practitioners to make an informed decision on their efficacy and application. The main findings of this study were as follows: (1) CWI alleviated symptoms of DOMS at 24, 48, 72 and 96 h post exercise and was effective at 24 and 48 h following high intensity exercise. (2) CWI had a small but significant effect in reducing efflux of CK post exercise. (3) CWI had no effect on recovery of muscle strength but was effective in improving recovery of muscle power.
One proposed mechanism of CWI is a cold-induced reduction in muscle blood flow and tissue temperature causing decreased inflammation induced via strenuous exercise. Gregson et al10 recently showed reduced femoral artery blood flow (>40%) and muscle temperature (2–4°C) following 10 min of immersion in 8°C and 22°C water. The proposed reduction in inflammation is associated with a reduction of the sensation of pain caused by reducing the osmotic pressure of exudate, which pressurises nociceptors, signalling pain via type IV afferent fibres.14 24,–,26 Cold-induced vasoconstriction is thought to reduce permeability of cellular, lymphatic and capillary vessels, which reduces fluid diffusion into the interstitial space, which is the suggested mechanism of reduced inflammation following muscle-damaging exercise.27 The reduction in muscle tissue temperature following CWI is another proposed mechanism of CWI and may reduce metabolic enzymatic activity and limit secondary hypoxic damage to uninjured cells.28 Myrer et al29 indicated that the amount of adipose over the area of cold treatment significantly affects rate of intramuscular cooling and therefore should be taken into account when administering CWI protocols to athletes of varying body composition. It is currently unknown whether the major mechanism of CWI is reduced blood flow or whether tissue temperature needs to be reduced concomitantly.
The present findings show that CWI appears to be an effective analgesic, lasting up to 96 h post exercise. The overall Hedges' G of 0.53 (figure 3) suggests that 69% of the population will likely experience lower DOMS using CWI30; however, this does not indicate the magnitude of DOMS reduction. For comparative purposes, DOMS scores from visual analogue scales were standardised and compared retrospectively between control and CWI groups.12 13 15 16 31,–,36 The results showed CWI reduced perception of soreness on average by 16%. Whether this outweighs the logistical inconvenience of CWI remains the decision of the applied practitioner. Interestingly, at 24 and 48 h post exercise, CWI appears to have more effective analgesic properties following high-intensity exercise than eccentric biased exercise (table 2). Further mechanistic work is needed to understand the physiological effects of CWI following different exercise types to elucidate whether this is a true physiological effect or simply reflects the placebo effect.
Given the perceptual nature of DOMS assessments, it is plausible that the placebo effect phenomenon may have an impact on the efficacy of CWI as recovery strategy.37 Given the rapidly increasing popularity of water immersion recovery strategies, despite a lack of evidence to support their use, it is quite possible that participants believed and expected a positive outcome from CWI, thereby influencing the measure of DOMS. Unfortunately, due to the nature of water immersion, it is not possible to provide a true placebo condition within such experimental trials. Figure 2 indicates this by the high risk of bias in the blinding category. Whether the placebo effect contaminates these results or whether in fact it is an important aspect of any recovery strategy remains to be elucidated and warrants further consideration in future research. Studies which incorporate objective methods of inflammation and swelling, as well as subjective markers of perception of soreness, will contribute to understanding of the role of the placebo effect in CWI research.
Cold water immersion was not effective at improving recovery of muscle strength post exercise. The effect of eccentric exercise on muscle strength has been extensively reviewed and is proposed to relate to disrupted sarcomeres in myofibrils and damage to the excitation-contraction coupling system.38,–,40 Following the primary phase of muscle damage, a disruption in calcium homeostasis in the cytosol leads to a cascade of events following the exercise that further damages the cell partly via oxidative mechanisms.9 It would appear CWI is not able to alleviate this secondary damage and muscle strength loss; however, there is little evidence investigating the potential mechanism of CWI reducing post-exercise oxidative stress.
The only positive effect of improving recovery of muscle function was in tests of muscle power. The effect of CWI acting specifically to recovery of muscle power and not muscle strength is an interesting finding with no obvious explanation, so the following proposed mechanisms are speculative. Inter-individual differences in muscle strength are predominated by muscle cross-sectional area,41 whereas muscle power involves an intricate interaction of muscle cross-sectional area and excitation-relaxation kinetics.42 It is unknown whether CWI may specifically affect different characteristics of the force–velocity relationship of skeletal muscle. An alternative explanation is that type 2 fibres are preferentially damaged following eccentric exercise and are the predominant fibre type in high-velocity muscle contractions involving elevated power production.24 It could be speculated CWI is associated with a heightened recovery of type 2 fibres. Following strenuous exercise such as various field sports, preferential recovery of power over strength may have implications for periodising training in subsequent days. Whether CWI has specificity to recover muscle power over strength requires further research.
Following high-intensity exercise, CWI was more effective at alleviating DOMS at 24 and 48 h than following eccentric exercise (table 2). While there are physiological differences between high-intensity exercise and eccentric exercise, it is difficult to explain the mechanisms of action as to why CWI may be more efficacious following high-intensity exercise than eccentric exercise. It was also clear that although markers of physiological stress and recovery may appear to be similar following different exercise modes, the underlying aetiology of the stress is likely to be different between the two exercise modes. Bimodal contributions to reduced performance potential following strenuous exercise are speculated to be (1) an initial mechanical and/or metabolic muscle injury that transpires during the exercise and (2) a secondary phase subsequent to the exercise that involves a disruption in intracellular homeostasis followed by an inflammatory response.9 It is suggested the contributions of the mechanical and metabolic stress that contribute to this first phase of physiological disturbance vary considerably between eccentric and high-intensity exercise types. Furthermore, identification and analysis of indices thought to be implicated in various causes of physiological stress, such as oxidative stress, substrate depletion, hyperthermia, stress hormones and cytokines, as well as the common markers of recovery will help contribute to understanding the recovery process and provide greater rationale for the inclusion of interventions.
Vaile et al36 43 have consistently found positive effects from CWI on recovery of muscle power. One lucid difference of these studies is the contribution of hydrostatic pressure by immersing to the neck. The physiological responses to hydrostatic pressure have been extensively reviewed.27 During thermoneutral water immersions to the neck, there is a displacement of fluid and gas from higher pressure areas at the ankle to low pressure areas at the water surface. This ‘squeezing’ effect induces alterations in fluid within the intracellular, interstitial and intravascular spaces. Water immersion causes increases in central blood volume44 due to fluid shifts from interstitial to intravascular space.27 This is one proposed mechanism of hydrostatic pressure to reduce oedema caused by strenuous exercise. Research has not yet focused on controlling water temperature and assessing the effect of different hydrostatic pressures. This could help ascertain the contribution of hydrostatic pressure to the efficacy of water immersions.
Intramuscular proteins have been extensively used as biochemical markers of muscle damage. Figure 4 indicates that although there was a statistically significant reduction (p = 0.022) in the efflux of CK post exercise, the Hedges' g of 0.221 showed this was a very small effect. This agrees with recommendations from Warren et al19 not to use intramuscular proteins as markers of muscle damage as they do not accurately reflect functional loss resulting from strenuous exercise. Blood levels of intramuscular proteins represent a balance not only between rate of release but also between rate of removal. Consequently, measurement of CK is likely to be sensitive to changes in blood flow, which may explain the high variability of this measure. Clarkson et al45 showed that following eccentric exercise, variations in participant genotypes that code for myofibrillar proteins influence the phenotypic response to muscle damage response in the form of CK and functional loss of strength. This is a potential reason for diverse inter-individual CK responses to strenuous exercise, despite similar participant characteristics (age, sex, athletic status).
A rationale for utilising CWI is to reduce the post-exercise inflammatory response, with the aim of minimising the reduction of muscle function and increase in DOMS associated with strenuous exercise. It has, however, been suggested that the inflammatory response is critical for optimal repair of damaged tissue.28 Although the mechanisms of training adaptation are not fully understood, it may be detrimental to reduce the commonly accepted damage-repair-adaptation model by diminishing the inflammatory response; however, there is a lack of evidence to support this.32 46 This raises the question of whether frequent or habitual use of strategies designed to reduce inflammatory responses can be detrimental for elite athlete adaptation to training.
Conclusion
CWI is frequently used as a recovery modality from strenuous exercise, despite a lack of evidence-based guidelines. This review illustrates that CWI is an effective strategy to reduce DOMS following a range of exercise types, yet the mechanisms remain elusive. While the effects of CWI on recovery of muscle function were less clear, the positive effects of alleviating soreness with a large body of evidence endorses utilisation of CWI. Various other strategies purport to enhance recovery from exercise,9 yet to date, CWI is the only strategy with a systematic review to promote its efficacy.
The majority of current research is descriptive in nature and therefore contributes a limited amount to the understanding of the potential mechanisms underpinning the effects of specific recovery strategies. There are many areas that future mechanistic research should address, with the most pertinent topics being the effects of water temperature, hydrostatic pressure and the application following different exercise types. In addition, it is critical to elucidate the physiological processes affected by water immersions to gain a clearer understanding of both the short-term and long-term effects of their use. This review highlights to the applied practitioner that it may be important to understand the physiological stress induced following different exercise types before prescribing recovery modalities. While it is apparent that CWI has no acute negative effects on recovery from strenuous exercise, research should investigate chronic application on adaptation to training.
References
Footnotes
-
Competing interests None.
-
Funding None.
-
Provenance and peer review Not commissioned; externally peer reviewed.