Article Text

Statistics from Altmetric.com
Illness or injury affected four out of every five athletes on the Great Britain Track and Field Team before, during or immediately after the 2012 Olympic Games.1 The return to play (RTP) decision is a case of risk management, and athletes may continue to train or compete, despite being ill or injured. This begs the question: ‘How is the return to play decision made in elite sport’?
RTP decisions are complex, specific to the athlete and type of sport, and often influenced by ‘decision modification’ factors (eg, pressure to return for a major event).2 In the case of a sprinter with a hamstring strain 2 weeks from the World Championships, the final RTP decision-maker might be the athlete. However, the healthcare professional should be the final RTP decision-maker when athlete decision-making capacity is compromised (eg, concussion). Decisions regarding the immediate medical management (including RTP) of an ill or injured player on the field of play should be made by a healthcare professional. The coach or manager should have no say in whether the medical team should attend the athlete, or in immediate player assessment.3
Where an athlete has the capacity to make a decision, we propose (and use) a shared decision-making (SDM) process; this approach improves outcomes and satisfaction with treatment.4
The three key steps in SDM are:5
Choice: making the athlete and coach aware that reasonable options exist;
Option: providing more detailed information about the different options;
Decision: guiding the athlete and coach to consider their preference and decide what is best.
Role definition in sports medicine SDM
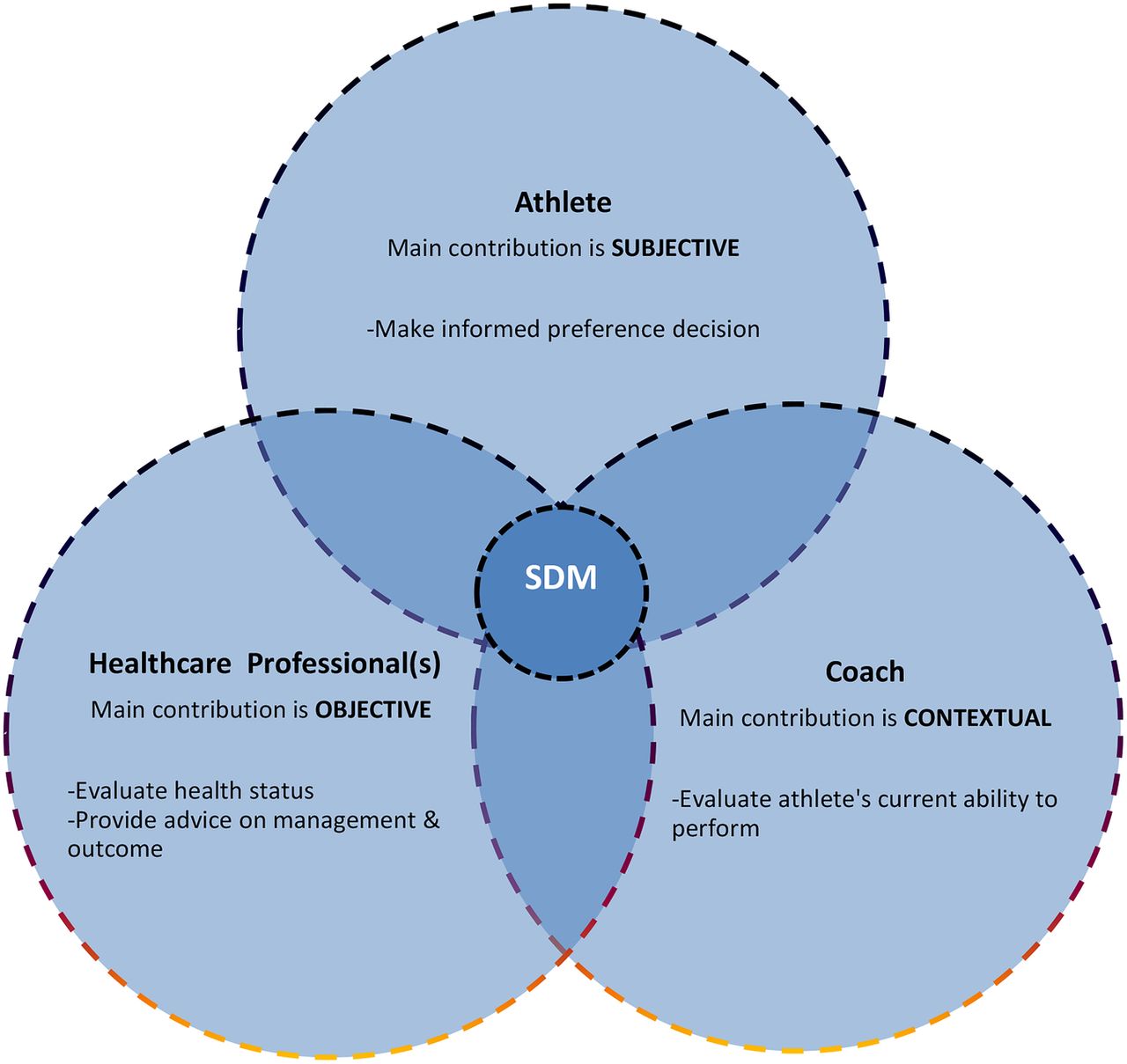
The three key people in SDM (figure 1):
Healthcare professional: The most appropriate person to evaluate the health status of the athlete and provide objective advice on management options and possible clinical outcomes following RTP (usually a sports physician and/or physiotherapist). This includes the short-term risk of performance detriment or reinjury, the consequences of reinjury and the long-term health (and performance) risk. This advice is primarily based on the clinical situation—the context of the real athlete with a very specific problem. Professional experience, sport-specific injury and performance knowledge and a relationship with the individual athlete, framed by an understanding of the relevant published scientific evidence, are the important elements of the decision-making process. In elite sport, this advice is usually informed by input from the supporting team of healthcare professionals who work with the athlete.
Athlete: When fully competent, the athlete should make an informed decision about his/her readiness and desire to RTP. This decision is based on personal circumstances and experience, his/her intrinsic view on risk taking, the environment and specific information regarding health and performance. Contextual factors that may be relevant to the athlete include sponsorship deals or media pressure. Despite the athlete's preference, at the highest level of elite sport, there are often wider performance implications with impact on other athletes in the team (and in individual events) that need to be considered (ie, one rower causing a rowing 8 to fail). Therefore, the final decisions regarding selection, participation and RTP are not usually made in isolation. The athlete's input is a pre-requisite.
Coach: The informed coach evaluates the current ability of the athlete to perform to a specific required standard, based on knowledge of the athlete, the training missed, the athlete's functional progression in rehabilitation and the information provided by healthcare professionals. The coach's contribution to the RTP discussion relates to the sport-specific context. For example, the coach of an Olympic triple jumper will not use the same RTP criteria as the coach of an Olympic football or rugby sevens team. In elite sport, only the coach can place this current ‘ability-to-perform’ into the performance context of the upcoming opposition, event/match conditions, stage of the season, importance of the competition, impact on later competitions and the ability of potential replacements.

{kind=link}
The size of the contributing circles to the shared decision-making (SDM) processes are influenced by different factors, including health status, participation risk and other decision modifiers. The position of the SDM circle might therefore vary: for a concussed athlete with ‘no capacity’ to take part in the SDM process, the decision is firmly within the healthcare professional circle. In the case of the athlete and coach travelling alone to a training camp/competition, the healthcare professional might be absent from the SDM process.
Whether SDM improves athlete health or performance outcomes has not yet been studied. But SDM improves satisfaction and reduces decisional conflict in healthcare.6 Coaches can influence injury occurrence through load management, implementing appropriate prevention strategies and optimising the athlete's technique.7 ,8 Coaches can also contribute to the athlete wisely addressing contextual factors (ie, sponsors/media) with respect to RTP (and this may influence the athlete's RTP attitudes and decisions).
The healthcare professional's role is objective—to accurately inform the athlete and coach about health status and risk. The athlete and coach ultimately evaluate the information and make a decision about RTP. Successful SDM depends on effective communication within performance teams; clear and consistent, ongoing communication is vital to achieve trust among the key people involved, and ultimately, the quality RTP decision.
For more information on shared decision-making, see the suggested reading list in the online supplementary appendix.
Supplementary appendix
Footnotes
Twitter Follow Hendrik Dijkstra at @DrPaulDijkstra, Noel Pollock at @drnoelpollock, Clare Ardern at @clare_ardern
Contributors HPD substantially contributed to conception and design, coordinated authors, drafted, revised and approved the final version of the manuscript. NP, RC and CLA participated in drafting and revising the manuscript and approved the final version to be published.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.