Article Text

Abstract
Objective To examine the value of isokinetic strength assessment for predicting risk of hamstring strain injury, and to direct future research into hamstring strain injuries.
Design Systematic review.
Data sources Database searches for Medline, CINAHL, Embase, AMED, AUSPORT, SPORTDiscus, PEDro and Cochrane Library from inception to April 2017. Manual reference checks, ahead-of-press and citation tracking.
Eligibility criteria for selecting studies Prospective studies evaluating isokinetic hamstrings, quadriceps and hip extensor strength testing as a risk factor for occurrence of hamstring muscle strain.
Methods Independent search result screening. Risk of bias assessment by independent reviewers using Quality in Prognosis Studies tool. Best evidence synthesis and meta-analyses of standardised mean difference (SMD).
Results Twelve studies were included, capturing 508 hamstring strain injuries in 2912 athletes. Isokinetic knee flexor, knee extensor and hip extensor outputs were examined at angular velocities ranging 30–300°/s, concentric or eccentric, and relative (Nm/kg) or absolute (Nm) measures. Strength ratios ranged between 30°/s and 300°/s. Meta-analyses revealed a small, significant predictive effect for absolute (SMD=−0.16, P=0.04, 95% CI −0.31 to −0.01) and relative (SMD=−0.17, P=0.03, 95% CI −0.33 to −0.014) eccentric knee flexor strength (60°/s). No other testing speed or strength ratio showed statistical association. Best evidence synthesis found over half of all variables had moderate or strong evidence for no association with future hamstring injury.
Summary/Conclusion Despite an isolated finding for eccentric knee flexor strength at slow speeds, the role and application of isokinetic assessment for predicting hamstring strain risk should be reconsidered, particularly given costs and specialised training required.
- Muscle Injury
- Hamstring
- Sport
- Isokinetic
- Assessment
Statistics from Altmetric.com
Introduction
Injuries to the hamstring muscles are prevalent across sports that require high force and high velocity actions such as sprinting and kicking,1–3 along with the capacity to carry out prolonged intermittent and high-speed running.1 4–6
Football (soccer), Australian football and American football consistently report high prevalence and recurrence of hamstring strain injury (HSI).1 7 8 Reinjuries are typically more severe than the index HSI.9 Time lost from training and competition results in deficits in individual and team performance,10 and represents a financial burden for sporting organisations.11 Accordingly, HSIs have been extensively researched.12 13
Isokinetic thigh muscle strength assessment is a popular screening tool for identifying athletes at risk of future HSI,8 14 despite mixed results for its predictive validity.12 13 Some studies found that isokinetic testing could not predict HSI,15 16 while other studies found some predictive ability of isokinetic testing.17 18 Researchers have also explored specific between-muscle strength ratios, with inconsistent results.14 19 A previous meta-analysis of risk factors for HSI indicated that quadriceps peak torque12 was the only parameter, among a number of isokinetic parameters examined, to provide any potential for risk prediction. The limitation of previous meta-analyses was the inclusion of data across only one isokinetic testing speed.12 In addition, further isokinetic strength risk factor studies have been published since this review.8 14 20
Therefore, the aim of this review was to synthesise available literature to examine the value of isokinetic strength assessment for predicting risk of HSI, and to direct future research in this area.
Methods
Search strategy and selection of studies
Systematic database searching was conducted, from database inception to April 2017, across Medline, CINAHL, Embase, AMED, AUSPORT, SPORTDiscus, PEDro and the Cochrane Library (see online supplementary file 1 for an example of search strategy).
Supplementary file 1
Search terms from the research question were mapped to medical subject headings, where possible, and also searched as keywords (table 1). EndNote X3 software (Thomson Reuters, New York, USA) was used to import references and to delete duplicate copies. Two examiners (BDG and TP) independently applied selection criteria to abstracts and titles of the search yield. Additional literature was screened following citation tracking, reference list scanning and ahead-of-press searches in key sports medicine journals (British Journal of Sports Medicine, American Journal of Sports Medicine, Scandinavian Journal of Medicine & Science in Sports and Sports Medicine). Examiners both independently reapplied the selection criteria to full-text versions (BDG and TP) and complete agreement was reached on all articles for inclusion.
Keywords for systematic search
Study selection criteria
Participants/Injury
Articles that examined athletes or athletic populations and subsequent occurrence of a primary or recurrent hamstring muscle strain injury during a sport or competition-related activity were included. Discrete isokinetic strength data for participants sustaining these injuries were required for inclusion. Studies examining hamstring muscle strains were distinguished from tendinopathy, contusion-type injuries or other non-specific thigh conditions, and these other injuries were excluded.
Isokinetic strength and risk
Included studies were required to examine one or more isokinetic strength variables and their association with HSI. Peak torque variables, strength ratios and asymmetries from the hamstrings, quadriceps and hip extensors were included. Specific strength ratios examined included (1) conventional hamstrings: quadriceps (HS:Qu); (2) functional HS:Qu; (3) hamstrings:opposite hamstrings (HS:Opp HS); and other mixed approaches. Conventional HS:Qu ratios are calculated from the concentric torques generated by the knee flexors and knee extensors at a given contractile velocity. Functional HS:Qu ratios are calculated from the eccentric knee flexor torque and the concentric knee extensor torque. All contractile velocities were accepted (30–300°/s) to capture the influence of different testing parameters on the risk of future HSI.
Study type
Descriptive, epidemiological, intervention-only or case studies, systematic reviews, non-systematic reviews, and opinion articles were not included. Full-text versions from peer-reviewed sources were required to enable rigorous methodological appraisal. Abstract-only or unpublished data were not accepted. Studies required an English version.
Data collection and analysis
Risk of bias assessment
Two reviewers (BDG and MNB) independently used a modified version of the Quality in Prognosis Studies (QUIPS) tool for risk of bias assessment of all included studies. Any discrepancies were evaluated by a third reviewer (TP). The QUIPS tool has been previously outlined in the literature,21 22 including application in a recent hamstring-related systematic review.23 Potential sources of bias are examined according to six subheadings: study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, and statistical analysis and reporting (online supplementary file 2). Each of the six study design elements are appraised according to specific criteria used to determine degree of risk, and are scored ‘yes’ or ‘no’. If a single category scores less than 75% of ‘yes’ responses, it is deemed to have a ‘High Risk’ of bias for that single aspect of study design. Conversely, ‘Low Risk’ of bias is determined if there is greater than or equal to 75% of ‘yes’ responses. Subsequently an overall level of risk for a study is calculated according to the number of categories falling within the high and low risk of bias classifications. Studies having satisfied at least five out of six bias categories and having satisfied item 4 (outcome measurement) are deemed to have an overall low risk of bias. This method has been used in previous reviews of hamstring injury.23 24
Supplementary file 2
Data extraction
Data extraction focused on risk of sustaining a future HSI and specific isokinetic strength variables, including differentiation between angular velocities and contraction mode(s). Where possible, raw data relating to absolute (Nm) and relative (Nm/kg) torque from specific angular speeds and the contraction mode were diverged to identify risk for particular sets of contractile conditions. Data were also extracted for methods of injury diagnosis, study duration and key results relating to HSI prediction. Independent data extraction was carried out by non-blinded reviewers (BDG and TP) and was used to determine the overall heterogeneity between studies.
Data analysis and best evidence synthesis
Mean values, standard deviations (SD), relative risk and risk ratios (RR), odds ratios (OR), and associated 95% CIs were extracted. For continuous data, standardised mean difference (SMD) and 95% CIs were calculated by dividing the means of the injured and uninjured groups by the pooled SD. SMD provides an indication of the between-group difference in strength outputs for a given torque variable, in athletes who did and did not sustain a subsequent hamstring strain. Data not suitable for meta-analyses were used in the best evidence synthesis to determine the nature of association between each isokinetic variable and HSI risk.
Where possible, meta-analysis was performed using Comprehensive Meta-Analysis V.2.0 (Biostat, Englewood, New Jersey, USA) software. A random-effects model was incorporated to account for potential methodological or statistical heterogeneity affecting the strength or direction of results. A random-effects approach ensures there is limited influence or assumptions of causes of variance in sample distributions. This results in statistically clearer and more accurate data sets around pooled effect sizes.25 The I2 statistic was employed to assess heterogeneity between pooled studies.26 Pooled SMDs were interpreted to identify small (≤0.2), moderate (0.21–0.5) and large (≥0.8) effect sizes.27 Statistical significance was set at P<0.05.
A best evidence synthesis was undertaken, as described previously,28 29 to determine the strength of relationships between all variables since not all studies could be included in meta-analyses due to insufficient data or substantial heterogeneity. Results of the best evidence synthesis were used to improve the interpretation of data derived from meta-analyses and original data extracted from included studies. Strength of evidence was stratified according to five hierarchical criteria listed below. Similar criteria have been used in previous hamstring-related systematic reviews.23 24
Strong evidence: consistent results in two or more low risk of bias studies, with generally consistent findings in ≥75% of studies.
Moderate evidence: one low risk of bias study and one or more high risk of bias studies that provide consistent findings, or consistent findings reported in two or more high risk of bias studies with consistent results in ≥75% studies.
Limited evidence: single-study findings from either a high risk or low risk of bias study.
Conflicting evidence: multiple studies (of either high or low risk of bias) that do not provide consistent results, with consistent results in <75% studies.
No evidence: no randomised controlled trials or non-randomised controlled trials available for assessment.
Results
Search results
Following removal of duplicates, 595 articles from the initial search yield underwent title and abstract screening. Application of selection criteria resulted in 53 studies for further analysis in full-text form. Subsequent application of criteria to full texts resulted in nine studies for inclusion. Manual reference checks, citation tracking and ahead-of-press searching highlighted an additional three studies, resulting in a final yield of twelve studies to be included8 14–20 30–33 (see figure 1 for full search flow diagram).

Search flow diagram.
Description of the included studies
This body of literature captured 508 HSIs in 2912 participants across Australian rules football,16 17 30 football (soccer),14 15 18–20 American football,8 rugby31 and sprinting32 33 (table 2).
Characteristics of the included studies
Risk of bias assessment
A high risk of bias was found in six studies.16–18 20 30 31 The remaining six8 14 15 19 32 33 were determined to have a low risk of bias (table 3). Complete agreement on all items of bias assessment was reached by all authors (BDG, TP and MNB). Full details of the scoring of assessment using the QUIPS tool are provided in table 3. When considering overall key sources of study bias, ‘confounding variables’ was the most consistent area determined to elevate risk (75% of studies).
Risk of bias assessment
Overview of best evidence synthesis results
The results of the best evidence syntheses identified that for 20 of the 38 isokinetic strength variables, there was either moderate or strong evidence for no association with future HSI (table 4). There was limited evidence for no association between 14 strength variables and HSI and conflicting evidence for an unknown association for three variables. There was limited evidence for a single variable (concentric hip extensors at 60°/s) as a predictor of HSI risk; however, findings were reported in only one study.33 Furthermore, no strength ratio or imbalance measure was associated with future HSI.
Results of best evidence synthesis
Overview of results from meta-analyses
Eighteen meta-analyses were performed across the twelve studies. The associations between isokinetically derived measures of hamstring (figure 2), quadriceps (figure 3), and strength ratio or imbalance (figure 4) torque variables and future HSI are displayed graphically. With the exception of a small, significant predictive effect for absolute and relative eccentric knee flexor torque (at 60°/s) (figure 2), there were no statistically significant effects for any of the 16 other measures.

Hamstring strength variables grouped meta-analyses. HS, hamstring; SMD, standardised mean difference. *P<0.05.

Quadriceps strength variables grouped meta-analyses. Qu, quadriceps; SMD, standardised mean difference.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
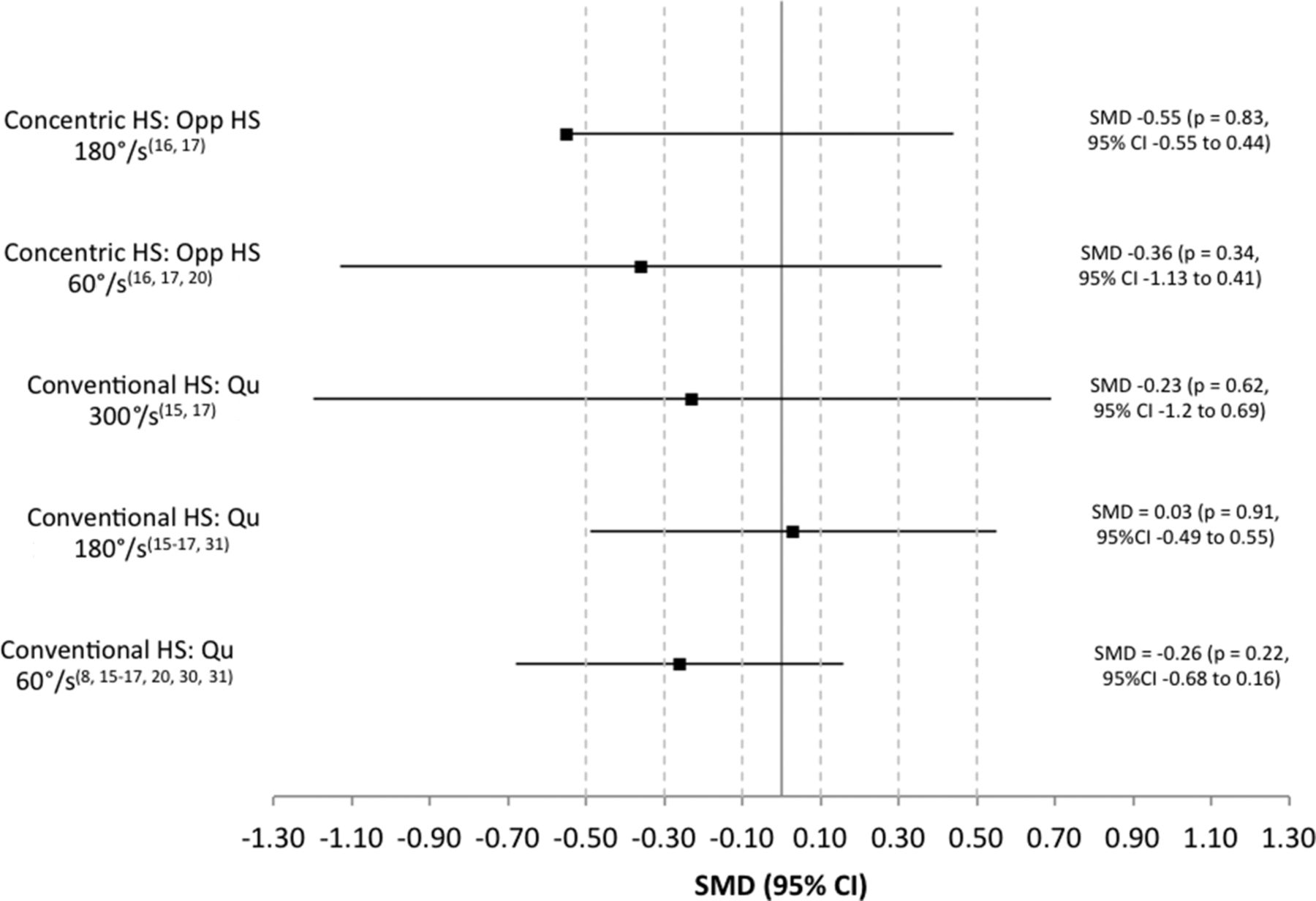
Strength ratio variables grouped meta-analyses. HS, hamstring; Opp, opposite; Qu, quadriceps; SMD, standardised mean difference.
Discussion
Across the 18 meta-analyses, there were only two significant findings: small, significant effects for absolute and relative eccentric knee flexor weakness at 60°/s to predict future HSI. In contrast, best evidence synthesis found evidence for no association between eccentric knee flexor strength (at 60°/s) and HSI. This finding may highlight the statistical influence on the meta-analysis result from a single study with a considerably larger subject pool and HSI numbers than the other studies.
Best evidence synthesis of all 38 isokinetic variables identified that 53% displayed moderate to strong evidence for no association with HSI risk. Limited evidence for no association was found for 36% of variables, while 8% had conflicting evidence for an unknown association. Only one variable (3% of all) suggested the potential presence of an association with future HSI (concentric hip extensor 60°/s), with the strength of this evidence deemed to be limited. Hip extensor peak torque was only evaluated in one study and may warrant further research.
Knee extensor (quadriceps) weakness was not a predictor of future HSI in the current analyses, which is in contrast with a previous review.12 This is likely the result of the recent addition of further key prospective data in this area.8 14 20 The best evidence synthesis supported our meta-analysis findings, with either moderate or strong evidence for no association between all quadriceps strength measures and future HSI.
Isokinetic testing may not be best suited to detect the influence of strength in future HSI, due to factors relating to the test position and control of both contractile speed and mode. The test position is thought to replicate late swing stage. However it may not detect specific deficits present in function, particularly those that underpin building locomotive velocity from lower speed running to sprinting.34 35 Control of contractile speed and contractile mode may further constrain optimal behaviour of the musculotendinous unit during the stretch-shortening cycle and limit expression of force in the way it occurs dynamically.36 37 The absence of a predictive ability of isokinetic testing does not indicate that hamstring muscle properties are not important to HSI risk. Alternative testing methods measure strength-related factors predictive of future HSI, particularly eccentric hamstring torque generating capacity,3 5 38 39 and should be investigated further. It is likely that injury-risk moderation and performance involves complex interplay between numerous lower limb strength-based attributes,40 41 tissue architectural characteristics38 and player loading indices.6 42 43
In conjunction with other hamstring assessment tools, such as NordBord3 5 38 and hand-held or externally fixed dynamometry,39 44 isokinetic testing may have a role in secondary prevention strategies or with staging rehabilitation prior to return to sport.45 Given the significant eccentric strength changes across preseason and in-season periods,3 strength testing modalities should have the capacity for repeat measures to be taken in ongoing monitoring and screening practices.45 However, in light of the findings presented here, and given the significant time requirements and costs associated with isokinetic testing,46 this form of testing represents an unlikely and impractical means of screening athletes at risk of HSI for many clubs and clinicians.
Isokinetic strength asymmetries or imbalances were not associated with future risk of HSI. Similarly, there was no significant relationship with any strength ratio tested, despite previous reports and isolated study findings.17 19 This is consistent with recently published results, including risk examined against specified strength ratio cut-offs, showing a lack of predictive validity for detecting risk of hamstring muscle injury.20 Strength ratio calculation may have a more practical role elsewhere. Clinical applications may include athlete monitoring or profiling in response to training loads, according to the needs of the specific sport, or to individual attributes that may predispose to injury.6 42 43 45 47
Limitations of this review include the potential for publication and language biases. Studies were required to be published and written in the English language, which could have resulted in fewer studies than are available on the topic of isokinetic strength testing for HSI prediction.
Conclusion
This systematic review identified that the overall role of isokinetic strength assessment for detecting the risk of future hamstring muscle injury is limited. Based on the results of meta-analyses, slow speed isokinetic eccentric knee flexor strength testing may be of limited benefit. However, the best evidence syntheses combined with considerations around costs and specialised training needed to carry out isokinetic strength testing may preclude its use as a screening tool.
What is already known on this topic?
Hamstring strain injuries continue to be a considerable issue, impacting on team and individual successes.
Different measures of strength and strength ratios are gaining increasing attention in their relationship with hamstring injury risk.
Isokinetic strength assessment has been reported to have a potential association with HSI risk.
What are the findings?
There may be a small, predictive effect for relative and absolute isokinetic eccentric hamstring strength (at 60°/s) in detecting subsequent hamstring strain risk.
No other measure of hamstring, quadriceps or hip extensor torque-generating capacity was determined to have a significant relationship with risk for hamstring injury.
No strength ratio or measure of imbalance or asymmetry was determined to possess a significant association with HSI risk, including the well-researched conventional and functional hamstrings:quadriceps strength ratios.
The role of isokinetic strength assessment for detecting hamstring strain risk is limited, and future research and athlete monitoring practices in this area may be better focused elsewhere.
References
Footnotes
Contributors All authors made equal contributions to the work. All authors gave permission for the final version to be submitted.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.