Article Text

Abstract
Objective: To evaluate a sports safety-focused risk-management training programme.
Design: Controlled before and after test.
Setting: Four community soccer associations in Sydney, Australia.
Participants: 76 clubs (32 intervention, 44 control) at baseline, and 67 clubs (27 intervention, 40 control) at post-season and 12-month follow-ups.
Intervention: SafeClub, a sports safety-focused risk-management training programme (3×2 hour sessions) based on adult-learning principles and injury-prevention concepts and models.
Main outcome measures: Changes in mean policy, infrastructure and overall safety scores as measured using a modified version of the Sports Safety Audit Tool.
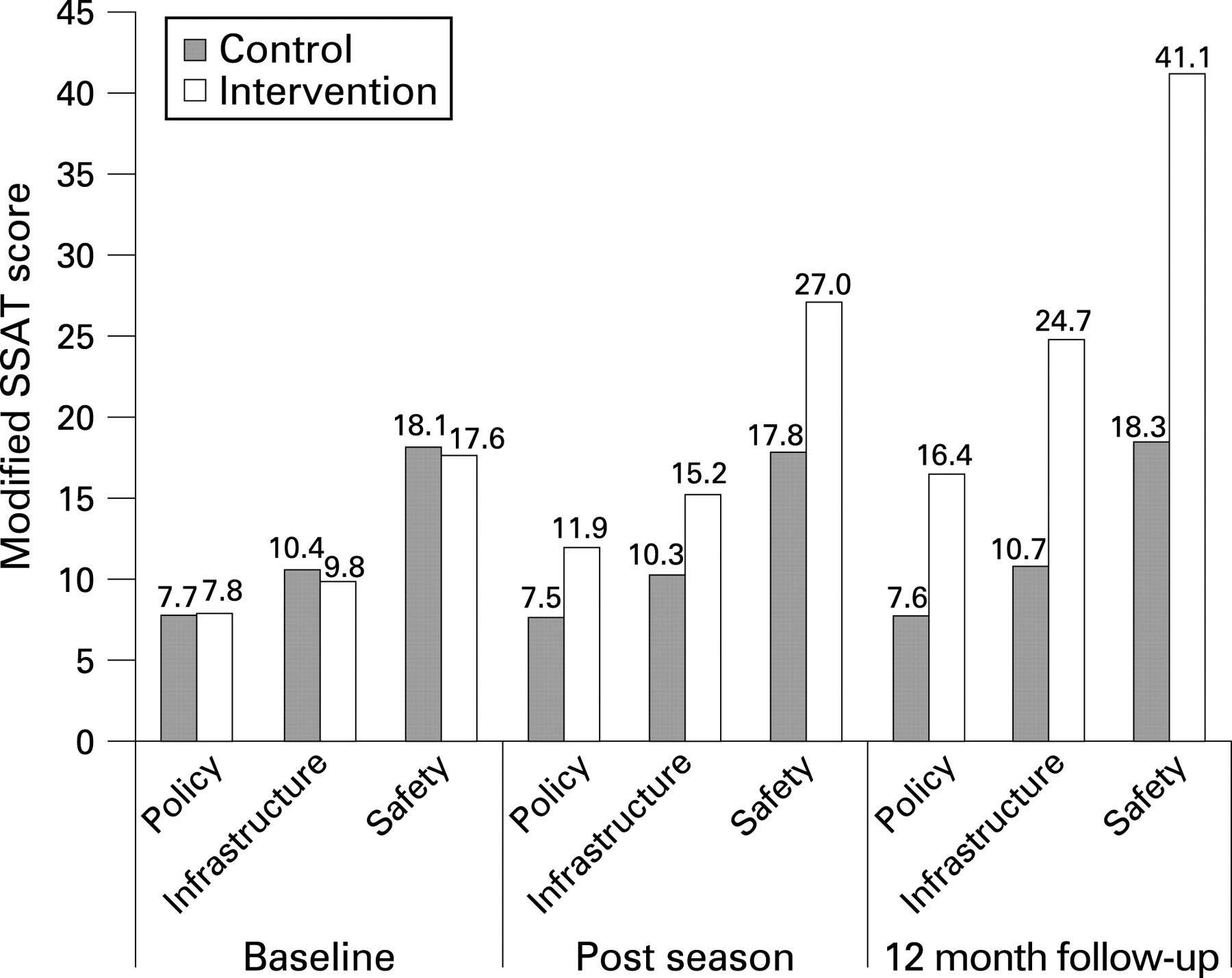
Results: There was no significant difference in the mean policy, infrastructure and overall safety scores of intervention and control clubs at baseline. Intervention clubs achieved higher post-season mean policy (11.9 intervention vs 7.5 controls), infrastructure (15.2 vs 10.3) and overall safety (27.0 vs 17.8) scores than did controls. These differences were greater at the 12-month follow-up: policy (16.4 vs 7.6); infrastructure (24.7 vs 10.7); and overall safety (41.1 vs 18.3). General linear modelling indicated that intervention clubs achieved statistically significantly higher policy (p<0.001), infrastructure (p<0.001) and overall safety (p<0.001) scores compared with control clubs at the post-season and 12-month follow-ups. There was also a significant linear interaction of time and group for all three scores: policy (p<0.001), infrastructure (p<0.001) and overall safety (p<0.001).
Conclusions: SafeClub effectively assisted community soccer clubs to improve their sports safety activities, particularly the foundations and processes for good risk-management practice, in a sustainable way.
Statistics from Altmetric.com
Sports injuries are a public health issue that incur a high personal, social and economic cost.1–3 Injury and the fear of injury are barriers to participation in physical activity,4 5 and addressing sports injuries is a public-health priority.6 7 Most sports injuries are preventable,8 9 and sports governing bodies have a legal and ethical responsibility to endeavour to prevent injuries by identifying, assessing and controlling the risks associated with their sport.10 The application of risk-management principles to sports safety has been advocated internationally10–13 and in Australia.9 14 15 Risk management has been described as “the culture, processes and structures that are directed towards realising potential opportunities whilst managing adverse effects”.16 Risk management underpins occupational health and safety practices in most sectors.17
The sport/leisure sector has not recognised the importance of risk assessment10 nor the support needs of community sports clubs to conduct safety-related risk management.18 An Australian standard is available for managing risk in sport and recreation,16 and resources and training are available to support sporting organisations with risk management.11 19 20 However, sports-related risk management has tended to come from a legal/insurance viewpoint rather than a public-health/injury-prevention perspective.21 In the peer-reviewed literature, there is no information about the development, adoption, evaluation or dissemination of currently available sports safety-related risk-management resources or training.
The aim of this study was to evaluate SafeClub, a sports safety and injury prevention-focused risk-management training programme for community sports clubs. The evaluation measured the impact of SafeClub on the sports safety activities (ie sports safety-related risk management policies and infrastructure) of participating community soccer (football) clubs in Sydney, Australia. Although SafeClub has been designed for use with all community sports, soccer was considered the most suitable sport in which to conduct the evaluation. Soccer is popular,22 has a relatively well-understood injury profile,23 24 has poor safety policies and practices compared with other Australian community sports,18 25 and is a priority for injury-prevention action in Australia.26
METHODS
A controlled pre–post test study design was used. The Northern Sydney Area Health Service Human Research Ethics Committee approved the study.
Sample
Soccer New South Wales (NSW) identified four affiliated community soccer associations in the Greater Sydney region for participation in the study, based on their knowledge of each association’s capacity, infrastructure and interest. Two pairs of similar associations were recruited. The associations similar in size (number of affiliated clubs), budget, size of committee, paid administration hours, association policies, and support for affiliated clubs. One association from each similar pair was randomly allocated to each arm of the study: intervention (SafeClub) or control (usual sports safety activities).
Clubs affiliated with the participating associations were invited to join the study via presentations at association annual general meetings in 2004. Following the presentations, each club was contacted by telephone to arrange a suitable baseline data collection time. Clubs in the same association were allocated to the same arm of the study.
Intervention
SafeClub is a training programme based on a five-stage model of risk management: risk identification, risk assessment, risk management, implementation and evaluation.9 21 SafeClub was developed in response to a survey that found that few community soccer clubs adopted a strategic approach to safety or had the infrastructure to implement sustainable injury prevention initiatives.27 Additional informal consultations with regional sports associations and community clubs also suggested that the safety issues of concern varied significantly from club to club depending on the club’s size, facilities, human resources, location, and player and spectator characteristics. SafeClub was developed to assist clubs to identify and manage their specific safety issues, rather than adhere to a prescribed set of safety activities that may not be relevant to their needs.
SafeClub delivery consists of three 2-hour training sessions based on adult-learning principles including using practical, problem-centred learning strategies that capitalise on participants’ knowledge and experience. Between sessions, participants are asked to try out ideas discussed during the training and report on progress at their club. The process for identifying and selecting risk-management strategies is based on injury-prevention concepts and models.28 Participating clubs are encouraged to develop a sustainable, club-specific sports safety manual by the end of the training. SafeClub was piloted and presented, in modified form, as a workshop at a national scientific conference29 before being evaluated in this study. SafeClub was delivered in mid-2005, in the middle of the community soccer season.
Data collection
Demographic and sports safety activity information were gathered from participating clubs using a modified version of the Sports Safety Audit Tool (SSAT).30 The SSAT modifications were based on a review of sports injury-prevention best practice, which advocated the development and implementation of sports safety plans using risk-management processes, including delegating responsibility for safety, prioritising key issues, considering first aid and protective equipment, hazard inspections, and a review component.9 15 The modified SSAT used in this study is available upon request.
Each participating club completed the 72-item modified SSAT three times: at the start of the 2005 season (baseline), at the end of 2005 season (post-season) and midway through the 2006 season (12-month follow-up). Clubs that could not be contacted after four telephone attempts were considered non-respondents at each data-collection stage. Most interviews were conducted using a standard interview protocol during a face-to-face meeting with a club representative. However, nine of the 12-month follow-up interviews were conducted over the telephone. Presidents and secretaries were the preferred representatives, and interviews were conducted at times and locations convenient to participants, usually after hours at their club, home or workplace.30
Characteristics of the clubs
In total, 32 of a possible 50 intervention clubs (64% response rate) and 44 of a possible 51 (86% response rate) control clubs were enrolled in the study at baseline. Of these, 27 intervention clubs and 40 control clubs were still enrolled at the post-season and 12-month follow-ups. There was no significant difference between the retention rates for intervention (84%) and control clubs (91%) (χ2(1, n = 76) = 0.758, p = 0.384).
Of the 76 clubs enrolled at baseline, 49% were represented by the club secretary, 38% by the president, 4% by the treasurer and 9% by others (eg coaches, sports trainers). Most (86%) clubs were incorporated and 3% employed a paid administrator. The mean length of existence of clubs was 31.9 (SD 17.9) years. Three-quarters (75%) of the clubs had been in existence for >20 years and 9% for <5 (range 1 to 86) years.
At baseline, the participating clubs varied in size from 7 to 113 registered teams (mean 39.2, SD 26.5) with 70 to 1369 registered players and 4 to 28 committee members. Approximate annual budgets ranged from $A1000 to $A325 000 (mean $95 396 (SD 73 760)). There were no significant differences between intervention and control clubs on the demographic items measured except that intervention clubs were bigger (mean 47.7 vs 32.9 teams, 95% CI 2.9 to 26.8) and had more registered players aged ⩾12 years (mean 324.3 vs 202.8, 95% CI 35.4 to 207.7). Table 1 shows the demographics of intervention and control clubs at baseline.
Not all clubs provided information for each item so the number for each item varies and the mean was calculated based on the number for each item (range intervention clubs 28 to32, control clubs 35 to 44).
Statistical analysis
A scoring system was developed for the SSAT before the start of the study. Items that the researchers considered reflected fundamental and wide-reaching risk-management practices identified in the literature9 15 18 were scored more highly than specific, individual items considered to be less important to sports safety. For example, a documented sports-safety/risk-management plan scored 5 points, whereas having safety as a regular item on committee meeting agendas scored 2 points and having a sun-protection policy scored 0.5 points. The maximum possible overall safety score of 65 was made up of a maximum policy score of 24 (from 30 policy items) and a maximum infrastructure score of 41 (from 26 infrastructure items).
The required sample size was estimated to be 33 clubs in each arm of the study. This assumed 80% power to detect a post-intervention difference of 15% in infrastructure score and 20% in policy score with a statistical significance level of 0.05 and a drop-out rate of 40%.
The independent samples t test was used to compare the demographic data of control and intervention clubs, and of clubs that were retained in the study and those that dropped out. The χ2 test was used to compare the proportion of intervention and control clubs responding positively to individual items at baselinebaseline, post-season follow-up and 12-month follow-up. A mean score was calculated for two items (“safety activities undertaken in past 12 months” and “other documented safety policy”) and this was compared at baseline, post-season follow-up and 12-month follow-up for intervention and control clubs using the independent samples t test. Policy, infrastructure and overall safety scores were compared at baseline, post-season follow-up and 12-month follow-up using a general linear model for repeat measures with time (baseline, post-season follow-up and 12-month follow-up) as the within-subject factor and group (intervention or control) as the between-subject factor. Statistical significance was set at p<0.05 with 95% CI. All data were analysed using SPSS V.10.0* (SPSS, Chicago, Illinois, USA).
RESULTS
Tables 2 and 3 show the proportions of intervention and control clubs that responded positively on each modified SSAT policy and infrastructure item respectively. The mean modified SSAT scores are provided for the items where respondents could report more than one activity (eg “safety activities undertaken in the past 12 months” and “other documented safety policy”) at baseline, post-season follow-up and 12-month follow-up.
At baseline, there were two items to which a significantly higher proportion of control than intervention clubs responded positively. Control clubs were more likely to report keeping a record of injuries that required attending hospital (64% vs 34%, χ2(1, n = 76) = 6.359, p = 0.012) and injuries that required attending a general practitioner/health professional (48% vs 16%, χ2(1, n = 76) = 8.483, p = 0.004).
At the post-season follow-up, a significantly higher proportion of intervention clubs than control clubs responded positively to 13 items. A significantly higher proportion of control clubs responded positively (92% vs 70%, χ2(1, n = 67) = 5.753, p = 0.016) to one item, “Collects injury risk information from Soccer NSW /Football Federation Australia” at this follow-up.
The post-season trend of intervention clubs responding more positively continued at the 12-month follow-up, with a significantly higher proportion of intervention clubs responding positively to 30 of the 56 items. There were no items to which a significantly higher proportion of control clubs responded positively at the 12-month follow-up.
Figure 1 shows the mean policy, infrastructure and overall safety scores for control and intervention clubs at baseline, post-season follow-up and 12-month follow-up.
{kind=link}
The general linear modelling indicated that the effect of time was significant for the policy (F(2,130) = 31.32, p<0.001), infrastructure (F(2,130) = 30.29, p<0.001) and overall safety (F(2,130) = 45.38, p<0.001) scores. Importantly, there was a significant linear interaction of time and group for all three scores: policy (F(2,130) = 31.16, p<0.001), infrastructure (F(2,130) = 28.20, p<0.001) and overall safety (F(2,130) = 43.45, p<0.001).
There was no significant difference in the baseline demographic characteristics or in the policy, infrastructure and overall safety scores of clubs that were retained in the study (n = 67) compared with those that dropped out (n = 9). The only item at baseline to which a significantly different proportion of retained than dropped-out clubs responded positively was for a “documented sports safety/risk-management policy” (22% vs 56% retained versus dropped out; χ2(1, n = 76) = 4.501, p = 0.034).
DISCUSSION
To our knowledge, this is the first evaluation of a risk management-focused sports-safety training programme for community sports clubs published in the reviewed literature. Most previous sports-safety and injury-prevention research has focused on the first two stages of van Mechelen’s four-stage model of sports injury prevention, establishing the extent of the problem, and the aetiology and mechanisms of injury.31 The current study evaluates an intervention to assist in the implementation of best practice. In terms of the Translating Research into Injury Prevention Practice (TRIPP) framework for sports injury prevention research proposed by Finch,33 this study fits into stage 5: understanding how evidence-based practice can be translated into actions that can be implemented in real-world circumstances.
The results of this study strongly suggest that SafeClub achieved its aim of assisting community soccer clubs to improve their sports-safety activities. There is also evidence that improvements reported by participating clubs were sustained, if not increased, over time. Interestingly, at the 12-month follow-up, a significantly higher proportion of the clubs that participated in the SafeClub training responded positively to 9 of the 10 items that were given a weighting of ⩾2 points (ie were considered fundamental and wide-reaching risk-management practices). This suggests that SafeClub was particularly effective at enabling clubs to lay the foundations for good risk-management practices through establishing core infrastructure (eg appointing a safety committee/coordinator); putting key processes in place (eg regularly reviewing injury records/risk information to inform plans, having safety as a committee meeting agenda item, acting upon and reviewing safety plans in a timely manner); and writing and regularly reviewing comprehensive safety policies and plans. A higher proportion of SafeClub-trained clubs also reported having a specific safety budget at the 12-month follow-up, but the difference did not reach statistical significance.
The application of risk-management principles to the development of sports-safety plans has been widely called for,9–16 19 20despite there being little evidence directly linking risk management to a reduction in sports injuries. Given the difficulty and cost of obtaining reliable community sports injury data34 35 and the limited resources available for this study, the outcome measure of interest in this study was indicators of good sports safety practice rather than injury rates. Whether the sports safety activities adopted by participating clubs were effective in reducing injuries is a separate question more aligned to stage 4 of the TRIPP framework (ideal conditions/scientific evaluation of preventive measures33) or stages 3 and 4 of van Mechelen’s model (introducing preventive measures and assessing their effectiveness31). The critical factor for SafeClub in this context was that it encouraged, supported and resourced evidence-based planning36 that enabled participants to develop sustainable safety activities tailored to meet the unique circumstances of their club.
There were several safety activities that >80% of participating clubs reported at baseline that they had already implemented. For example, nearly all clubs reported having documented policies on wearing/using protective equipment at competition and training, conduct of players and others attending competitions, modified rules for juniors, and child protection. In addition, >80% of participating clubs reported that they collected injury risk information from the state governing body for the sport (Soccer NSW), and >60% had a written “blood rule”, kept records of injuries that generated insurance claims, and regularly informed and consulted with coaches and committee members about safety. These findings suggest that safety was already on the agenda in some way at many participating clubs, perhaps as a result of Soccer NSW having previously introduced specific organisation-wide policies.
The limitations of this study need to be acknowledged. The community soccer associations that participated in this study were not randomly selected. They, and their affiliated clubs, may have been significantly different from other associations and clubs. However, any selection bias was minimised by the random assignment of similar pairs of associations to intervention or control arms of the study. Self-reporting by participants and the non-blinding of participants and researchers introduced the potential for interviewer bias and social desirability biases among participating clubs. This bias was minimised with the use of a validated modified SSAT,30 a standardised interview protocol and interviewer training. The potential for contamination between intervention and control clubs was limited because selected associations were geographically distant from each other, and clubs from the same association were assigned to the same arm of the study. Although there was no significant difference in demographics or SSAT scores between clubs that dropped out of the study and those that were retained, it is possible that there were significant differences between clubs that agreed to participate in the study at baseline and those that did not. However, response rates were good and, in the “real world”, only those clubs that are interested and have the capacity will participate in an intervention such as SafeClub. Intervention clubs were larger than control clubs (ie had more teams) and had more young players (ie ⩽12 years), which may have provided them with greater capacity and motivation to improve their safety activities. However, this is unlikely as there was no difference in the size of the committees or annual budgets of the two groups of clubs, suggesting that the human and financial resources available to the two groups were similar. The effects of clustering of clubs by associations were not taken into account in the statistical analysis but, given the magnitude of the differences observed, this is unlikely to have significantly affected the findings.37
CONCLUSION
SafeClub was developed in response to an identified need and is based on sound injury-prevention concepts and adult-learning principles. It was also extensively piloted before evaluation. This evaluation has shown that SafeClub is an effective tool for assisting community soccer clubs in Greater Sydney, Australia to improve their sports-safety activities in a sustainable way. It appears to be particularly effective in assisting clubs to develop and improve the foundations and processes for good risk-management practice. Further research is now required to determine if the success of SafeClub is transferable to other community sports with different organisational and administrative systems and in other geographical locations. Further research is also required to determine if community sports clubs that develop and implement safety plans and policies based on risk-management principles do reduce the risk of injury associated with participation in their club activities. We are planning to develop and implement a dissemination strategy for SafeClub to ensure it is widely available and the quality of its content and delivery are refined and maintained.
Acknowledgments
We thank Soccer NSW and the administrators of participating associations and clubs for their support and participation in this study. We also thank G Cross, who worked as a project officer on this study, and C Finch for statistical and study design advice. S Sherker was supported by a Public Health Research Training Fellowship from the National Health and Medical Research Council, Australia.
REFERENCES
Footnotes
funding: SafeClub was developed and piloted with the assistance of the Safe Community Programs in NSW Small Projects Funding Scheme. This study was partly funded by the NSW Sporting Injuries Committee Research and Injury Prevention Scheme.
Competing interests: None declared..