Article Text

Statistics from Altmetric.com
There has been recent discussion in the journal regarding the pathophysiological mechanisms of the development of tendinopathy.1 2 To date there has been no discussion on the role of the enveloping fascia in this condition. In other related musculotendinous conditions, there is evidence that inflammation of the fascia occurs, for example, in plantar fasciitis.3 Histological examination of this condition demonstrates a reactive-type inflammatory infiltrate with accompanying proteoglycan production and oedema seen with collagen thickening. The process is well demonstrated more diffusely in eosinophillic fasciitis, a rare scleroderma-type condition first described in 1974 by Shulman,4 which has a wide and varied clinical presentation.
Cook and Purdam1 propose a model of tendinopathy beginning with reactive change, although with no inflammatory component, which in turn leads on to tendon disrepair and ultimately tendon degeneration. What may well be missing is the “progenitor” stage, and by ignoring the potential role of the fascia and the fascia–tendon interface, we are potentially missing a critical aspect of this condition.
The gross fascial anatomy of the lower limb is poorly documented, other than the specific fascial attachments of the lateral side of the knee,5 medial knee6 and prepatellar structures.7 There are numerous theories as to the function of the lower limb fascia. A tension or rigging effect has been demonstrated in the lumbar fascia,8 9 but no similar proposal has been made in the lower limb. Alternatively, the crossover of fascial force transmission to contralateral limbs has been proposed by Vleeming and colleagues,10 and has the fibre orientation of fascia in its support, and finally the hydraulic amplifier effect11 of longitudinal muscle tension is an alternative theory.
None of the current papers on tendinopathy make reference to this anatomically important structure, but the plethora of recently cited papers with new therapeutic interventions for Achilles tendinopathy all make reference to the existence of a paratenon either surrounding or overlying the Achilles, which is often used to guide the injected component into the purported therapeutic delivery zone. A recent paper on ultrasound examination of the Achilles makes direct reference to this paratenon.12 In particular, high-volume saline injections,13 14 polidoconol injections15 16 and hyaluronic acid17 are described being injected into this subparatenon space.
During anatomical dissection of 22 embalmed and 10 fresh cadaveric lower limbs at the University of Melbourne, in the course of a complete examination of the fascia of the lower limb, the authors revisited the anatomy of the fascia around the Achilles tendon.
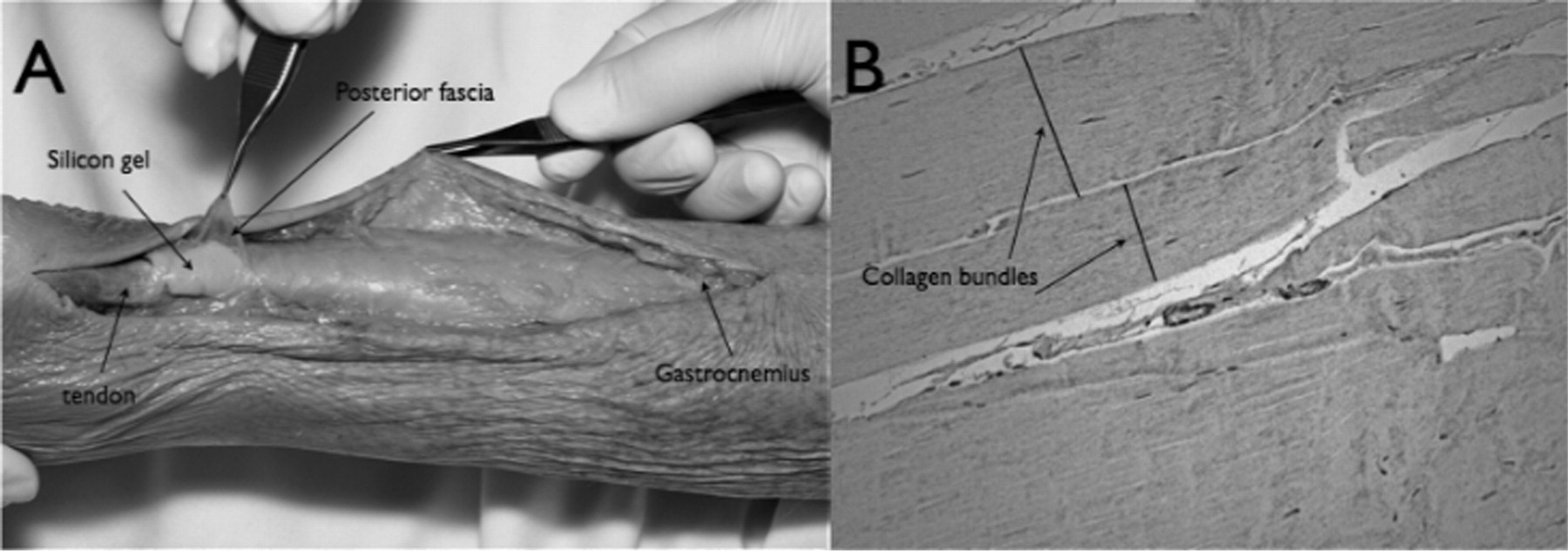
There was no evidence of a discrete structure independent of the fascia of the posterior compartment of the lower leg. This paratenon is in fact the posterior fascia of the lower limb. This was confirmed histologically, being made up of similar collagen bundles as the fascia overlying the gastrocnemius and peroneal compartments and of similar thickness and density. Further to this, the authors performed a needle dilatation using silicon latex under ultrasound guidance of the “paratenon space”, and then dissected the specimen to confirm that this was subfascial (fig 1).
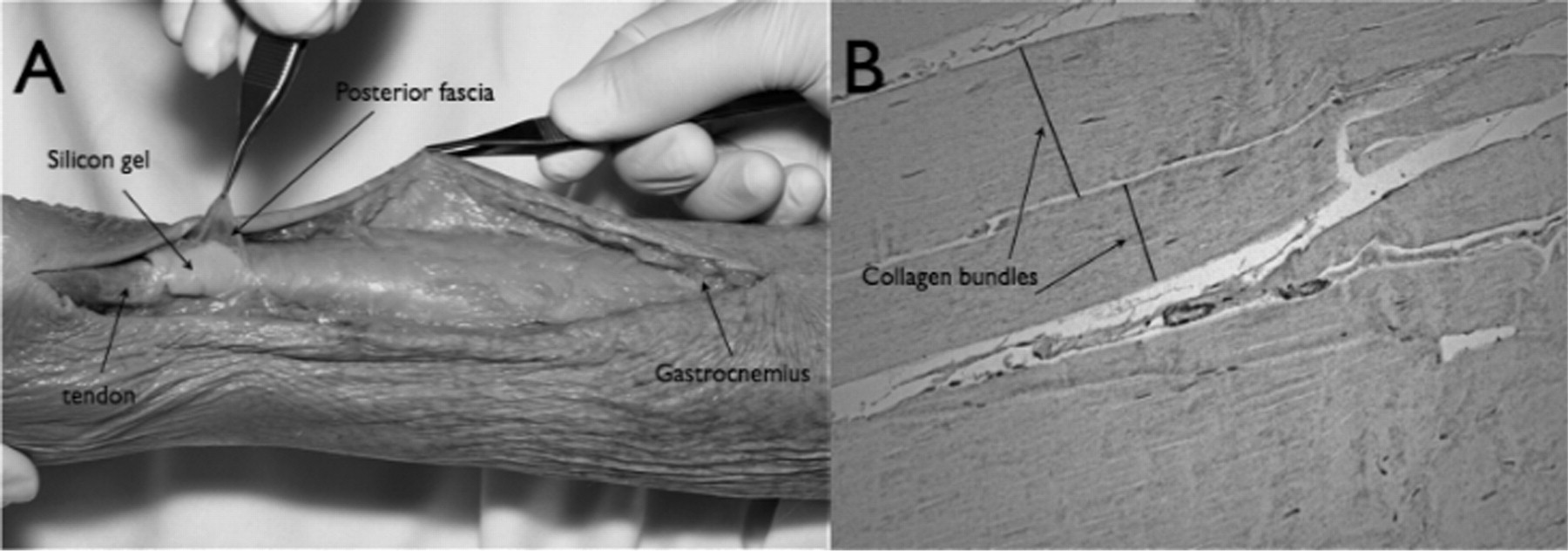
(A) Fresh cadaver dissection demonstrating silicon introduced subfascially, enveloping the gastrocnemius and the Achilles tendon (B) Histological image of posterior fascia (Leica Dm 4500B microscope at ×20 000 magnification, photographed using a Minolta 5000).
Ultrasound images confirm the space location, which was seen to track superiorly to surround the gastrocnemius (fig 2).

{kind=link}
{kind=link}
Ultrasound images of the achilles tendon (TA) and overlying fascia after the introduction of saline into the subfascial space (SFS).
Current papers on neovascularisation, neo-innervation15 and indeed new treatment interventions13 14 15 16 17 can be interpreted more accurately if there was an initial inflammatory process. If the posterior calf fascia, hitherto known as the “paratenon”, is the source of this initial inflammation, then this could be the source of the pain seen in the early stage (prereactive) and these changes leading to the identified neovascularisation around the tendon. Adhesions seen in eosinophillic fasciitis, which develops grossly thickened fascia and fibrosis, are indicative of the potential for fascial inflammation to cause adhesions. Adhesion of the underlying tendon to an inflamed painful fascia may be the precursor to abnormal loading of the tendon and subsequent tendinopathy.
By accurately describing the anatomy we can more effectively understand the role of current and potential interventions. As discussed earlier, there are many proposed treatments, which rely on the introduction of agents between the tendon and the fascia. Perhaps more excitingly, in those with refractory symptoms, Eklund and colleagues18 report on the successful use of infliximab in a patient with refractory plantar fasciitis. This alone suggests that the process is not entirely degenerative and that further work needs to be directed at this interface.
Is there a window where local therapeutic agents or systemic interventions might be appropriate in the athlete, and can the progressive condition be stopped in its tracks at the first sign by a disease-modifying antirheumatic drug such as anti-tumour necrosis factor alpha? Of course we are then into the realms of the World Anti-Doping Agency, but when a drug has a genuine benefit to the patient then its use could be justified, could it not?
Acknowledgments
The authors would like to acknowledge Associate Professor Christopher Briggs and the staff of the Cell Biology and Anatomy Department of the University of Melbourne for their assistance.
REFERENCES
Footnotes
Competing interests None.