Article Text

Statistics from Altmetric.com
- Heart
- athlete
- exercise physiology
- ventricular remodelling
- sports
- systolic dysfunction
- diastolic dysfunction
- systolic heart failure
- echocardiography
- cardiac function
- stress
- pulmonary arterial hypertension
Athlete's heart is the term given to the complex of structural, functional, and electrical remodelling that accompanies regular athletic training. It is an important physiological adaption which helps athletes perform better in physical tasks than non-athletes and one of the physiological changes that may make a good athlete great. The fact that the heart of an athlete is different to the non-athlete's was recognised in the late 19th century based on clinical examination, with the recognition of cardiac enlargement and bradycardia among more highly trained athletes. Our understanding of this syndrome has gradually expanded in parallel with the development of new invasive and non-invasive tools for the examination of cardiac structure and function. Initially, the chest x-ray and ECG demonstrated important features of cardiac chamber enlargement in athletes. The next steps incorporated invasive haemodynamic measures at rest and with exercise. An additional source of understanding of the athlete's heart has been examination of cardiac pathology specimens. More recently the use of imaging techniques such as echocardiography and cardiac MRI have played a central role in advancing our understanding of what constitutes an athlete's heart and in applying this information in clinical settings.
Study of the athlete's heart has been undertaken and is important for a number of key reasons: first, to understand how cardiac adaptation contributes to improved athletic performance; second, to guide development of training regimens which will optimise cardiac adaptation and thus enhance athletic performance; and third, to allow differentiation of the normal athlete's heart from important disease states which may share similar morphologic features. It is the third of these reasons that has assumed most importance in the cardiology and sports medicine worlds.
The aim of this article is for clinicians to learn about the key features of the athlete's heart and to understand concepts used to differentiate normal findings in an athlete from the presence of cardiac pathology such as hypertrophy cardiomyopathy (HCM), dilated cardiomyopathy (DCM), and arrhythmogenic right ventricular cardiomyopathy (ARVC) when faced with a specific clinical scenario. The process of cardiac remodelling will be examined as will the limits of what may be considered normal cardiac structure and function in an athlete.
Effect of exercise on the heart
Different forms of exercise impose differing loads on the cardiovascular system. A variety of terms have been used to describe this, but, put simply, pure endurance sports tend to place a high dynamic (isotonic) load on working muscles, and pure strength sports place a high static (isometric) load on the muscles. Dynamic exercise results in increased cardiac output through increases in heart rate and stroke volume, reduced peripheral resistance and a moderate increase in systemic blood pressure. Thus the load to which the heart is subjected is predominantly a volume load (figure 1). In contrast, the major physiological change with static exercise is a pronounced increase in both systolic and diastolic blood pressure accompanied by only small increases in heart rate, stroke volume, and cardiac output. Thus, the major load is that of pressure. The differential effects of pressure and volume loading during training was first documented in the seminal work by Morganroth,1 in which it was identified that although all athletes had increased left ventricular (LV) mass, in swimmers and runners the major finding was of increased LV dimensions while in wrestlers the major finding was of increased wall thickness. Although a dichotomous effect of exercise on cardiac structure would be convenient, most sports are not solely dynamic or static in the load they impose on the heart. Sports themselves may vary in the proportion of each of these components and can therefore be classified by the relative requirements for static (strength) and dynamic (endurance) demands,2 and this is summarised in table 1.
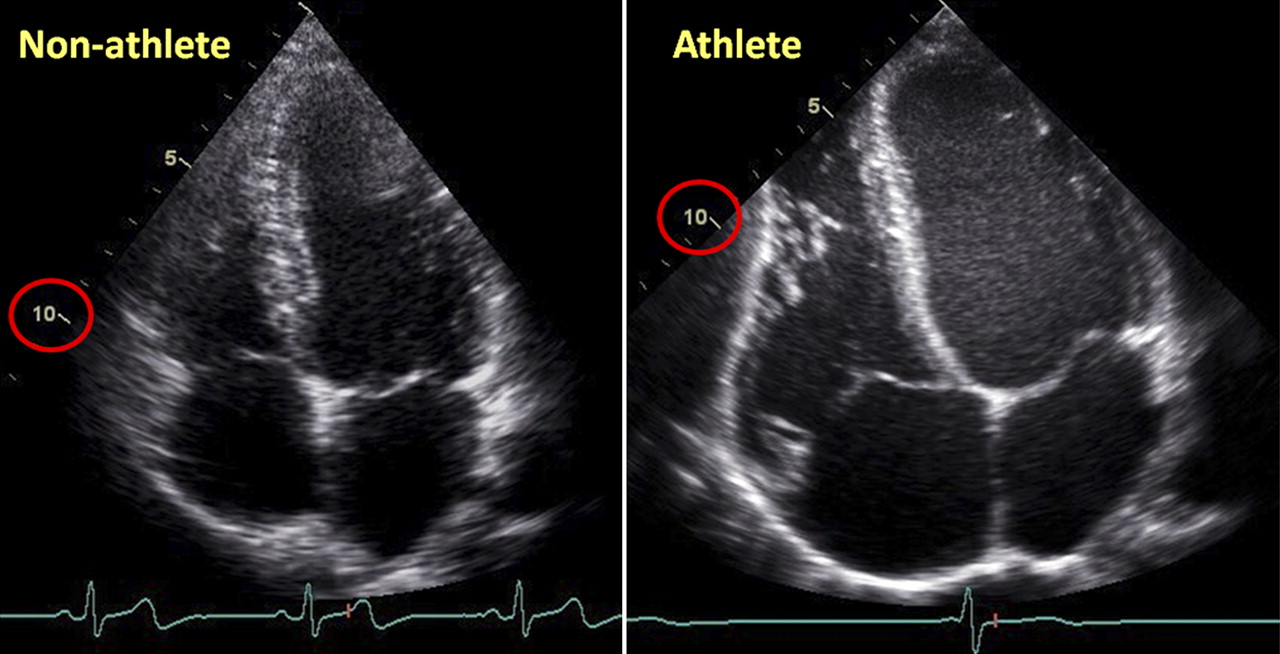
Apical four chamber echocardiogram comparing the heart of a 23-year-old non-athlete (left) with that of a 23-year-old professional cyclist. The volume load of endurance sport training results in dilation of all four cardiac chambers and a notable increase in stroke volume despite normal or even reduced resting function. In this case, a normal cardiac output is maintained at rest in spite of a pronounced bradycardia (heart rate 28 beats/min). The 10 cm echocardiographic field depth is marked in red to highlight the differences in cardiac size.
Classification of training type by sport (adapted from Mitchell et al2)
Structural remodelling
Left ventricle
Numerous studies examining the structural changes in the LV of athletes have defined changes common to all forms of training in addition to those which may differ between different sports or types of training. Some difficulties in interpretation of the literature result from the fact that many studies of athlete's heart involve discrete groups of athletes undertaking only one specific form of exercise, and the intensity of activity may also vary. This makes direct comparison of these studies problematic.
As previously outlined, the hallmark of all forms of athlete's heart is hypertrophy of the LV which may be eccentric or concentric in nature. Building on the work of Morganroth,1 Fagard3 and other investigators, an extensive meta-analysis by Pluim et al, published in 2000, examined changes in parameters of LV structure, comparing endurance trained athletes, strength trained athletes, and combined strength and endurance trained athletes with non-athletic controls.4 They found that LV mass was increased in all groups of athletes compared to control subjects, with no difference in LV mass between the three groups of athletes. Although it is usually assumed that strength trained athletes who may generate very high blood pressures during training would develop a concentric pattern of LV hypertrophy (LVH) with small cavity dimensions, increased LV mass and wall thickness, the available evidence does not support this. Strength trained athletes in fact have LV cavity sizes that are similar or slightly larger than sedentary controls,1 4 although wall thickness relative to cavity size does tend to be higher than controls and endurance athletes. This may be useful in differentiating athlete's heart from HCM, in which cavity sizes tend to be small, and it has been suggested that a cavity size <45 mm strongly favours a diagnosis of HCM.w1
Right ventricle
In endurance trained athletes, the right ventricle (RV) is subjected to the same volume load as the left side, and increased RV volume, mass, and stroke volume have all been observed in athletes, largely based on measurements using cardiac MRI. The phenomenon of balanced dilation of the RV, similar to increases in LV volume, has been described in these athletes.5 6 w2 Although recent work has suggested that the RV may remodel slightly more than the LV in endurance athletes7—possibly reflecting the fact that although the volume load during exercise is the same, RV wall stress increases more than LV wall stress during exercise, thus placing an additional pressure load on this ventricle—this difference is small. Other research has suggested that the common ECG changes seen in athletes of incomplete and complete right bundle branch block (RBBB) reflect the degree of RV remodelling, even in the absence of significant structural heart disease.w3 There has been little work on RV changes in athletes engaged in static exercise, although one study observed increased RV volume in sprinters,w4 a finding which requires further study. The challenge in clinical practice has been to measure RV size accurately due to the complex three dimensional structure of this chamber, although the use of cardiac MRI and three dimensional echocardiography may make this more practicable in the future (figure 2).

Cardiac MRI enables visualisation (and volumetric quantification) of both ventricles. There is currently some debate as to whether the right ventricle (RV) dilation is proportionally greater than the left ventricle in endurance sports. In these examples, the RV is more prominent in the runner and cyclist and, as is commonly seen, the free wall bulges below the lateral tricuspid annulus (arrows). In these horizontal long axis views, the constraint on cardiac enlargement posed by the thorax is readily appreciable. In the marathon runner, the sternum and ribs border the entire RV and the left atrium is constrained by the thoracic spine.
Atria
In addition to remodelling of the LV and RV, studies have shown atrial enlargement to be frequent in trained athletes whether identified by dimensionsw5 or volumetric measures.w6 Most studies have examined the left atrium, although right atrial enlargement has also been described. In general, atrial enlargement is proportional to the enlargement of the ventricles and is affected by the type of training undertaken. There is some speculation that atrial enlargement may not regress completely after cessation of athletic activity and may predispose athletes to an increased risk of subsequent atrial fibrillation.
Functional remodelling
Left ventricle
While structural change within the LV has been very clearly and consistently demonstrated, the evidence regarding functional change has been less consistent.8 Compared to pathological LV remodelling which is frequently associated with reduced systolic and/or diastolic function measures, athlete's heart has been demonstrated to have preserved or even enhanced function. Most functional studies have used echocardiography and a small subset have used cardiac MRI. LV ejection fraction (LVEF) is the most common measure of systolic function used and athletes generally have values for LVEF which are close to the general population. The exception to this may be those endurance athletes with notably dilated left ventricles who may have an LVEF which is ‘lower than normal’, and resting values as low as 41% have been documented in otherwise normal athletes, although stroke volume is normal. One study of professional cyclists reported that 11% of study participants had an LVEF <52%.9 A low LVEF was generally associated with more significant LV enlargement suggesting that in these dilated hearts, less vigorous contraction is required to maintain a normal stroke volume at rest, although other studies have shown normal, or even supra-normal augmentation of the LVEF during activity.10 w7 The difficulty arises in differentiating a dilated heart with an LVEF below the normal range from a DCM if the heart is only studied at rest, and stress echocardiography may be useful in this setting to confirm normal augmentation with exercise.
Recently, attention has focused on direct measures of myocardial function such as tissue velocity, strain and strain rate for assessment of both systolic and diastolic function. Some researchers have found evidence of enhanced systolic myocardial function at restw8 in athletes, but this has not been universal.w9 w10 Similarly, studies of myocardial function during exercise have also been somewhat heterogeneous, possibly reflecting variable methodology; at present, until the factors underlying the variability in findings are elucidated, these are not considered routine in the clinical assessment of the athlete's heart. These direct measures of myocardial function may, however, prove to be very useful in the future.
In general, studies of diastolic filling have confirmed that the structural remodelling seen as part of the athlete's heart is not associated with impairment of diastolic filling. In fact, Levine et al11 eloquently described improved LV chamber compliance in athletes, as compared with non-athletes, by means of lesser increases in pulmonary artery capillary wedge pressure for a given increase in end-diastolic volume—that is, athletes seem to be able to distend their ventricles and thus recruit the Frank-Starling mechanism more effectively. However, a prospective test of this principal was not as evident when a 1 year intensive training regimen failed to demonstrate an increase in LV compliance.w11 Teske et al have also challenged the notion of superior LV filling characteristics by demonstrating that echocardiographic measures of diastolic function did not differ between athletes and non-athletes, regardless of age.w12 Thus, filling of the athlete's ventricle is often brisk due, at least in part, to the fact that the chamber is larger. The extent to which intrinsic lusitropic properties of the myocardium add to enhanced filling remains to be determined.
Right ventricle
There have been fewer studies examining myocardial function of the RV. Similar to the LV, RV ejection fraction is frequently in the low-normal or mildly abnormal range if there is significant cardiac enlargement.7 Erol et al12 reported that RV systolic and diastolic myocardial velocities were similar in athletes and non-athletes, while an eloquent study in a large cohort of elite athletes recently demonstrated that RV deformation was reduced in well trained athletes when compared with untrained subjects, particularly in the basal segments and among those athletes with greater RV chamber dilationw13 (figure 3). The significance of these findings remains to be determined. Like ejection fraction, the reduced deformation may simply reflect the reduced work required of the enlarged RV to generate the same stroke volume at rest. Ambiguities may be resolved by studying RV function when under the exercise demands of increased pressure and volume load.

An example of right ventricular free wall strain imaging using colour coded tissue Doppler imaging. Peak systolic strain is relatively reduced in the basal segment of this healthy endurance athlete's heart as has been described by Teske et al.w12 Of note, there is also post-systolic shortening with the peak shortening occurring later than the more apical segments and after aortic valve closure.
Electrical remodelling
In addition to structural and functional remodelling, it is recognised that there is electrical remodelling of the athlete's heart in response to training, resulting in distinct changes in the ECG. It is important for the clinician to be able to correctly identify those changes which result from intense physical training and do not carry an increased risk of adverse cardiac outcomes, in addition to identifying ECG changes which are associated with underlying cardiac diseases and may result in cardiac events, the risk of which may be increased by participation in sport.w14 HCM, ARVC, and the channelopathies represent some of the pathologies most frequently associated with sudden cardiac death in athletes aged <35 years, with HCM being most common. ECG changes frequently precede the phenotypic structural changes of HCM and ARVC and may be the sole marker of an increased risk of sudden cardiac death early in the disease process. The channelopathies (long and short QT syndromes, Brugada syndrome, and catecholaminergic polymorphic ventricular tachycardia (VT)) are seldom associated with morphologic abnormalities, and diagnosis depends upon the identification of characteristic ECG changes and/or familial history. Based on this rationale, preparticipation screening of competitive athletes is mandated in many countries and sporting competitions, and frequently includes an ECG in addition to a clinical assessment. Accurate interpretation of the ECG, in the light of known changes of electrical remodelling seen with the athlete's heart, will result in less unnecessary investigation and exclusion of athletes based on ECG abnormalities which may be considered acceptable in an athlete.
The most commonly observed forms of electrical remodelling include sinus bradycardia, sinus arrhythmia or first degree atrioventricular (AV) block, largely due to high vagal tone at rest. The European Society of Cardiology recently published guidelines for interpretation of the 12 lead ECG in the athlete. These guidelines provide a clinically useful classification of ECG abnormalities into: those which are considered common and related to training, and are therefore part of the spectrum of electrical remodelling in the athlete's heart; and those which are uncommon and training unrelated, and should prompt examination for underlying cardiac pathology.13 This document provides a very practical framework for evaluation of electrical remodelling. In short, sinus bradycardia, first degree AV block, incomplete RBBB, early repolarisation and voltage criteria for LVH may be considered normal electrical remodelling of the athlete's heart. Some of these reflect the underlying structural remodelling such as development of LVH.w14 Other abnormalities such as T wave inversion, complete bundle branch blocks, and left atrial enlargement on ECG are not regarded as training related changes reflecting a normal athlete's heart, and further evaluation for pathology is recommended (table 2).
ECG findings considered normal and abnormal for the athlete's heart (adapted from Corrado et al13)
There is, however, variability in what constitutes normal electrical remodelling based on gender, race, and type of training. There may also be interaction of these factors. Compared to female athletes, male athletes have a much higher prevalence of abnormal ECG findings that may reflect, but are not diagnostic of, cardiac disease.w15 Normal black athletes have a higher prevalence of voltage criteria for LVH, ST segment abnormalities, and deep T wave inversion than both male14 w16and female15 white athletes. Endurance training has been associated with a higher rate of ECG changes than non-endurance sports.w15 It should be noted, however, that many athletes with ECG changes considered abnormal which are detected at screening and requiring further cardiac assessment are found to have no underlying structural cardiac disease, and the ECG changes are therefore part of the athlete's heart phenotype for that individual.w15
Other factors which may impact on the athlete's heart
How much training is required to develop an athlete's heart
Most studies of the athlete's heart on which our understanding of the normal phenotype is based are conducted in elite amateur or professional athletes and generally reflect high levels of training. In clinical practice, a cardiologist is often asked to see a recreational athlete with ECG or cardiac structural parameters which fall outside of the limits of normality for a non-athlete, but are within normal limits for an athlete. Whereas findings in an elite athlete may confidently be ascribed to athlete's heart, the question which must then be addressed in a recreational athlete is whether the findings for this individual reflect an athlete's heart or reflect pathology—that is, do they train enough to develop an athlete's heart. There has been surprisingly little research in this area and at present, from a single study of 127 males, it appears that changes of athlete's heart—comprising lower resting heart rate, increased peak Vo2, and increased LV mass—are only seen in those individuals performing more than 3 h of exercise per week.16 Recent studies have shown a very strong association between cardiac MRI derived measures of cardiac volumes, cardiac mass, and Vo2max across a wide range of athletic conditioning, suggesting that athlete's heart should be considered as a continuum.w17 w18 This may be clinically useful in evaluating whether a degree of remodelling can be attributed to athletic conditioning, in that a Vo2max test, or even a Bruce-protocol stress test (given that exercise tolerance is associated with Vo2) may confirm a high level of fitness and provide reassurance in a subject with an enlarged heart.
Racial variability
It is apparent that genetic and racial variability affect the individual's cardiac response to exercise training such that different limits of normality may need to be applied depending on an athlete's background. Athletes of Afro-Caribbean background tend to have increased LV mass and wall thickness when compared to white athletes. In fact, the normal distribution of these parameters in Afro-Caribbean athletes is shifted to the right such that these athletes may have wall thickness up to 15 mm.14 In Basavarajaiah's study, 25% of black athletes had LVH based on an end-diastolic wall thickness >12 mm, compared with only 4% of white athletes. Black athletes of East African origin, on the other hand, show a lower frequency of LVH than those of West African ancestry. There are only limited data in other racial groups such as Asians or the indigenous populations of many countries, despite such populations being disproportionately well represented in some elite sports.
Effects of detraining
Upon cessation of training, the changes of athlete's heart may regress towards more normal structure.17 This has been advocated as a useful method for discrimination of the true athlete's heart from a structurally abnormal heart due to cardiac pathology, in which the expected regression with detraining will not occur. Regression of changes has been not only with structural, but also with electrical remodelling.w19 There is some evidence to support this approach, although there is conjecture about whether longstanding changes of athlete's heart in an older athlete will regress as effectively as in a younger athlete.
Mechanisms of remodelling
Athlete's heart is an adaptive response to exercise training which imposes an intermittent volume and pressure load. This remodelling response to an exercise stimulus is often termed ‘physiological’ in contrast to the hypertrophic response which results from pathological entities such as systemic hypertension, valvular heart disease and cardiomyopathy. In both cases, an increase in cardiac load activates a variety of molecular mechanisms, activates ribosomal kinases and increases protein synthesis which are necessary for an increase in muscle mass. However, the molecular mediators of ‘pathological’ hypertrophy (natriuretic peptides, vasoactive hormones and catecholamines) are quite different from those which mediate hypertrophy in athletes (trophic hormones such as insulin-like growth factor), possibly as a result of the chronic versus intermittent nature of the load excess.18 w20 Pathological hypertrophy includes cellular apoptosis, expansion of pro-fibrotic elements and frequently progresses to cardiac dysfunction whereas the increase in myocyte mass is relatively ‘pure’ in athletes with minimal or no increase in extracellular expansion. Microarray techniques have been used to demonstrate the differences in gene expression between hypertrophy resulting from physiological and pathological stimuli,w21 although the separation remains incomplete and some investigators have argued that the distinction is somewhat arbitrary.w22
Is the athlete's heart always benign and reversible?
Physiological hypertrophy implies that muscle mass has the capacity to both increase and decrease in response to changes in load. Indeed, de-training leads to regression of cardiac hypertrophy and can be a clinically useful tool when attempting to separate athlete's heart from structural heart disease. However, normalisation of cardiac mass may not always be complete, even after many years of deconditioning.17 w23 This seems particularly true of well practised athletes who have developed profound cardiac hypertrophy over many years. The lack of longitudinal studies detailing cardiac morphology before athletic conditioning means that one cannot exclude the possibility that these athletes who do not regress to the normal range had enlarged hearts before sports training (perhaps conferring a performance advantage). However, excluding this hypothesis, the lack of normalisation infers that athletic cardiac hypertrophy may, at least in some athletes, result in expansion of the extracellular matrix—a proposition with some support from recent reports of abnormal regions of delayed gadolinium enhancement on MRI (a marker of fibrosis) within the myocardium of athletes who had been intensively training for many years19 w24 (figure 4). A recent study reported inflammatory and pro-fibrotic cellular infiltrates among the myocardium of intensively trained ratsw25 and a resulting increase in susceptibility to ventricular arrhythmias. Recent accumulating evidence suggests that competitive endurance sports over many years may constitute a risk factor for atrial arrhythmias, and interested readers are referred to a recent review by Montw26 for further detail. Thus a degree of controversy persists. Although the prognosis in athletes with cardiac hypertrophy appears distinct from those with hypertrophy associated with clinical pathologies, it remains possible that there may be some overlap.

Delayed gadolinium enhancement (DGE) can be used to identify regions of fibrosis within an athlete's myocardium. The clinical significance of small regions of septal DGE, especially at the mechanical ‘hinge points’ of the right ventricle insertion, is uncertain. Here a healthy world class triathlete (A) and a recreational marathon runner with complex ventricular arrhythmias (B) demonstrate an almost identical pattern of DGE.
Identifying structural heart disease in athletes
As detailed above, there is significant overlap in the phenotypic characteristics of the normal athlete's heart and important underlying diseases associated with sudden death during exercise such as HCM, DCM, and ARVC. Accurate differentiation can be difficult and, for this reason, considerable effort has gone into defining the limits of normality in parameters which can be used to reliably differentiate the normal athlete's heart from a cardiomyopathic heart.
There is ongoing debate regarding precisely where the limits of normality should be set, and as new imaging modalities with less variability such as cardiac MRI are more frequently used, it is likely that these limits may be further modified. As a doctor, the question which must often be answered is whether the findings in an individual athlete are within the expected limits of normal for that athlete. Thus, when assessing the individual athlete, it is important to consider measures of cardiac structure and function and their normal ranges in light of important factors known to affect cardiac adaption which have been discussed above, such as age, gender, race, and body size.
In the athlete undertaking predominantly static exercise with an abnormal ECG and possibly an echocardiogram with increased LV wall thickness, an athlete's heart must be differentiated from HCM. Appropriate information about symptoms and family history must be sought, but in differentiating athletes with physiological hypertrophy from those with HCM the most common parameters examined are LV wall thickness and cavity size. Whereas the upper limit of wall thickness in non-athletic subjects is 12 mm by echocardiography, studies have shown that a proportion of normal athletes may have septal wall thickness in excess of this. Work by Pelliccia et al20 suggested that a wall thickness ≥13 mm is very uncommon in Caucasian athletes, a finding supported by subsequent studies from Sharma et al in adolescent athletes.21 As noted earlier, a wall thickness of up to 15 mm may be normal in some athletes of Afro-Caribbean descent.14
In the athlete undertaking predominantly dynamic exercise or combined exercise, the finding of a dilated LV, possibly accompanied by a ‘low’ ejection fraction, must be differentiated from a DCM. Exercise testing with imaging to document exercise capacity and ventricular response to exercise may be useful in this context, with the cardiomyopathic heart being unable to augment adequately during stress testing. Further assessment of structure with cardiac MRI to characterise the myocardium and to look for late gadolinium enhancement may be useful in selected cases. In the athlete with disproportionate enlargement of the RV, a diagnosis of ARVC should be considered. Original or revised Task Force criteria should be applied, and although cardiac MRI may be useful for more detailed assessment of both RV and LV volume and structure, imaging may only provide one major criterion towards diagnosis and is not sufficient by itself. Careful examination of the ECG, a detailed family history, and in some cases endomyocardial biopsy may be required for a definitive diagnosis. Published normal ranges for measures used to separate athlete's heart from cardiac pathology are listed in table 3 and a possible assessment algorithm is shown in figure 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow chart for evaluation of the athlete's heart. †Type 1 ECG changes are those considered normal for an athlete, and type 2 ECG changes are considered abnormal.13 ARVC, arrhythmogenic right ventricular cardiomyopathy; DCM, dilated cardiomyopathy; EF, ejection fraction; EP, electrophysiology; HCM, hypertrophic cardiomyopathy.
Implications
The athlete's heart phenotype is a wonderful example of physiological adaptation to the demands placed upon it by training and competition. By understanding the relationship between factors such as the sporting discipline, the training volume, gender and race, and the resulting structural, functional, and electrical remodelling, we can more reliably differentiate the normal athlete's heart from pathological remodelling which may occur as a result of an inherited or acquired cardiomyopathy. Although the differentiation is easy in many cases, it is the role of the clinician to integrate all these factors and decide whether the degree of remodelling is most consistent with physiological or pathological change. Whether the athlete's heart is entirely a benign and reversible entity remains a topic of some conjecture and is likely to be addressed by further studies in the athlete population with new and more sophisticated methodology. These unanswered questions remain important as exercise remains a useful lifestyle intervention capable of prolonging life and increasing wellbeing in our community.
The athlete's heart: key points
Structural and functional remodelling
Regular exercise training results in left ventricular hypertrophy.
The cellular mechanisms of physiological hypertrophy differ from the mechanisms of pathological forms of hypertrophy.
The pattern of remodelling varies with the type of training: dynamic exercise causes eccentric hypertrophy with increased left ventricular cavity dimensions, static exercise causes concentric hypertrophy with near-normal cavity dimensions, and exercise with significant dynamic and static loads causes a mixed pattern of hypertrophy.
The limits of hypertrophy vary by gender and race with greater wall thicknesses seen in males and in athletes of Afro-Caribbean descent.
The quantity and type of exercise training need to be considered in deciding whether observed structural remodelling is appropriate for that athlete.
Left ventricular ejection fraction in athletes is generally within the same normal range for non-athletes (apart from those with very dilated hearts in whom the ejection fraction is often mildly reduced).
Electrical remodelling
Normal electrical remodelling in the athlete's heart reflects increased parasympathetic tone, reduced sympathetic tone and cardiac chamber hypertrophy.
Sinus bradycardia, first degree atrioventricular block, incomplete right bundle branch block, early repolarisation and isolated voltage criteria for left ventricular hypertrophy are common features of normal electrical remodelling in the athlete's heart and do not usually require further evaluation.
Widespread T wave changes, abnormal cardiac axis, complete bundle branch blocks, left atrial enlargement, pre-excitation, and pathological Q waves are not normal features of the athlete's heart and should prompt further evaluation.
Common clinical dilemmas
A small left ventricular cavity with increased wall thickness should raise suspicion of hypertrophic cardiomyopathy.
Disproportionate enlargement of the right ventricle should raise suspicion of arrhythmogenic right ventricular cardiomyopathy.
Excessive dilation of all cardiac chambers with low ejection fraction and failure to augment normally with exercise should raise suspicion of dilated cardiomyopathy.
Reversal of remodelling through detraining may help to determine whether an observed structural abnormality is due to the athlete's heart, although reverse remodelling may be incomplete in some longstanding athletes.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
References
- ↵
- ↵This article reviews circulatory physiology changes during static and dynamic exercise and classifies sports by their relative static and dynamic components.
- ↵
- ↵Large meta-analysis of cardiac structural and functional changes in athletes from a variety of sports, showing variation in the pattern of remodelling with different sports.
- ↵This cardiac MRI study supports the concept of balanced remodelling of the left and right ventricles in the athlete's heart.
- ↵
- ↵
- ↵
- ↵The role of imaging in understanding the athlete's heart is reviewed.
- ↵
- ↵
- ↵
- ↵European guidelines for the interpretation of the ECG in athletes, which differentiate abnormalities which are part of the athlete's heart from those which may reflect underlying cardiac disease. A clinically useful guideline.
- ↵Important study which highlights the effect of ethnicity on cardiac structural limits of normality for the athlete's heart.
- ↵This study demonstrates that ethnic differences in the athlete's heart are also seen in female athletes.
- ↵
- ↵Review of the cellular mechanisms of cardiac hypertrophy which highlights the differences between physiological and pathological hypertrophy.
- ↵This study shows that detraining results in reversal of the athlete's heart phenotype; however, the reverse remodelling is frequently incomplete.
- ↵
- ↵Study of almost 1000 athletes to try and define the limits of physiological left ventricular hypertrophy so that abnormal hypertrophy in conditions such as hypertrophic cardiomyopathy could be reliably identified.
- ↵
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online References
Footnotes
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. The authors have no competing interests.
Provenance and peer review Commissioned; internally peer reviewed.