Article Text

Abstract
Background Alterations in scapular orientation and dynamic control, specifically involving increased anterior tilt and downward rotation, are considered to play a substantial role in contributing to a subacromial impingement syndrome (SIS). Non-surgical intervention aims at restoring normal scapular posture. The research evidence supporting this practice is equivocal.
Objective The aim of this study was to systematically review the relevant literature to examine whether a difference exists in scapular orientation between people without shoulder symptoms and those with SIS.
Data sources MEDLINE, AMED, EMBASE, CINAHL, PEDro and SPORTDiscus databases were searched using relevant search terms up to August 2013. Additional studies were identified by hand-searching the reference lists of pertinent articles.
Review methods Of the 7445 abstracts identified, 18 were selected for further analysis. Two reviewers independently assessed the studies for inclusion, data extraction and quality, using a modified Downs and Black quality assessment tool.
Results 10 trials were included in the review. Scapular position was determined through two-dimensional radiological measurements, 360° inclinometers and three-dimensional motion and tracking devices. The findings were inconsistent. Some studies reported patterns of reduced upward rotation, increased anterior tilting and medial rotation of the scapula. In contrast, others reported the opposite, and some identified no difference in motion when compared to asymptomatic controls.
Conclusions The underlying aetiology of SIS is still debated. The results of this review demonstrated a lack of consistency of study methodologies and results. Currently, there is insufficient evidence to support a clinical belief that the scapula adopts a common and consistent posture in SIS. This may reflect the complex, multifactorial nature of the syndrome. Additionally, it may be due to the methodological variations and shortfalls in the available research. It also raises the possibility that deviation from a ‘normal’ scapular position may not be contributory to SIS but part of normal variations. Further research is required to establish whether a common pattern exists in scapular kinematics in SIS patients or whether subgroups of patients with common patterns can be identified to guide management options. Non-surgical treatment involving rehabilitation of the scapula to an idealised normal posture is currently not supported by the available literature.
- Shoulder injuries
- Sports physiotherapy
Statistics from Altmetric.com
Introduction
Shoulder pain is associated with substantial morbidity. The reported point prevalence ranges between 7% and 27% in the general population and it is thought to increase with age.1 Subacromial impingement syndrome (SIS) and rotator cuff tendinopathy are considered to be the most common causes of shoulder pain. Their point prevalence has been estimated to be between 2.4% and 14%.2 SIS has been shown to affect both manual and sedentary workers3 ,4 as well as sporting populations.5
The term SIS encompasses shoulder pain and pathology originating from the tendon or bursal tissue in the subacromial space, but its aetiology is still not fully understood. The symptoms experienced in SIS may be due to extrinsic,6 ,7 intrinsic8 or a mixed aetiology.9 ,10 The condition is typically diagnosed clinically using a combination of impingement or rotator cuff tests; however, the diagnostic accuracy of these tests has not been confirmed.11–,13
One hypothesis is that scapular dyskinesia is involved in the pathogenesis of SIS by reducing the subacromial space creating mechanical impingement of the subacromial tissue, thus resulting in pain and dysfunction.14 ,15 The rehabilitation of scapula-stabilising muscles is commonly prescribed for the management of SIS.16 ,17 However, the findings of studies which have examined changes in the activation patterns of muscles of the shoulder complex and those controlling the scapula in people with SIS have been equivocal. A recent systematic review of nine electromyographic (EMG) studies of the shoulder complex in people with SIS concluded that a difference between the upper and lower trapezius EMG activity may exist when compared to people without symptoms, whereas evidence did not exist or was inconsistent for supraspinatus, teres minor, serratus anterior, deltoid and biceps.18 These variations in findings may represent the multifactorial aetiology of SIS or, alternatively, may be due to the small study sizes and methodological factors failing to detect change.
An alternative method to investigate the relationship between SIS and posture is to explore the relationship between scapular orientation and symptoms. The literature has associated an anteriorly tilted, downwardly rotated scapular orientation with SIS.17 ,19 ,20 Early studies investigating scapular orientation analysed static measurements derived from bony landmarks on radiographs.21 ,22 These studies identified that differences existed between asymptomatic and symptomatic shoulders in scapular orientation at different points in arm elevation. With the development of measurement techniques, three-dimensional (3D) motion recording methods have enabled a more accurate representation of multiplanar scapular motion.23 This investigation aims to systematically review the available research on scapular orientation in people with SIS when compared to those without symptoms, in order to establish whether a relationship between scapular position and SIS exists.
Methods
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed when conducting this systematic review.24 ,25 To avoid a bias of predicting and directing the study towards a desired outcome, the methodology was formulated a priori.26
Literature search
A search of the literature was performed using the following databases
-
MEDLINE and In Process and Other Non-Indexed Citations and Ovid MEDLINE, from 1946 to 26 August 2013
-
Allied and Complementary Medicine Database (AMED), from 1985 to 26 August 2013 (through OVID)
-
ExcerptaMedica Database (EMBASE), from 1980 to 26 August 2013 (through OVID)
-
Citation Index for Nursing and Allied Health Literature with full text (CINAHL plus with full text) 1981 to 26 August 2013 (via the EBSCOhost)
-
PEDro, 1929 to 26 August 2013 as per criteria for inclusion to database
-
SPORTDiscus 1939 to 26 August 2013 (via the EBSCOhost)
Subject headings and free text search terms were used to search for relevant articles. These included variations of the following: shoulder joint; shoulder; shoulder pain; scapula; shoulder impingement syndrome; SIS; rotator cuff; bursitis; orientation; biomechanics; imaging; movement; posture; and kinesiology. The full Medline search strategy is presented in the online supplementary appendix.
Study selection
The following inclusion and exclusion criteria were applied to the articles.
The titles and abstracts were screened by the first reviewer (ER), and papers were identified based on the relevance of the study in relation to the population, intervention and outcomes detailed in the title and abstract. Full text copies were obtained for the selected studies and for those where relevance was not clearly identifiable in the abstract and title. The electronic search was then supplemented by manual searches of the reference lists of these articles. The selected articles were further assessed in a non-blinded and standardised manner by the first and second reviewers for their eligibility (ER and SP). The inclusion and exclusion criteria (summarised in table 1) were applied. Disagreement was reconciled by a third reviewer (JL/SM).
Inclusion and exclusion criteria
Quality assessment
Studies meeting the above inclusion criteria were assessed for quality using the Downs and Black Checklist (1998).27 In its entirety, this appraisal tool is a 27-point checklist and is divided into five subscales comprising: assessment of adequate reporting (10 items); external validity (3 items); internal validity detailing measurement and outcome bias (7 items); confounding (6 items); and power (1 item). It has a maximum score of 32, with each item scoring 0 or 1, except for a 2 point score for fully describing the distribution of principal confounders, and a possible 5 point score for sufficient power calculation. Most of these items pertain to any type of study design, but three items (known confounders, main outcomes and sample size) are design specific and customised by raters.28 The Downs and Black Checklist has been shown to have moderate to good inter-rater reliability.27 ,28 For the purpose of this study, the tool was modified by eliminating two items relating to randomisation and allocation concealment,28 and also by changing the final item from a score of 0–5 to a scale of 0–1. There was a score of 1 if a power calculation or sample size calculation was provided, and 0 if there was no power calculation, sample size calculation or explanation whether the number of participants was appropriate.29 The total maximum score of the modified checklist used in this review was 26.
Each included study was initially assessed by two independent reviewers and scored using the modified checklist. Subsequently, if required, a consensus score was reached after discussion.
The Downs and Black Checklist itself does not provide bandings for levels of quality.27 Various quality rating categories have been suggested, such as using the median values of percentage scores,30 or assigning the following ordinal categories: low (≤33.3%), moderate (33.4–66.7%) and high (≥66.8%).28 The latter categorisation was chosen for this systematic review.
Data extraction and synthesis
Data extraction was carried out by the first reviewer (ER) and checked by the second reviewer (SP), using predesigned and standardised forms.26 ,31
After data extraction, the final inclusion and exclusion decisions were made regarding the study, referenced against the predetermined criteria (table 1), and this decision was detailed on the data extraction forms. The information is detailed in table format to highlight the similarities and differences within the study designs, objective, subject population and control, measurement and outcome measure. Two tables detail this information. Online supplementary table S1 details the study characteristics and online supplementary table S2 details the outcomes.
While the approach used to conduct this review was guided by the PRISMA statement, the heterogeneity in the studies did not allow for a meta-analysis, and therefore a narrative review was performed.
Results
The initial database searches identified 7445 abstracts, and of these 1106 were identified as duplicates and removed. Eighteen articles were deemed relevant based on their title, abstract or both. Two were removed as the main body of the study was not in English.32 ,33 Full text articles were retrieved for 16 studies, 10 of which satisfied the inclusion and exclusion criteria and were included in this review (table 2); 6 were rejected.34–39 Of the six articles, one had required arbitration and it was rejected from this study on the basis of the diagnostic criteria used for the subject sample.37 Of the ten studies, two shared the same participants and because of this, these studies were combined during analysis.40 ,41
Included studies
The selection process is displayed in figure 1.
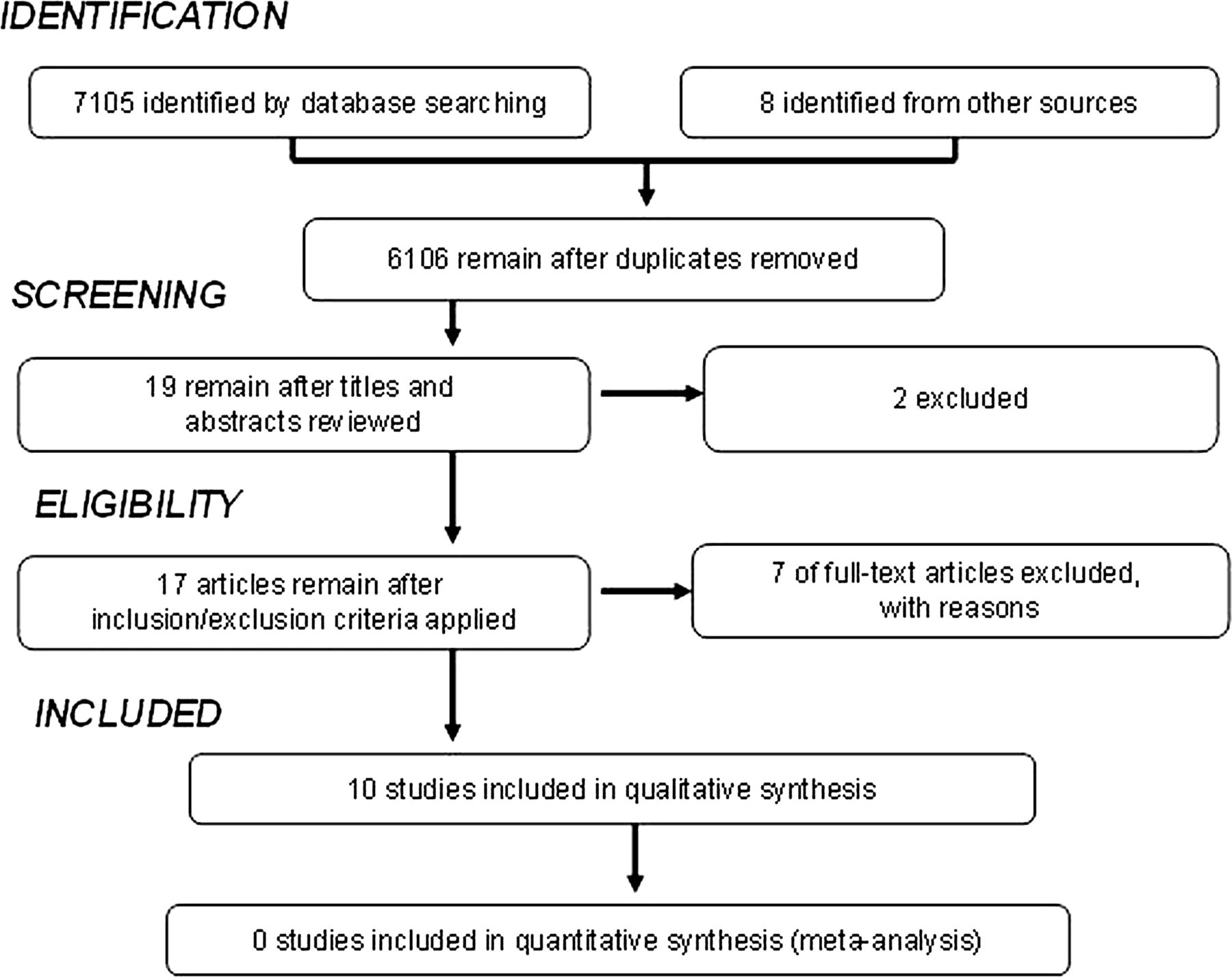
{kind=link}
Depicts the identification, screening, eligibility and inclusion phases of the study selection process in this systematic review.
Methodological quality
The 10 selected investigations were scored using the modified quality assessment tool. Uncertainties were discussed and consensus was reached, resulting in incomplete consensus between raters. The results are shown in table 3.
Results of Downs and Black Checklist Application in the included studies
Articles relating to the same cohort40 ,41 had their scores combined to prevent bias. The quality scores ranged from 14/2642 to 19/26,43 with three studies40 ,41 ,43 being deemed to be of high quality and the remainder of moderate quality. All 10 articles were therefore considered in this review. The most common methodological flaws were: (1) not including an acknowledgement of whether or not there were any adverse effects on the measurement process (criterion 8, table 3); (2) poor description of the source population and recruitment process (criteria 11and12, table 3); (3) not describing the environment where the studies took place (criterion 13, table 3); and (3) not stating whether the rater was blinded to the study group during measurements (criterion 15, table 3).
Only one study had a follow-up period,43 so applying criteria 9 and 12 had limited value for the remaining studies.
Study characteristics
Of the 10 studies included in this review, the sample size ranged from 2142 to 90.44 In two studies,45 ,46 56 participants compared the symptomatic shoulder to the asymptomatic contralateral side, and therefore the total number of participants was 370. The age range of the participants with SIS was 17–74 years, compared with 19–74 years in the control group. The duration of symptoms was noted in only four studies40 ,41 ,43 ,46 and ranged between 2 weeks and 8 years. Six of the studies considered the degree of pain and disability resulting from SIS, and this was measured by the: Shoulder Pain and Disability Index (SPADI);40 ,41 ,47 Wheelchair Users’ Shoulder Pain Index (WUSPI);48 Neer & Welsh Swimmers’ Shoulder Grading System43; visual analogue scale (VAS) for pain44; Flexilevel Scale42; and the American Shoulder and Elbow Surgeons’ Self-Report Form.44 Participants were recruited from a number of populations including hospital clinics,44–,47 sports teams (swimming and baseball),42 ,43 construction industries40 ,41 and wheelchair users.48
Methods of assessing scapular orientation
Various methods of assessing scapular orientation were employed. Orientation and motion of the scapula were measured by 3D electromagnetic motion systems using surface electromagnetic sensors40–,42 ,44 ,47 ,48 and infrared probing system,46 plane radiographs,45 360° inclinometer43 and Moire topography.49 Of the six studies which used 3D electromagnetic motion systems, only four studies (2 of which were combined) used the same landmarks for sensors and axis coordinates to determine scapular position and motion.40–,42 ,44 Of these four studies, scapular orientation and motion were measured during arm elevation in the scapular plane40 ,44 ,47 and when lowering the arm.41
Results of the studies
Six studies were deemed to be of moderate quality42 ,44–,49 and three were of high quality;40 ,41 ,43 however, conflicting findings were identified. These findings are described in online supplementary table S2.
Upward rotation of the scapula
When compared to participants without symptoms, people with SIS displayed increased scapular upward rotation during elevation of the arm48 and functional activities,44 whereas other studies reported decreased scapular upward rotation during elevation in the scapular plane40 ,43 and into abduction above 90°.45 It may be of relevance that the latter had a higher proportion of higher quality trials. No difference was found in scapular upward rotation in further studies investigating elevation of the arm in the scapular plane,42 abduction and flexion46 and when lowering the arm from an elevated position.41 Su et al43 along with Ludewig and Cook,40 both deemed high quality in this review, reported that scapular dyskinesia may be demonstrated more prominently after fatigue or when movements are repeated under load.
Scapular anterior –posterior tilt
A decreased posterior tipping angle, that is, a position of relative anterior tipping of the scapula was demonstrated in two studies which were found to be of moderate quality.42 ,47 A high-quality study by Ludewig and Cook40 found no difference between groups, but anterior tipping of the scapula increased when re-examined under loaded conditions. Borstad and Ludewig41 reported no difference between groups under test conditions in their high-quality study. Conversely, one further study,44 of moderate quality, found that SIS displayed more posterior tilt than the control group during flexion and elevation in the scapular plane.
Scapular elevation
Lin et al42 reported increased scapular elevation in baseball players with SIS, as did Warner et al49 during dynamic assessment under load of a patient population. Both studies were found to be of moderate quality for the purpose of this study. Their conclusions are supported by further studies47 ,44 where scapular orientation was evaluated during static positions in elevated positions rather than continuous motion. This may have resulted in fatigue and hence a greater likelihood of demonstrating a significant difference when compared to the control group.
Discussion
The results of this systematic review demonstrate a distinct lack of consistency in their methodologies and results. While some studies reported altered scapular kinematics in SIS subjects, these results are challenged by an equal number reporting contradictory findings. There is no clear explanation for this. They may have occurred as a result of: the multifactorial nature of SIS;50 the considerable difficulty in establishing a diagnosis of SIS;11–,13 ,51 ,52 the uncertainty in the definitive relationship between SIS and posture53; the various methods of measuring scapular position41 ,47; a lack of reporting the definitive reliability of the measurements used49; and reporting differences in scapular position without reporting if the differences were greater than the clinical error of measurement, such as the SE of measurement.54 It is also raises the possibility that the results of this study, along with other studies, challenge the certainty that an ideal scapular position exists and deviation causes or contributes to SIS.8 ,55
It may be argued that the increased scapular upward rotation44 ,48 and posterior tilting of the scapula44 found in some studies may be explained as a consequence of SIS to reduce compromise of the subacromial tissues. Other features thought to be associated with SIS, such as the intrinsic manifestations of tissue oedema and thickening and fibrosis within the subacromial space, may result in adaptive movement patterns to compensate for the increased volume in the space. The acromiohumeral distance has been reported to be as little as 4.1 ± 2.5 mm.14 Consequently, a small change in the local tissue swelling may have a substantial impact. Conversely, studies which found a reduced scapular upward rotation,40 ,43 increase in anterior tipping42 ,47 and increase in medial scapular rotation40 ,41 ,46 ,49 may have contributed to the cause of the condition, narrowing the subacromial space and resulting in mechanical impingement of the tissue. These could be the cohort of patients who may benefit from a focused scapular rehabilitation programme,16 ,17 which is a common procedure in the non-surgical management of SIS.
The methodological variability of the 10 studies included in this review did not permit us to draw definitive conclusions. Ludewig and Cook40 and Borstad and Ludewig41 investigated men working in the construction industry, so it may not be appropriate to extrapolate their findings to other patient groups. Similarly, studies involving swimmers43 and baseball players42 are also limited to specific subgroups. Only two studies provided evidence of a power calculation,40 ,41 which may suggest that the conclusions reached in other studies are based on inadequate sample sizes, which in turn reduce the ability to reach definitive conclusions. Limited information on the sample population and selection process of recruits in studies reduced some quality scores.
This systematic review of the research investigating scapular orientation and kinematics in people diagnosed with SIS, when compared to asymptomatic controls, concludes that a synthesis of the current research findings suggests that no definitive relationship exists between scapular orientation and SIS. Clinicians assessing scapular position in this patient group and making recommendations to rehabilitate the scapula to an idealised normal position must do so with caution and with the knowledge that no definitive abnormal position has been identified with certainty. Unquestionably, substantially more research is required to further our understanding on the relationship between scapula position and SIS.
Future research is required which combines dynamic scapular tracking, EMG and pain perception in people with symptoms of SIS, in comparison to appropriately-sized populations of people without symptoms. These studies should balance the number of participants with dominant and non-dominant hands, in addition to accounting for differences in age, activity and body proportion. This would help provide the information that is required to better understand if an association between scapular position and SIS exists. Robustness of findings would be improved if those assessing were blinded to the subject’s status and reliability of assessment demonstrated. Standardising reliable measurement methods may in turn allow results and a meta-analysis to be performed in the future.
The limitations of this study may have resulted from a narrative approach being followed. This type of review was conducted due to the heterogeneity of the studies reviewed. In addition, the absence of consensus on the choice of a quality assessment tool with scientific rigour for this type of study resulted in the selection of a modified Downs and Black Checklist. Although elements of these modifications have been measured against other tools for reliability and validity,28 as well as used in other publications,29 more studies are needed to evaluate this further.
Conclusions
In conclusion, the underlying aetiology of SIS is still debated. The results of this review show a lack of consistency of the study methodologies and results. Currently, there is insufficient evidence to demonstrate that consistent patterns of scapular dyskinesia in SIS exist. This may be a reflection of the complex, multifactorial nature of the syndrome or it may be due to the methodological shortfalls in the available research. It also raises the possibility that deviation from a ‘normal’ scapular position may not be contributory to SIS but part of normal variations.
Ongoing research is required to establish whether there is a common pattern in scapular kinematics in SIS patients, or whether subgroups of patients exist and can be identified to guide management.
What are the new findings?
-
The results of this review demonstrate a lack of consistency of study methodologies and results.
-
This synthesis of the current research findings suggests that no definitive relationship exists between scapular orientation and subacromial impingement syndrome.
-
There is insufficient evidence to support a clinical belief that the scapula adopts a common and consistent posture in the subacromial impingement syndrome.
How might this impact on clinical practice in the future?
-
Further research is required to establish whether a common pattern exists in scapular kinematics in patients with subacromial impingement syndrome or whether subgroups of patients with common patterns can be identified to guide management options.
-
Non-surgical treatment involving rehabilitation of the scapula to an idealised normal posture is currently not supported by the available literature.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online table 1
- Data supplement 3 - Online table 2
Footnotes
-
Contributors ER conceived the study and was the primary reviewer, extracted and analysed the data and was the primary author. SP was the second reviewer. SM contributed to the design of the study and resolution of uncertainties regarding data extraction and analysis. JL contributed not only to the design of the study and the resolution of uncertainties regarding data extraction and analysis, but was also involved in the writing up of the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Warm up
- Corrections