Article Text

Abstract
Background and objectives: FIFA’s anti-doping strategy relies on education and prevention. A worldwide network of physicians guarantees doping control procedures that are straightforward and leave no place for cheating. FIFA actively acknowledges its responsibility to protect players from harm and ensure equal chances for all competitors by stringent doping control regulations, data collection of positive samples, support of research, and collaboration with other organisations. This article aims to outline FIFA’s approach to doping in football.
Method: Description of FIFA’s doping control regulations and procedures, statistical analysis of FIFA database on doping control, and comparison with data obtained by WADA accredited laboratories as for 2004.
Results: Data on positive doping samples per substance and confederation/nation documented at the FIFA medical office from 1994 to 2005 are provided. According to the FIFA database, the incidence of positive cases over the past 11 years was 0.12%, with about 0.42% in 2004 (based on the assumption of 20 750 samples per year) and 0.37% in 2005. Especially important in this regard is the extremely low incidence of the true performance enhancing drugs such as anabolic steroids and stimulants. However, there is a need for more consistent data collection and cross checks among international anti-doping agencies as well as for further studies on specific substances, methods, and procedures. With regard to general health impairments in players, FIFA suggests that principles of occupational medicine should be considered and treatment with banned substances for purely medical reasons should be permitted to enable players to carry out their profession. At the same time, a firm stand has to be taken against suppression of symptoms by medication with the aim of meeting the ever increasing demands on football players.
Conclusion: Incidence of doping in football seems to be low, but much closer collaboration and further investigation is needed with regard to banned substances, detection methods, and data collection worldwide.
- DCO, doping control officer
- EPO, erythropoietin
- FIFA, Fédération Internationale de Football Association
- F-MARC, FIFA Medical Assessment and Research Centre
- hGH, human growth hormone
- IOC, International Olympic Committee
- TUE, therapeutic use exemption
- UEFA, Union of European Football Associations
- WADA, World Anti-Doping Agency
- anti-doping strategy
- prohibited substances
- therapeutic use exemptions
- sanctions
- occupational medicine
Statistics from Altmetric.com
- DCO, doping control officer
- EPO, erythropoietin
- FIFA, Fédération Internationale de Football Association
- F-MARC, FIFA Medical Assessment and Research Centre
- hGH, human growth hormone
- IOC, International Olympic Committee
- TUE, therapeutic use exemption
- UEFA, Union of European Football Associations
- WADA, World Anti-Doping Agency
The ongoing debate and controversies concerning doping (that is, the list of prohibited substances and procedures, and sanctions used in amateur and professional sport) has raised public awareness of a problem that has not been fully appreciated during the rapid development of various sports disciplines.
It is only 38 years since drug testing was first introduced at the1968 Olympic Games in Mexico City following amfetamine and nicotinyl tartrate related deaths of a number of cyclists at the 1960 Summer Olympic Games in Rome and the 1967 Tour de France. Regular doping controls have been conducted since, but these controls have failed to prevent sportsmen and sportswomen from taking performance enhancing drugs both during and out of competition. Regrettably, banned and harmful substances are openly available, even without prescription. Drugs such as nandrolone can be purchased over the internet in unlimited quantities. In recent years, an increasing number of positive samples and cases of so-called recreational drugs, such as marijuana and cocaine, have been observed and need to be addressed accordingly. In addition, media reports may encourage those competing at lower levels of sport to experiment in the use of such substances without considering the possible side effects and medical complications, let alone the legal consequences of their actions.
Sporting associations, including the Fédération Internationale de Football Association (FIFA), have stated that the fundamental aims of doping controls and anti-doping policies are to:
-
uphold and preserve the ethics of sport
-
safeguard the physical health and mental integrity of the players
-
ensure that all competitors have an equal chance.
FIFA introduced doping controls in 1970 to ensure that the results of national and international matches were a fair reflection of the ability of those taking part. The FIFA Sports Medical Committee is responsible for implementing doping controls at all FIFA competitions and also for coordinating with confederations and member associations. The overall management of doping controls is conducted by the FIFA administration (Medical Office and the FIFA Sports Medical Committee).
Over the past 12 years, the FIFA Medical Assessment and Research Centre (F-MARC) has developed a worldwide network of specialists who are involved in the educational process within the confederations and national associations as well as in practical performance of doping controls for national, international, and FIFA competitions. The medical doctors/sports physicians, following their Hippocratic Oath as well as their professional and ethical values, play key roles in FIFA’s long term strategy in the fight against doping. Many of these doctors are also team physicians in their national associations.
The fight against doping in football focuses on education and prevention with regular in-competition and out-of-competition controls. In past years, approximately 15 000 doping controls were performed annually on footballers, with over 20 000 performed in both 2004 and 2005. FIFA articulated its unyielding position in the fight against doping prior to the world cup competition in both 1998 and 2002 (FIFA Magazine May 2002)1 and reinforced its strategy in the FIFA Magazine in March 2004.2
Physicians demonstrated their strong support of the FIFA long term strategy in its fight against doping before the 2002 FIFA World Cup Japan/Korea. The team physicians of all 32 finalists signed a joint declaration in the fight against doping, supporting FIFA’s decision to introduce routine blood sampling to analyse for blood doping and erythropoietin (EPO). This was a firm message to the football community and demonstrated the excellent collaboration and cooperation between the FIFA Sports Medical Committee and the team physicians taking care of the players before and during the competition. The team physicians of all the finalists of the 2006 FIFA World Cup Germany again reinforced the fight against doping with a joint declaration signed on 5 March 2006 to keep this unique event free of doping.
DEFINITION
Doping is defined as any attempt by a player, either themselves or at the instigation of another person such as manager, coach, trainer, doctor, physiotherapist, or masseur, to enhance mental and physical performance non-physiologically or to treat ailments or injury—when this is medically unjustified—for the sole purpose of taking part in a competition. This includes using (taking or injecting), administering, or prescribing prohibited substances before or during a competition. These stipulations also apply to out-of-competition testing for anabolic steroids and peptide hormones, and to substances producing similar effects. Any other prohibited method (for example, blood doping) or manipulation of collected samples is likewise classified as doping.
The detailed definition as related to the anti-doping rule violations is presented in the current FIFA doping control regulations (January 2006).3 Doping contravenes the ethics of sport, constitutes an acute or chronic health hazard for players, and may have fatal consequences.
THE EXTENT AND SCOPE OF DOPING IN FOOTBALL
FIFA is a global organisation that unites over 250 million footballers in 207 countries. Around 40 million of these players are female. Currently, confederations, national associations, or both that fall under FIFA’s management, carry out their own doping controls at the competitions they stage. However, the urine or blood samples, or both must be analysed at laboratories accredited by FIFA/World Anti-Doping Agency (WADA). These laboratories send reports on any “chemically positive” A samples to the member associations, and FIFA headquarters for management and WADA for information. Once the FIFA medical office receives a positive A sample report, it requires follow up information from the national association/confederation in question, or both—that is, the results of the possible B sample decision made by the particular disciplinary committee. If the information is not provided, the FIFA disciplinary committee takes appropriate action. Since the 1994 FIFA World Cup in the USA, the FIFA Medical Office has undertaken stringent registration of analysed samples.
A new doping control policy for FIFA competitions was introduced at the FIFA U-17 World Championship in New Zealand in 1999. Since then, during tournaments, two players from each team are randomly selected to undergo doping tests after each match. Between 1994 and 2005, 3327 doping controls (men and women) were performed during three consecutive FIFA world cups (USA, France, Korea/Japan), two consecutive Olympic games (Sydney, Athens) as well as the last Women’s World Cup (USA, 2003), the FIFA U-19 in Thailand, the FIFA U-17 World Cup in Peru, the FIFA Confederations Cup in Germany, the FIFA Club World Cup in Japan, the FIFA Beach Soccer World Cup in Brazil, the FIFA U-20 World Cup in the Netherlands, and FIFA World Championship in Futsal, Chinese Taipei, as well as during the World Cup 2006 preliminaries. Only four samples tested positive during this period: one for ephedrine and pseudoephedrine in 1994 one for cannabis and one for nandrolone during the FIFA World Youth Championship 2003 held in the United Arab Emirates, and one for ephedrine in Angola. This reflects an overall incidence of 0.12% positive cases over the past 11 years. The extremely low incidence of positive cases during FIFA competitions indirectly confirms the FIFA long term strategy in the fight against doping: that education and prevention play a key role in keeping high profile competitions free of doping.
It can only be assumed that team sports such as football are not as prone to misuse of performance enhancing substances as are individual sports. During the 2004 Olympic Games in Athens, there were 27 positive cases—all in individual athletes and none in any team sport participants. It might be hypothesised that the close collaboration of the team sport medical committees since the 2000 Olympic Games in Sydney, positively influenced the attitude of fairplay among team sports during the Olympic Games in Athens.
Close collaboration between accredited laboratories, the reporting system, and the central control system is an important tool for statistical recording of the extent of doping in football in the future. Although several prominent footballers have tested positive for drugs in recent decades, the true extent of the problem is unknown. Even if we assume that doping is still not a major issue in team sports such as football, any estimation of the problem can be considered as merely an unscientific hypothesis or speculation. To meet the challenges brought about by this situation, FIFA has taken action to develop closer collaboration between the medical committees of the various confederations. In October 1999, the FIFA Sports Medical Committee and the Union of European Football Associations (UEFA) Medical Committee met to discuss the latest sports medicine issues with the aim of not only combating doping but also developing educational programmes designed to meet the fundamental objectives outlined above.
Similar meetings have been conducted between the representatives of the FIFA Sports Medical Committee and the medical committees of the Confederation of North, Central American and Caribbean Association Football (CONCACAF) (North and Central America, 2000, 2001), Asian Football Confederation (AFC) (Asia, 2001, 2002, 2005), and Confederation Africaine de Football (CAF) (Africa, 2003, 2004). During 2005, meetings were conducted with the newly established Oceania Football Confederation (OFC) Sports Medical Committee and Confederación sudamericana de Fútbol (CONMEBOL) with the aim of harmonising doping control procedures, improving the understanding of the scientific background of doping, and enhancing the FIFA network of doping control officers (DCOs) who fulfil educational duties as a part of their responsibilities.
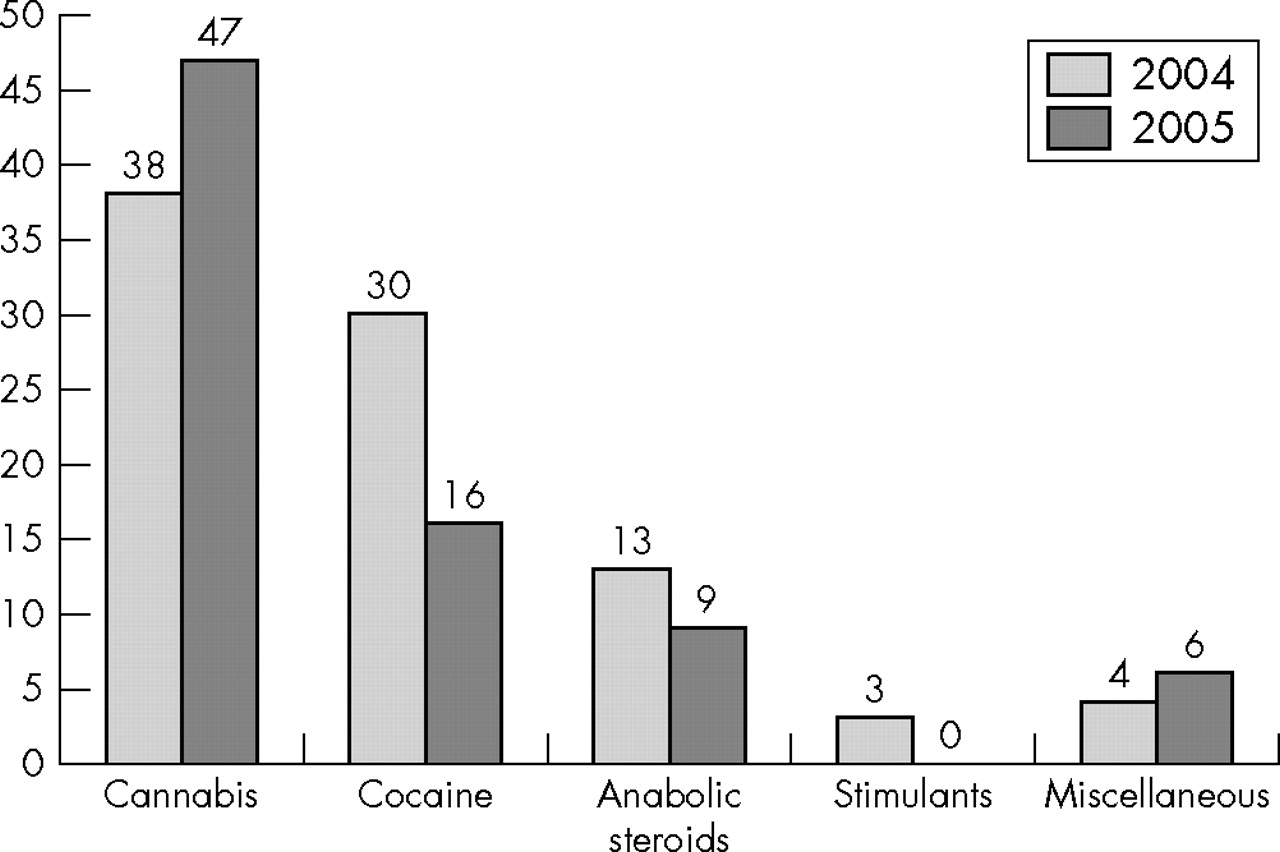
According to the statistics of the International Olympic Committee (IOC) (until 2003) and WADA accredited laboratories (as of 2004), approximately 20 750 doping controls are performed annually on football players. The majority of the controls are done in Europe and North and South America. The numbers of doping controls continue to increase in the other confederations. In this respect, FIFA developed its own database to keep records on the substances being reported as positive to allow online control of management of these samples within the different confederations and member associations. During 2004 and 2005, 88 (0.42% based on the assumption of 20 750 samples per year) and 78 (0.37%) positive samples, respectively, were registered at FIFA (fig 1). The increase is probably because of improved reporting systems used by the laboratories as a result of the implementation of WADA (March 2004). The majority of the positive cases were detected or reported by the European laboratories which receive most of their samples from the European national associations (figs 2 and 3).
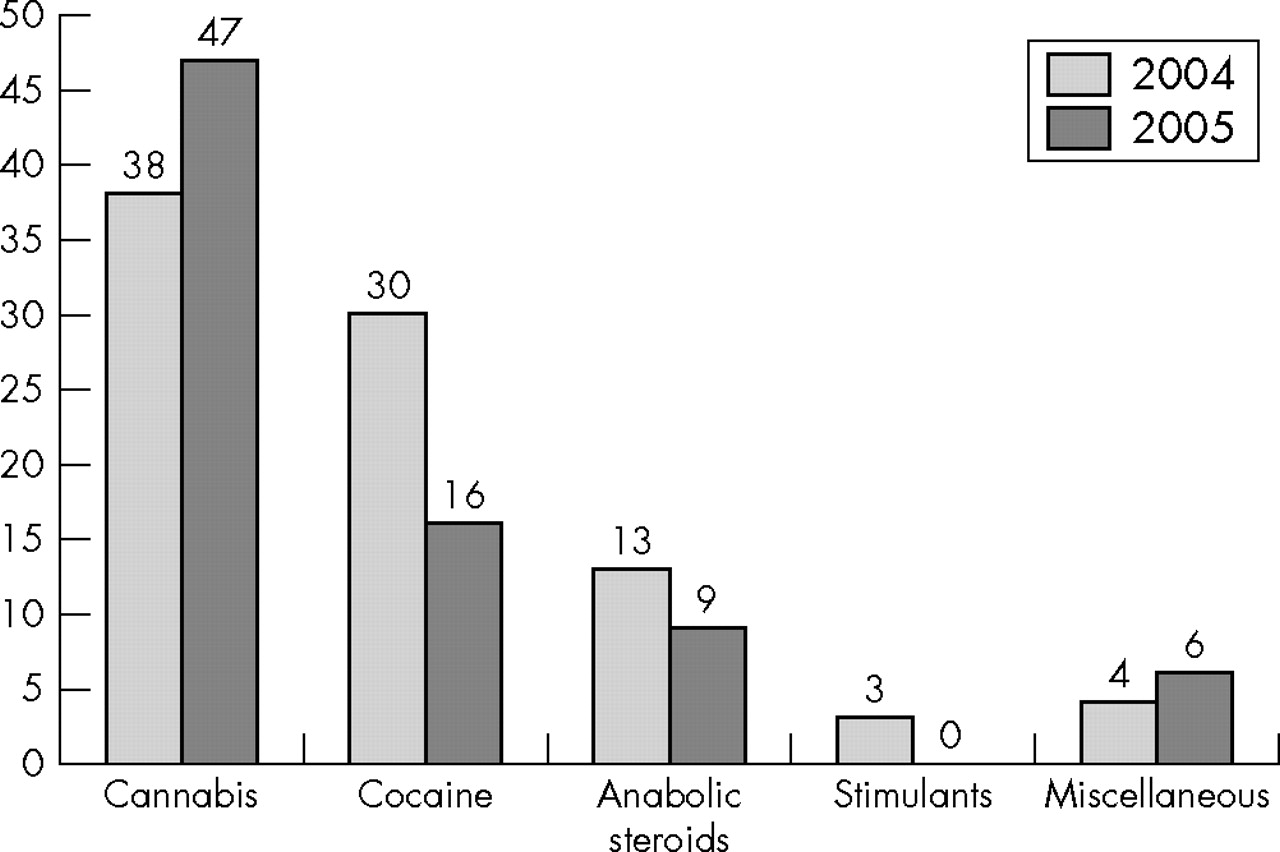
Doping statistics per substance (excluding testosterone/epitestosterone (T/E)): FIFA 2004 and 2005.

Positive doping samples by confederation (excluding testosterone/epitestosterone (T/E)): FIFA 2004 and 2005. See text for abbreviations.

Positive doping samples for Europe by country (excluding testosterone/epitestosterone (T/E)): FIFA 2004 and 2005.
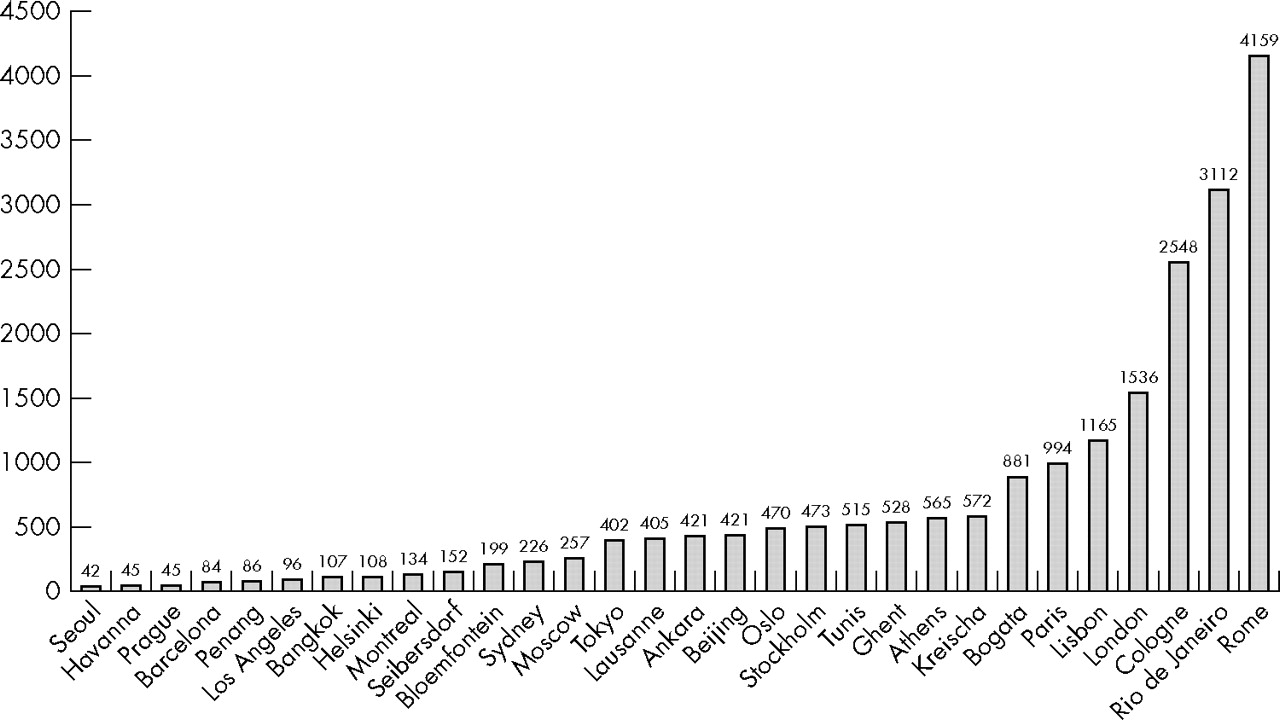
Following FIFA’s 2003 meeting in Zurich with medical representatives of the Olympic Team Sports Federations and representatives from WADA accredited laboratories, it was possible to obtain reliable data on analyses of doping samples performed by the WADA accredited laboratories (fig 4). There was quite a discrepancy in the numbers of samples analysed in the laboratories for football (FIFA) ranging from 42 analyses in Seoul to 4159 in Rome. Analysis of these data might influence the future strategy of the distribution of the samples to the laboratories. Knowledge of the total number of football samples analysed during the year 2004 allows calculation of the incidence of positive samples in total (0.42%), and the distribution and calculation of incidence in the different confederations of FIFA (table 1), and the most commonly found prohibited substances (table 2). The analyses presented do not include the applications for therapeutic use exemption (TUE) or the pending T/E (testosterone/epitestosterone) ratio cases. These cases are extremely difficult to manage and have motivated F-MARC to undertake a new research study in collaboration with the WADA accredited laboratory in Lausanne for direct proof of testosterone in urine. This study is currently underway.
2004 doping statistics (per confederation) from WADA accredited laboratories (excluding T/E)
Substance per positive sample from WADA accredited laboratories (2004)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Numbers of samples analysed in 2004 at WADA accredited laboratories for doping.
The relatively low incidence of positive doping samples, especially for the true performance enhancing drugs such as anabolic steroids and stimulants, support the assumption that there is no evidence of systematic doping. Other important support for the assumption for no evidence of systematic doping has been provided by UEFA (2005/2006 Champions League competition). All 32 participating teams have undergone unannounced doping controls in their training camps. Ten players per team were tested by UEFA medical doctors. All 320 samples were declared negative.
The newly developed FIFA database for management of all samples collected worldwide allows tracking the records of DCOs and has proved to be an extremely useful tool for following up cases, particularly the less experienced FIFA member associations. As of January 2006, this database allows tracking each positive sample with the aim of having the final decision of the member association’s disciplinary committee no later than 90 days after the analysis of the B sample.
The FIFA database will allow a continuous cross-check with the WADA database (ADAMS, Anti-Doping And Management System), once that is operational, not only to control the reporting system of the WADA accredited laboratories, but also to allow prospective studies on sanctions related to the different substances, the severity of the violation, or both.
LIST OF PROHIBITED SUBSTANCES
Like most major governing bodies of sports and the IOC, FIFA has drawn up lists of both prohibited doping substances and methods. The categories of prohibited substances and methods are approved by the FIFA Sports Medical Committee and follow the Prohibited List and International Standards published by the WADA. The most recent FIFA doping control regulations and list of banned substances (January 2006) are divided into three main sections containing different categories of prohibited drugs and methods (box 1). Additional methods and substances such as stimulants, narcotics, cannabinoids, and glucocorticosteroids are included for in-competition testing. The 2006 list includes specified substances that are examined for monitoring purposes and are particularly susceptible to unintentional anti-doping violations because of their general availability in medical products or because they are less likely to be successfully misused as doping agents. A doping violation involving such substances may result in a reduced sanction provided that the (FIFA Doping Control Regulations p. 33):
Box 1 FIFA doping control regulations: categories of banned substances and methods
Prohibited substances
-
Anabolic agents
-
Hormones and related substances
-
β2 agonists
-
Agents with antiestrogenic activity
-
Diuretics and other masking agents
Prohibited methods
-
Enhancement of oxygen transfer
-
Chemical and physical manipulation
-
Gene doping
Substances and methods prohibited in competition
-
Stimulants
-
Narcotics
-
Cannabinoids
-
Glucocorticosteroids
athlete can establish that the use of such specified substances was not intended to enhance sports performance
An extensive list for each category of prohibited substances is provided by FIFA in the annual doping control regulations. These lists are always followed by the words “and related substances” to include all substances that have a similar chemical structure and/or pharmacological effect.
Even though the majority of the drugs described are banned in football, some categories are more capable of enhancing a player’s performance than others and, as such, may well be used in our sport. Two categories not commonly used by players are narcotic analgesics and diuretics. The narcotic analgesics used are mainly from the opioid family—for example, morphine. Diuretics are used as masking agents in certain sports. Both of these categories are contraindicated for the types of exercise that footballers have to perform on the field over 90 minutes. Three categories that could involve footballers are stimulants, anabolic agents, and peptide hormones.
CURRENT DOPING CONTROL REGULATIONS
Cooperation between the confederations and national associations
A comparative study of the existing doping control regulations issued by the FIFA confederations in 1999 showed a high level of agreement as far as the lists of banned substances and methods were concerned. This was because the confederations simply decided to adopt the current FIFA doping control regulations. A detailed survey of the doping control regulations issued by national football associations in 1999, however, revealed some differences in the procedures and inclusion of certain substances in the categories of prohibited substances.
Following this comparative study, the FIFA Sports Medical Committee and F-MARC issued a proposal to the executive committee to harmonise the doping control regulations of all national associations and to adopt the list of prohibited substances and methods. Following FIFA’s executive committee decision, the FIFA congress ratified the decision at its Ordinary Congress in Seoul (May 2002), which paved the way for the decision of the FIFA Extraordinary Congress in Doha/Qatar (December 2003). This follows the method of individual case management and will extend expulsion sanctions by the disciplinary committees of national associations for all international matches, and vice versa.
Stringent rules of procedure
Although the in-competition Doping Control Regulations outline a clear procedure, the out-of-competition controls have not been performed routinely in football mainly because the professional football player is “in competition” almost the entire year except during brief seasonal breaks (two to four weeks) or if in rehabilitation after severe injury.
FIFA and UEFA jointly produced a set of regulations for out-of-competition doping controls for the first time before EURO 2000. About one month before the tournament, all the competing countries were informed that unannounced doping controls might be carried out at training camps and the procedure to be followed. After lots had been drawn to select four national teams, two DCOs (one from UEFA and one from FIFA) visited the training camps in question at around 11 am and immediately reported to the national team’s head of delegation. The head of delegation was requested to find a suitable location for collecting the required samples. The players to be tested—four per team—were then drawn by lots and the doping control procedure was carried out by the UEFA and FIFA doctors immediately afterwards. The experience of these out-of-competition tests showed the need for a much greater level of cooperation between national associations, confederations, and FIFA to ensure that procedures for standard doping controls and unannounced out-of-competition controls were brought more closely into line.
A similar procedure for out-of-competition controls was performed in training camps before the FIFA World Cup 2002 (Korea/Japan) and Euro 2004 (Portugal). The procedure proved to be feasible and the compliance of involved teams and individual players was 100%. Out-of-competition, unannounced controls are planned prior to the FIFA World Cup Germany 2006.
The need to use a medical doctor as a DCO
Although some sporting organisations and anti-doping agencies continue to employ coordinators who are not medical doctors, FIFA and its member confederations insist on physicians for doping controls. This requirement requires closer analysis.
Players from teams selected to undergo a doping test are required to provide details of any treatment with medicines from 7 weeks to 72 hours before the test or the competition in question. All medicines that a player has received must be listed together with details of the method of administration, dosage, and medical indications. The information declared on the forms used for this purpose is covered by patient confidentiality and may not be communicated to non-medical personnel (for example, the general secretary of the football association concerned, the player’s coach or the club’s general manager) unless the A sample tests positive. For confidentiality reasons alone, it is essential that the DCO is a physician with appropriate qualifications for this position.
Clinical studies show that until recently most of the doping substances encountered have been, as a general rule, drugs developed for therapeutic purposes and are primarily used for medical therapy. Today, however, an increasing number of substances are being developed for the sole purpose of doping, and no studies have been conducted into their clinical effectiveness. This is an important reason why specially trained physicians, working in close cooperation with laboratory specialists, should serve as doping control coordinators. The doctor not only has to carry out the control procedure, but also has an educational function before, during, and after the doping control.
PROHIBITED SUBSTANCES PRESCRIBED FOR MEDICAL REASONS (TUE)
If there is any doubt regarding the appropriate therapeutic treatment of a player who has a medically confirmed pathological condition, drugs containing prohibited or partially prohibited substances could be permitted in exceptional cases if:
-
the player’s health would be impaired if the prohibited drug were withheld
-
no performance enhancement could result from the prohibited substance being administered as medically prescribed
-
no permitted or practical alternative drug is available in place of the prohibited substance.
In such a situation, a player or his or her doctor must request for a TUE by submitting a formal application to the FIFA Doping Control Sub-Committee. Strict confidentiality is necessary and guaranteed.
FIFA has become part of an international network in this field, initiated by the Australian Sports Drug Medical Advisory Committee (ASDMAG), and will be able to draw on the accumulated body of knowledge from other team sports, WADA, and individual cases. The TUE applications are managed by the FIFA Doping Control Sub-Committee. A copy of approval or rejection is automatically sent to WADA for information and possible appeal.
LABORATORY ANALYSIS OF SAMPLES
Chain of custody
The laboratories that are in charge of doping analysis throughout the world are all specialised and well equipped institutions, empowered by their national sporting authorities to analyse the urine samples received from sporting authorities. WADA has established an accreditation system for such laboratories. A total of 33 laboratories were fully accredited in 2005 (box 2). This accreditation is based on quality control checks performed annually on each laboratory. The main objective of accreditation is to guarantee uniform quality of analysis at laboratories all over the world.
Box 2 FIFA/WADA accredited laboratories in 2005
Ankara (Turkey)
Athens (Greece)
Bangkok (Thailand)
Barcelona (Spain)
Beijing (China)
Bloemfontein (South Africa)
Bogota (Colombia)
Cambridge (England)
Cologne (Germany)
Gent (Belgium)
Havana (Cuba)
Helsinki (Finland)
Kreischa (Germany)
Lausanne (Switzerland)
Lisbon (Portugal)
London (England)
Los Angeles (USA)
Madrid (Spain)
Montreal (Canada)
Moscow (Russia)
Oslo (Norway)
Paris (France)
Penang (Malaysia)
Prague (Czech Republic)
Rio de Janeiro (Brazil)
Rome (Italy)
Seibersdorf (Austria)
Seoul (Korea)
Stockholm (Sweden)
Sydney (Australia)
Tokyo (Japan)
Tunis (Tunisia)
Warsaw (Poland)
International federations, including FIFA, use these official laboratories for their major events and competitions. The laboratory is requested by the governing body concerned to analyse samples and is obliged to comply strictly with the rules laid down in their medical codes. The laboratories treat all samples anonymously with each sample being labelled with a code number known only to the player and the committee in charge of the controls. This is essential to assure the player that the analysis is completely objective and to avoid any undue pressure on the laboratory which analyses the samples.
The results (negative or positive) are communicated to the committee in charge of the controls. If the A sample is positive, the test is performed a second time before the result is sent to the relevant committee. A copy from the report of any positive case is simultaneously sent to the international federation (if the committee in charge is not in charge of the controls) and to FIFA and WADA. The committee in charge then informs the player who then has a limited time to request analysis of the B sample.
The sample analysis
Samples are analysed with the aim of identifying all detectable banned substances. The equipment used is state of the art technology designed to generate a “molecular fingerprint”. The technique of choice is gas (or liquid) chromatography controlled with detectors based on mass spectrometry. Chromatography is the first step in the analysis, consisting of a preliminary separation in the mixture of several natural or non-natural substances contained in each urine extract. After the substances have been sorted, a mass spectrometer provides a picture of the molecular structure that can be compared with others stored in the chemical databases of the computer that controls the entire system.
The aim of these analyses is to prove that no banned substances are present in the urine samples provided by “clean” players (the vast majority: a true negative), so that a player can then be declared negative. In positive cases, the same technology must also deliver absolute chemical proof that a banned substance or its degradation products (called metabolites) are present in the urine (a true positive). Every possible step is taken to prevent samples from erroneously being declared positive (a false positive); in general, the purpose of B sample analysis is to provide confirmation of the result obtained during the first test in the presence of the player or one the player’s representatives.
Unfortunately, not all banned substances used in sport can be detected using this technology (a false negative). In addition, some of them have exactly the same structure as their natural endogenous forms and are quite difficult to tell apart.
The T/E ratio
Widespread use of anabolic steroids in doping began in the 1980s and testosterone was one of the preferred androgenic-anabolic agents. Until recently, it was difficult to differentiate between synthetic and natural testosterone in the body. The only method available was a quantitative one involving the establishment of a ratio with another steroid called epitestosterone, which is similar to testosterone and is very stable in its concentration. The normal Caucasian and African populations have a mean ratio (testosterone to epitestosterone, T/E) of 1.5:1 (for males) with some variability, rising to 4:1 in rare cases. The mean ratio for Asian people is generally lower than 1:1. A player with excessive levels of testosterone will have a much higher ratio, resulting from an increase in testosterone concentration. It was later decided that the maximum permissible T/E ratio would be 6:1, and that any ratio over this limit would be declared positive. Currently, the limit for an adverse finding is fixed at 4:1.
In addition to the T/E ratio, monitoring of the complete steroid profile of the player over time can also demonstrate manipulation. This can be due to the consumption of other steroids such as testosterone precursors which can be easily purchased over the internet. Moreover, new laboratory instrumentation, the isotope ratio mass spectrometer (IRMS), allows differentiating between steroids of endogenous and exogenous origin in urine. This tool, together with retrospective data on the player, if they exist, and in some cases, additional endocrinological investigations, will provide the disciplinary commissions with the opportunity to make the most accurate decision in a timely manner.
A validation study initiated in 2004 by FIFA jointly with Swiss Anti-Doping Laboratory (LAD, the WADA accredited laboratory in Lausanne) is in progress.
The case of nandrolone
Just before the FIFA World Cup in France in 1998, a number of well known players tested positive for small amounts of nandrolone metabolites in their urine. Nandrolone (chemical name nortestosterone) is an anabolic steroid often encountered in bodybuilding doping cases. In general, this compound is taken in high doses and its degradation products (metabolites) remain detectable in urine for up to several months. Before the 1998 World Cup, FIFA commissioned an independent anti-doping laboratory (LAD) to carry out a collaborative study to obtain a true picture of the situation in football. With the agreement of national and international bodies, every player from every team in the top national leagues in Switzerland (A and B leagues) was tested after a game (356 players in total over two weekends) in collaboration with the Swiss anti-doping committee. The results were compared with those obtained by testing amateur footballers and students. Without revealing anything about the origin of these products, the study showed some players had nandrolone metabolites in their urine after the game. The traces of metabolites in the urine of those players were very small, and all were below the limits of a positive reading.
On the basis of this study, FIFA was able to organise the anti-doping programme for the 1998 World Cup with a degree of assurance to provide reliable information to the competing teams to rule out any occurrence of false positive tests. With FIFA’s support, this study into nandrolone and its derivate substances continued. Extraordinary variability in excretion was shown, making the relation between dosage, time delay, and urine concentration critical. Involvement of a world governing body in such a research programme is essential if any worthwhile progress is to be made in this area. The players can also be given the assurance that, scientifically and ethically, they start a match on an equal “playing field” with their opponents as far as doping is concerned.
THE PEPTIDE HORMONES
There are several peptide hormones in the list of prohibited substances, of which the two most important are EPO and the human growth hormone (hGH).
EPO
The use of EPO in sport can be established by analysing urine by a novel method based on the biochemical properties of EPO. EPO and its analogues are too large to be filtered by the kidney and are easily eliminated in urine. As their concentrations in urine are so low there was a need for improvement in biochemical technology to allow the detection of this product in urine. Thus, in 2000, the WADA accredited laboratory in Paris implemented a method based on a small structural difference between recombinant and natural EPO to determine whether doping had taken place. This method is now applied in several accredited laboratories in the world.
hGH
The chemical structure of bioengineered hGH is almost identical to the natural hormone produced by the body. Consequently, it is particularly difficult to differentiate between the injected and the natural hormone. Recently developed methods use blood as a biological sample for the determination of a specific ratio diagnostic for the use of recombinant hGH. This new approach clearly demonstrates the necessity to implement blood sampling for anti-doping purposes.
Blood sampling
Recently, blood has been introduced as an alternative biological matrix to urine for anti-doping sampling purposes. Since 2004, blood has been recognised as absolutely necessary for reliable results for some forbidden substances and methods. The list of these substances and methods is not definitive, but currently, hGH, synthetic haemoglobins, and homologous blood transfusions can be reliably detected with several blood matrices.
Some other blood tests are also carried out in certain sports, not for the purpose of determining the presence of doping, but rather as general health checks conducted in the context of medical screening of the competitors. This has potential for the future and could easily be introduced by some national or international federations depending on their structural organisation. However, this concept is more difficult to implement in larger federations which have players on every continent.
FIFA NETWORK OF DCOs
In cooperation with the football confederations and national associations, FIFA has established a worldwide network of more than 250 specially trained physicians who act as FIFA’s DCOs. With regard to medical confidentiality and the necessity for specific knowledge in the field, FIFA only accepts physicians as DCOs.
To ensure “unity of doctrine” all DCOs attend instructional seminars conducted by F-MARC (Professor Jiri Dvorak, Chairman) and FIFA Doping Control Subcommittee (Professor Toni Graf-Baumann, Chairman). Such seminars have been held for CAF (Tunis, November 2000), AFC (Penang, January 2001), UEFA (Zurich, January 2001), CONCACAF (Miami, February 2001), and OFC (Auckland, New Zealand, March 2001), and also in Tunis in January 2004, Marrakesh in November 2004, Buenos Aires in March 2005, Oman in May 2005, Port of Spain in December 2005, Auckland in February 2006, and Buenos Aires in April 2006.
The DCOs, as members of the FIFA network, are currently spread around the world. To make doping control cost effective, the FIFA Congress followed the recommendation of the Sports Medical Committee that DCOs are, by profession, physicians who follow the Hippocratic Oath and their professional laws. DCOs perform doping controls on their national team in their country when playing against a team from another country. The FIFA doping control procedure is straightforward and transparent, leaving no room for cheating or wrongdoing when all steps are performed in the presence of representatives from both teams. This makes the logistics easier and significantly reduces the costs involved, particularly for qualifying matches for major competitions.
RESEARCH
The current list of banned substances contains a number of drugs for which there is no conclusive scientific evidence to justify inclusion on the list. Research on selected substances has highlighted some performance enhancing effect whereas other references are doubtful. In view of the potentially enormous repercussions (as demonstrated at the Sydney Olympic Games) there are several ways of improving the current situation.
-
A database containing all currently listed substances should be set up. This should give details on the pharmacological background, research findings, and clinical papers documenting the effects of the particular substance.
-
Borderline substances should be reconsidered on the basis of research studies providing scientific analysis of their effect on physical and psychological performance as well as effect on the metabolism.
-
A standard study design (double blind, randomised trials) should be set up for substances under scrutiny, proved in pilot projects and implemented multicentrically. The results of such studies should form the basis for future inclusion on the list of prohibited substances.
-
Tracing and identification of masking agents.
Such initial research work might help to reduce the list of banned substances so that the focus can be on the major problem areas such as anabolic steroids, and peptide hormones and related substances, such as human chorionic gonadotrophin, hGH, and EPO. Research into nandrolone metabolism in footballers, conducted with FIFA’s support, eloquently documents the complexity of the problem. The study showed that current laboratory methods cannot distinguish between endogenous metabolism and exogenous intake of nandrolone. Although the cut-off level of 2 ng/ml would appear rational, it is not scientifically proved, leaving the door wide open for discussion. Further double blind studies are in progress in an attempt to obtain the scientific evidence needed to end the ongoing speculation. Until then, this cut-off level is valid and will remain in effect.
FIFA has realised and documented its responsibility by supporting research studies that promise to enhance current medical knowledge. A combined effort with other international sports federations, the IOC, and anti-doping agencies might, however, accelerate the process.
EDUCATING THE FOOTBALL COMMUNITY ABOUT DOPING AND PERFORMANCE
Two issues of importance with regard to education of the football community are:
-
Collaborating with team doctors
-
Supplements and special nutrition
Continuous and close contact with team doctors is necessary in countries where sports medicine is still developing and where the team doctors may not have special training on doping issues. In view of the rapid changes in doping with regard to both substances and methods of administration, a constant exchange of information with all team doctors is essential. Besides the fact of the problem, effective procedures against doping cannot be put into practice unless a close, trusting relationship has been established between the team doctors and the DCOs.
With regard to above, particular attention must be paid to food supplements and special diets that might be prescribed for an player. Supplements or diets may contain banned substances, which means that the player may be taking substances (or using food supplements) without realising that it may contain a banned substance. If the player tests positive, it is difficult to prove that the substance(s) in question originated in the player’s food or food supplements. From the legal point of view, players testing positive in such situations must bear the responsibility themselves. Here, too, a constant flow of information between DCOs and team doctors helps everyone keep abreast of developments in the “market” and prevent problems arising for players.
The recently published summary of the “Nutrition for Football: the FIFA/F-MARC Consensus Conference”4 clearly states that there is no evidence to support the current widespread use of dietary supplements in football. Supplements should be used only on the advice of qualified sports nutrition professionals. Football players can stay healthy, avoid injury, and achieve their performance goals with good dietary habits. Players should choose foods that support and optimise both training and match performance. What a player eats and drinks in the days and hours before a game, as well as during the game, can influence the result by reducing the effects of fatigue and optimising performance. Food and fluid ingested soon after a game and training can accelerate recovery. All players should have a nutrition plan that takes individual needs into account.
FIFA’S COOPERATION WITH wada
On 4 February 1999, a Lausanne declaration on doping in sport was presented to the IOC and international sport federations that an independent international anti-doping agency should be established and fully operational by the 2000 Olympic Games in Sydney to coordinate the various programmes necessary to realise the objectives. FIFA’s medical and legal representatives have developed a close collaboration since 1999 based on numerous meetings with the representatives of the WADA, particularly following the meeting of FIFA President Mr Joseph Blatter and the Chairman of WADA, Mr Richard Pound, in Montreal in December 2001.
FIFA’s medical and legal experts contributed significantly to the improvement of the World Anti-Doping Code particularly in versions 1 and 2. They insisted on having independent expert opinion by prominent European judges and lawyers, including the International Sports Lawyers Association, on individual case management regarding positive cases. This individual case management has been confirmed as a strategy by internal studies of the medicolegal aspects of the team sports federations based upon 184 positive samples between 1998 and 2003 in different sports.
After intensive discussions with Mr Pound, the management of WADA, and a historic speech delivered by Mr Pound (54th Ordinary FIFA Congress in Paris on 19 May 2004), an informal agreement on collaboration between FIFA and WADA was signed by the respective presidents and confirmed by the IOC President, Dr Jacques Rooge. Based upon this agreement and adaptation of the FIFA Doping Control Regulations, changes have been incorporated in the FIFA Disciplinary Code.
LEGAL BACKGROUND
In this regard, the legal background will be briefly described. FIFA is a private association in accordance with Article 60 ff. Swiss Civil Code with headquarters in Zurich, Switzerland. Consequently, FIFA is a legal person in accordance with Swiss private law and has to comply with it when setting up its statutes and regulations.
The principles of fault and individual case management are essentials of Swiss sanction law and therefore have to be considered when imposing private sanctions. Every sanction contains a distinctive individual component, because every sentence has to take into account the fault of the delinquent. FIFA has been following these principles in its Doping Control Regulations from the beginning.
To base its decisions on expertise, FIFA itself sought a legal opinion from the Court of Arbitration for Sport (CAS) about the extent to which WADA’s code complied with Swiss law in September 2005.
In its legal opinion published in April 2006, CAS explicitly confirmed FIFA’s practice of individual case management when sanctioning doping offences. In addition, CAS noted that FIFA’s principle of individual case management complies with the World Anti-Doping Code. At the same time, the independent sports arbitration body, with headquarters in Lausanne (Switzerland), has also ruled that FIFA’s provisions with regard to the fight against doping and the sanctioning of doping offences are, to the greatest possible extent, in line with the World Anti-Doping Code, and that they are also fully in line with Swiss law. CAS also compared FIFA’s provisions with those of the World Anti-Doping Code in 22 main areas. In 16 points, including the definition of doping, the strict liability principle, the list of prohibited substances, therapeutic use exemptions, testing and analysis, hearings, commencement of the ineligibility period, and disqualification provisions regarding teams, CAS stated that there were no material differences between the two sets of regulations.
Furthermore, CAS confirmed FIFA’s attitude by stating that neither the IOC nor WADA has the right to dictate to FIFA as regards the latter’s disciplinary regulations for the fight against doping and the sanctioning of doping offences. According to CAS, international sports federations are free to establish such provisions as they deem appropriate, especially as CAS also noted that the World Anti-Doping Code is not legally binding per se. CAS reported differences in six areas between FIFA’s provisions and the World Anti-Doping Code, although it only highlighted significant deviations in three of these points. CAS came to the general conclusion that with regard to the approach used to determine the level of punishment to be imposed, there are no considerable differences between the two sets of regulations. FIFA, as well as WADA, are in the process of finding a consensus to maximum and minimum of sanctions.
With regard to possibly eliminating a sanction in cases in which athletes prove that they did not act with fault or negligence, CAS recommended that FIFA incorporate an appropriate provision in its regulations and not impose sanctions on athletes who prove that a prohibited substance entered their body through no fault or negligence of their own. FIFA, however, already follows such a practice by applying the principle of guilt when sanctioning doping offences. In addition, FIFA was advised by CAS to adapt its regulations to clarify WADA’s right of appeal against procedures followed in final-instance decisions. Conversely, it was noted that with its provision regarding the statute of limitations, the World Anti-Doping Agency’s code is not in line with Swiss law.
This legal opinion from CAS has laid the foundations for FIFA to make the necessary adjustments to the relevant provisions independently. FIFA, together with WADA, under the moderation of the Sports Minister of England, Mr R Caborn, have discussed the points of differences in a constructive way to reach a FIFA’s complete compliance with WADA code. Beyond that, after being operational for two years, it seems reasonable to reflect on the feasibility and applicability of the World Anti-Doping Code based upon the analysis of positive doping cases as related to the incidence and management among the different member associations. Such analysis is foreseen within the revision of the World Anti-Doping Code, which was initiated by WADA in April 2006.
OCCUPATIONAL MEDICINE IN FOOTBALL: A VISION
Occupational medicine deals with all work related aspects of health that affect the employee’s ability to function effectively: the workplace itself, the type of work, the state of health of the employee. In addition to purely physical aspects, social and psychological influences must also be considered. It is easy to see that construction workers who are paid according to how much work they complete will be subject to greater stress than, say, a gardener or office worker employed on standard terms. Moreover, within any occupation there are those—often a considerable percentage—who will regularly need medicines to function properly—for example, those with diabetes, high blood pressure, allergies, rheumatic disorders. In such cases, any extra stress in the work environment can easily lead to a situation where the ability of the person to function is close to the borderline of what can be physically expected. These people can often become incapable of continuing in the job or of only doing so under medical supervision and with the prescription of suitable medicines.
There are definite limits to the level of stress under which such people can function and it is the concern of occupational medicine to recognise and deal with these limits. Occupational medicine aims to point out to both employer and employee that only under certain specified conditions will optimum performance be possible. The conditions that could be recommended in such cases might include changes in the workplace, in working hours, in the pressures of the job, or might specify regular medical treatment for the employee—for example, prescription medicines to protect the employee from the effects of workday stress, such as β blockers.
What is already known about this topic
Doping control in sports was introduced in 1968, with the aim of upholding and preserving the ethics of sport, safeguarding the physical and mental integrity of players, and ensuring equal chances for all competitors. Different approaches have been used in the fight against doping. These approaches should ideally be based on valid data of the true extent of doping and sound scientific knowledge of substances, their pharmacokinetics, pharmacodynamics, and effects, and the detection methods.
If we now consider a sport such as football, a number of examples can be identified. The proportion of players who have allergies is similar to that in the general population, and the treatment will be the same—that is, appropriate therapy often involving the taking of medicines, especially during those times of the year when the allergen count is high. But when we are dealing with open air sports, the treatment prescribed could lead to problems since many of the drugs usually prescribed are on the list of banned substances (such as corticosteroids) even though their prescription is medically justified.
An example of an American professional international woman player makes the situation clear. She has a relatively rare disease that makes her blood pressure and fluid balance subject to extreme variations; this in turn makes it impossible for her, without medical help, to pursue her profession at the required level. She needs ongoing treatment with a mineralocorticoid (fludrocortisone). However, in contrast with those mentioned above, this medicine has neither an anabolic nor an anti-phlogistic effect and is thus not technically a doping substance in the true sense of the term. This raises the question whether it really constitutes doping if a player can perform at the expected level only after taking such a medicine. We suggest that this is a problem that falls within the scope of occupational medicine. If such treatment is prescribed for genuine medical reasons and involves taking a drug that in itself has no doping effect, then we cannot be talking about a case of doping, rather merely of enabling a professional player to exercise his or her normal profession. Occasional treatment with banned substances for “bona fide” medical reasons should be permitted if the facts of the case are presented openly to the doctors in charge of the doping control.
A quite different question is whether the ever increasing demands faced by professional footballers, in terms of the number of matches and tournaments in which they are expected to play, can be compensated for by taking medicines so that the required level of performance can be achieved over and over again. Playing so frequently, in football as in other sports, under circumstances necessitating more or less continual treatment with painkillers and anti-inflammatory agents, can have serious long-term consequences that really cannot be justified on the basis of occupational medicine or medical ethics. In this case, the limits of doping are recognisable.
Admittedly there is no doping in the first two examples in terms of performance enhancing drugs being taken. However, in the sense of medical treatment being used to suppress the symptoms of injuries and overexertion, clearly there is an aspect of doping involved. The workplace pressures on players in the short term lead to long term effects being ignored. As long as the players in question and their associations all have the same approach, only a firm stand by sports and occupational medicine will have the effect of providing the players with at least partial protection from such long term damage. This is further reason why the campaign against real doping must be actively pursued.
What this article adds
According to the data presented, the incidence of doping in football seems to be quite low (0.4%). The vast majority of positive samples are due to recreational drugs. These findings support FIFA’s strategy of education and prevention. On the basis of principles of occupational medicine treatment banned substances for medical reasons should be allowed to enable players to carry out their professional obligations.
Footnotes
-
Competing interests: None declared