Article Text

Abstract
Objective To determine the effectiveness of mindfulness-based programmes (MBPs) on the mental health of elite athletes.
Design Systematic review and meta-analysis.
Data sources Eight online databases (Embase, PsycINFO, SPORTDiscus, MEDLINE, Scopus, Cochrane CENTRAL, ProQuest Dissertations & Theses and Google Scholar), plus forward and backward searching from included studies and previous systematic reviews.
Eligibility criteria for selecting studies Studies were included if they were randomised controlled trials (RCTs) that compared an MBP against a control, in current or former elite athletes.
Results Of 2386 articles identified, 12 RCTs were included in this systematic review and meta-analysis, comprising a total of 614 elite athletes (314 MBPs and 300 controls). Overall, MBPs improved mental health, with large significant pooled effect sizes for reducing symptoms of anxiety (hedges g=−0.87, number of studies (n)=6, p=0.017, I 2=90) and stress (g=−0.91, n=5, p=0.012, I 2=74) and increasing psychological well-being (g=0.96, n=5, p=0.039., I 2=89). Overall, the risk of bias and certainty of evidence was moderate, and all findings were subject to high estimated levels of heterogeneity.
Conclusion MBPs improved several mental health outcomes. Given the moderate degree of evidence, high-quality, adequately powered trials are required in the future. These studies should emphasise intervention fidelity, teacher competence and scalability within elite sport.
PROSPERO registration number CRD42020176654.
- athletes
- psychiatry
- meta-analysis
- psychology, sports
Statistics from Altmetric.com
Introduction
Elite athletes face unique stressors that can place them at particular risk of experiencing mental health symptoms and disorders, with the prevalence of common mental health symptoms equivalent to or even or exceeding that of non-athletes.1–3 A developing tension between protecting athletes’ mental health and striving for optimal performance has brought renewed focus on this subject,4–6 prompting fresh calls for mental health to be prioritised alongside physical health.7 Comprehensive screening and monitoring tools are available.8 The International Olympic Committee Sports Mental Health Assessment Tool-19 is becoming widely used as a framework to identify and treat mental health symptoms and disorders in elite athletes.10 11 Mindfulness and meditation are cited as potential treatment options for athletes who are experiencing high psychological strain but do not meet the criteria to be diagnosed with a clinical disorder.9 Recommended treatment options should, therefore, be rigorously tested in elite athletes and the unique environments in which they operate.5 12 13
Mindfulness-based programmes (MBPs) such as mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT) aim to improve dimensions of mindfulness including attentional control, acceptance, emotional reactivity and self-compassion.14 15 They are comparable to other evidence-based approaches, such as cognitive–behavioural therapy, in treating mental health disorders.16 17 Mental health represents a spectrum from ‘flourishing’ to ‘languishing’.18 An individual may experience positive states of well-being (flourish) while living with a mental health disorder, or experience poor mental health (languish) in the absence of clinically relevant symptoms of a mental health disorder.8 18 MBPs teach foundational skills that support mental health and well-being across this spectrum.19 MBSR and MBCT typically consist of eight sessions per week, each lasting 2.0–2.5 hours, and are delivered in group settings by teachers who have successfully completed mindfulness-based teacher training.20 MBPs are associated with improvements in athletic performance, making mindfulness-based approaches popular in contemporary sports psychology.21–23 Careful adaptation of these programmes is required when targeting specific new groups and new contexts, such as elite athletes, to maximise acceptability, effectiveness, ease of implementation and scalability.24 The adaptation of MBPs to elite sport settings must take into account the impact at the level of the individual, as well as at the micro (coaches/teammates), meso (individual sport) and macro (wider sporting environment) levels.8 25
Important critiques of mindfulness highlight that commercialisation and overstating evidence have contributed to scepticism towards MBPs.26 A further critique is that mindfulness puts too much responsibility on individuals27 and fails to address the social determinants of mental health, such as socioeconomic disadvantage, structural racism, sexism and gender/sexuality discrimination.28 If MBPs are to be used to improve elite athletes’ mental health, the best available evidence first needs to be systematically evaluated. Hence, the objective of this review was to determine the effect MBPs had on elite athletes’ mental health.
Methods
This review was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines,29 and the implementing PRISMA in Exercise, Rehabilitation, Sports Medicine and Sports Science guidance.30 The protocol was registered via the Centre for Reviews and Dissemination (PROSPERO: CRD42020176654, 17 November 2020). Deviation from the original protocol occurred after data synthesis. We chose not to analyse secondary outcomes, which included performance and injury, because there were sufficient data for the primary mental health-related outcomes.
Eligibility criteria
Studies were selected with no restrictions on dates, country or language, if they had a randomised controlled trial (RCT) design, exclusively included current/former elite athletes of any age and compared a MBP to a control. Studies were excluded if they were not RCTs or were quasi-randomised, if the sample population were non-elite athletes or included a mix of elite/semielite/recreational athletes, and if the MBP was brief (<4 weeks).
Participants were elite athletes, classified as full professional, national, international or Olympic competitors, or involved in national or professional development training/competitions if under the age of 18.31 Student athletes were classified as elite if they were part of a university elite sport programme. For the USA, this was restricted to National Collegiate Athletic Association (NCAA) Division 1. MBPs had to meet the requirements detailed by Crane and colleagues,32 including being at least 4 weeks in length. All comparators, active or passive, were considered. Six primary outcomes were selected and between-group differences were analysed for (1) anxiety symptoms, (2) depression symptoms, (3) psychological distress, (4) stress, (5) psychological well-being and (6) mindfulness.
Anxiety and depression were included as these are the most commonly reported mental health symptoms and disorders in athletes.1 Psychological distress was included as a broader indicator of mental health that encompasses symptoms of anxiety, depression and negative affect.33 Stress was included because elite athletes are regularly exposed to environmental demands that surpass their adaptive capacity, contributing to stress,34 35 and high levels of stress are associated with mental health disorders in athletes.36 37 These four outcomes were combined to produce an overall mental health outcome that represented the accumulative effect of MBPs on mental health symptoms and disorders. Moving beyond the conceptualisation of mental health as merely the absence of symptoms or disorders,38 we included psychological well-being as a complex construct that includes optimal functioning and experience.39–41 Mindfulness reduces stress reactivity42 and was included to explore whether mindfulness skills are being enhanced by the MBP and, therefore, constitute a potential mechanism of change.19 Further definitions of mental health and well-being, as well as the assessment measures used, are included in online supplemental materials 1.
Supplemental material
Information sources and search strategy
Eight databases were searched (Ovid Embase, Ovid PsycINFO, Ovid MEDLINE, Scopus, ProQuest Theses & Dissertations, Cochrane CENTRAL, EBSCOHost SPORTDiscus and Google Scholar). The search strategies were developed with an information specialist (EH), and combined sets of terms for the thesaurus, title and abstract fields for mindfulness or meditation, athletes or para-athletes, along with filters for RCTs. No specific terms for comparators or outcomes were used. The search strategies for each database are available in online supplemental materials 2. Electronic searches were supplemented by forward/backward hand-searching the references of included primary papers and previous reviews.
Supplemental material
Study selection and data collection
The titles and abstracts of retrieved papers were screened independently by two authors (KM and PG), with disputes settled by the third (NK), using Covidence software.43 The full texts of relevant papers then underwent the same screening process. Standardised data collection forms were used to report the author and publication year, sample, sport(s), country, level of competition, mean age, MBP type, programme length (weeks), number of sessions, duration (of each session), dose (total duration of programme), control group, randomisation method, attrition, teacher experience, outcome measures, end point/follow-up, study and intervention quality, and researcher allegiance. Data were extracted by one author (KM) and independently verified by a second (NK). For information needed to calculate standardised effect sizes (ESs) not available in the article, a request to provide missing data was made to the author(s). Researcher allegiance was assessed against the following criteria: (1) mindfulness was the only therapy referenced in the title; (2) mindfulness was explicitly mentioned as the main experimental intervention in the introduction; (3) the control condition was included to control for the non-specific components of mindfulness; (4) there was an explicit hypothesis that mindfulness was expected to be more effective than the control.44 Quality of interventions was assessed using the following criteria: (1) a treatment manual was used; (2) the MBP was delivered by a qualified mindfulness teacher; (3) verification of treatment integrity occurred.44 45 The template for data collection is available in online supplemental material 3.
Supplemental material
Study risk of bias and certainty assessment
Study quality was evaluated using the Joanna Briggs Institute’s checklist for RCTs.46 This validated tool assesses the risk of bias within a study’s design, including randomisation method, allocation concealment, blinding, incomplete outcome data and reliability of measures. The full checklist is available in online supplemental material 4. The appraisal score was the number of ‘yes’ responses against the 13 applicable criteria. Cut-off points were based on those used in previous systematic reviews concerning athlete mental health47 and were ≤5=low quality, 6 or 7=moderate quality, ≥8=high quality, with two criteria that evaluated the blinding of assessors and those delivering the intervention deemed not applicable due to the nature of delivering and assessing psychological interventions.47
Supplemental material
The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) framework was used to define the certainty of the evidence for each individual outcome. Outcomes may be downgraded from ‘high’ to ‘moderate’, ‘low’ or ‘very low’ certainty of evidence due to risk of bias, publication bias, inconsistency, imprecision or indirectness.48 Two authors (KM and NK) independently assessed the evidence; in unclear cases, a decision was made by consensus. The template is available in online supplemental material 4.
Data synthesis
Analyses were conducted in R Studio V.1.3.1070 using the Metafor package.49 A random-effects model was used to account for differences in the intervention, control, sport and measures for the same outcomes. We used the standardised mean difference to estimate summary ESs. If more than one measure was used for a single variable in the same study, the mean was taken. For continuous outcomes, the mean post-test score of the MBP group was subtracted from the mean post-test score of the control group then divided by the pooled SD to yield Hedges’ g. ESs are considered small when g=0.20, moderate when g=0.50 and large when g≥0.80.50 The relative risk of dropout was calculated by dividing the cumulative incidence of intervention dropout by control dropout to measure the acceptability of MBPs in elite sport settings. Forest plots were used to visualise the ES from individual studies, depicted by squares whose size represented the relative weight given to the study based on sample size, accompanied by a 95% CI. The summary ES was represented by a diamond, with its horizontal spread indicating the 95% CI.
The four outcomes measuring mental health symptoms (anxiety, depression, psychological distress and stress) were combined to produce a single mental health outcome, and an accumulative ES was calculated to show the overall effect of MBPs on mental health symptoms.51 This combined outcome was used in the subgroup and meta-regression analyses.
Heterogeneity of studies was calculated using the Q statistic and Z-tests to produce an I 2 value and a 95% CI. I 2 acts as a descriptor of the percentage of variance in observed effects, based on variance due to true effects, using cut-offs: low, ≤25%; moderate, 25–75%; high, ≥75%.52 τ 2 was also used to represent the absolute value of true variance. A p value of <0.1 for the Q statistic indicated significant heterogeneity, and a τ 2 value of >1 indicated substantial between-study heterogeneity.53 Publication bias was assessed using the Duval and Tweedie trim and fill method to produce a funnel plot.54 Asymmetry in the funnel plot indicated potential publication bias, and an estimate of the number of missing studies recalculated the estimated ES based on the ‘filled-in’ studies. Begg and Mazumdar’s rank correlation, Eggers’s regression test for funnel plot asymmetry and Rosenthal’s fail-safe N, which estimates the amount of unpublished null studies required to nullify the results found, were also used to estimate publication bias.
Exploratory subgroup analysis was performed using a mixed-effect model,55 including the following variables: level of competition, MBP type, control type, researcher allegiance (1–2=low, 3–4=high), intervention quality (0–1=low, 2–3=high) and risk of bias (low=≤5, moderate=6 or 7). Other variables were not included due to incomplete data. Post hoc subgroup analysis can be used to generate hypotheses rather than make causal inferences.56 Metaregression was conducted using bivariate regression analysis, with the following variables: mean age, sex, MBP type, length, number of sessions, dose, risk of bias, control type, intervention quality, and researcher allegiance, first individually, then combining the significant variables using a multivariable approach. The statistical significance was set at a p value of <0.05 on both sides for all tests except for the bias-related tests, which were one-tailed.
Results
Study selection
After duplicates were removed, 2386 papers were screened for eligibility, resulting in 189 papers undergoing full-text screening. Twelve studies were included in the final qualitative synthesis and meta-analysis.57–68 See figure 1 for the PRISMA flow diagram.
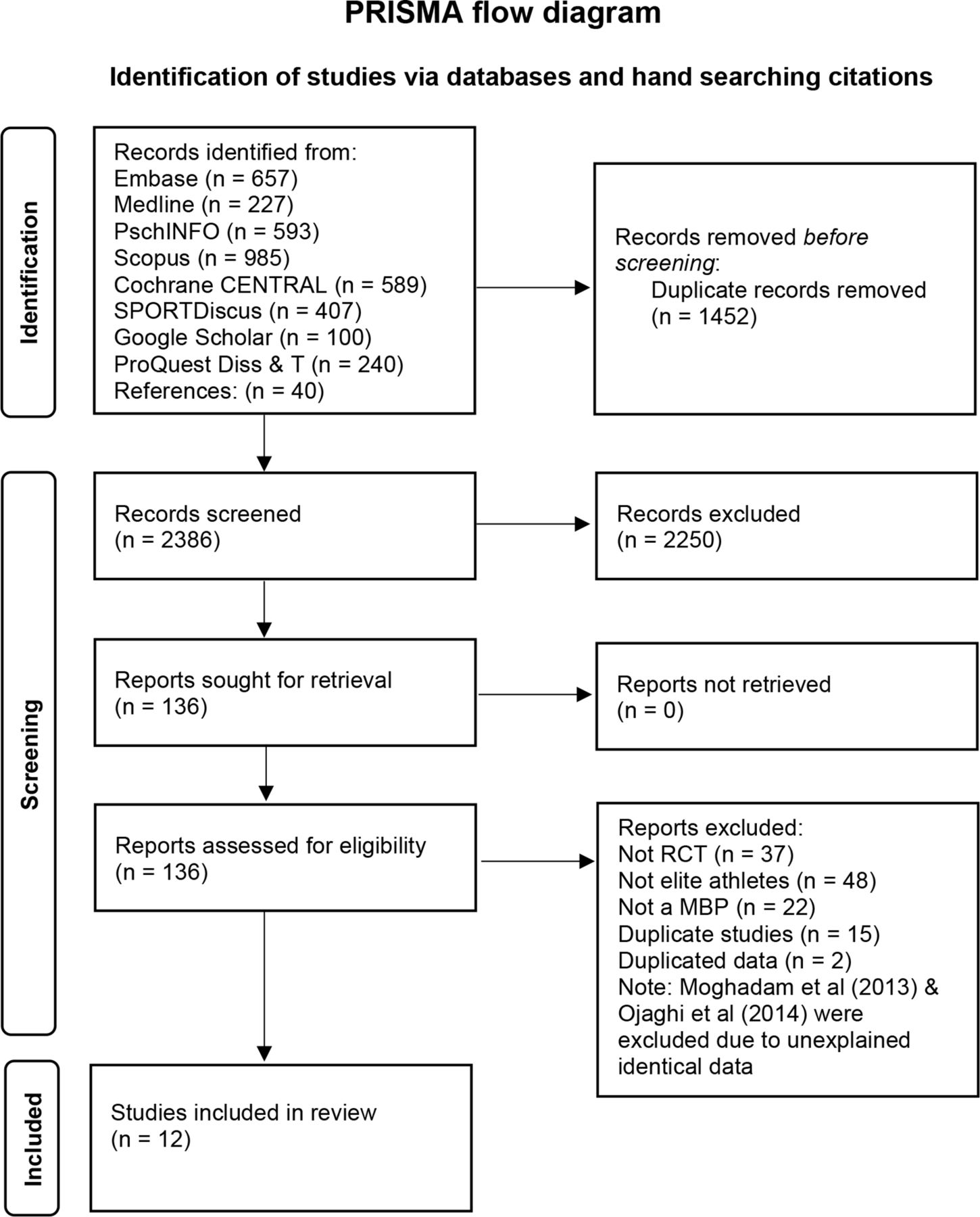
Preferred Reporting Items for Systematic Reviews and Meta-Analyses systematic review and meta-analysis flow chart. MBP, mindfulness-based programme; RCT, randomised controlled trial.
Description of included studies
Seven of the 12 studies were published in 2019 or later. The total number of athletes analysed was 613 (313 MBPs, 300 controls, mean 26 per condition), consisting of 457 (75%) men and 156 (25%) women. Seven studies focused on performance and well-being,58–60 62 64 67 68 two on anxiety/stress reduction,63 66 two on injury/concussion recovery61 65 and one on mindfulness/flow.57 The relative risk of dropout from the MBP was 0.48 compared with the control, with 4% (14/313) attrition from the MBP and 9% (28/300) from the controls. The mean age of athletes ranged from 17 years to 34 years. For further details, see table 1.
Description of individual studies
MBSR and the mindful acceptance commitment (MAC) approach69 were the most commonly used programmes, although five studies58 61 63 64 67 used considerable adaptations. Three studies used qualified mindfulness teachers59 62 64; three did not report who delivered the teaching58 63 67; three used PhD/MSc students61 65 68; one used sport psychologists60; another used a clinical psychologist66; and one used prerecorded audio.57 For further details, see online supplemental materials 3.
Risk of bias and certainty of evidence
The overall methodological quality of the 12 studies, according to the Joanna Briggs Institute’s checklist for RCTs,46 was moderate, with 10 studies rated moderate and two rated low. Full details are in online supplemental material 4. According to the predetermined criteria detailed in the methods,44 the quality of the interventions was generally moderate, with a mean of 1.8 out of 3. All 12 studies showed a degree of researcher allegiance towards MBPs, with a mean score of 3.4 out of 4. For further details, see table 1.
According to the GRADE framework,48 the stress and psychological distress outcomes were rated as having a high certainty of evidence. The anxiety and psychological well-being outcomes were downgraded to moderate due to inconsistency of results and imprecision. The depression and mindfulness outcomes were downgraded to moderate because of a strong suspicion of publication bias. For further details, see online supplemental material 4.
Results of individual studies and meta-analysis
Four outcomes assessing symptoms of anxiety, depression, psychological distress and stress were combined to represent the overall effect of MBPs on mental health symptoms and disorders. A significant moderate–large ES in favour of MBPs improving overall mental health was found (g=−0.75, number of studies (k)=9, p<0.001, 95% CI −1.06 to −0.45 (I 2=81, p<0.001, 95% CI 78 to 94, τ 2=0.33)).
Symptoms of anxiety
Six studies measured anxiety among 409 male and female athletes from different sports (mean age range: 17.1 to 34.1 years). Four studies included general symptoms of anxiety,59 66 67 70 and two studies considered competition specific anxiety.63 65 Overall, there was a significant large ES for MBPs reducing anxiety (g=−0.87, k=6, p=0.017, 95% CI −0.16 to −1.59; see figure 2). High heterogeneity was estimated between the studies (I 2=90, p<0.001, 95% CI 81 to 99, τ 2=0.68). From the two studies that measured competition anxiety, a large significant ES was found in favour of MBPs reducing symptoms (g=−0.85, k=2, p=0.018, 95% CI −0.15 to −1.55 (I 2=61, p≤0.001, 95% CI 0 to 100, τ 2=0.17)).

Forest plots showing the SMD for anxiety, depression, psychological distress, stress, psychological well-being and mindfulness between athletes who participated in an MBP compared to controls. CI, confidence interval; DF, degrees of freedom; MBP, mindfulness-based programme; p, significance of heterogeniety; Q, Cochran’s Q test; SM, standardised mean difference.
Symptoms of depression
Three studies measured depression among 166 male and female athletes from different sports (mean age range: 19.8–34.1 years).59 66 67 A large but non-significant ES (g=−0.90, k=3, p=0.13, 95% CI −2.05 to 0.25) was associated with MBPs reducing depression (see figure 2). High heterogeneity was likely (I 2=90, p<0.001, 95% CI 56 to 100, τ 2=1.49).
Psychological distress
Four studies measured psychological distress among 335 male and female athletes from different sports (mean age range: 17.1–32.5 years).58 62 65 67 A significant moderate ES (g=−40, k=4, p<0.001, 95% CI −0.61 to −0.18) was associated with reduced psychological distress in favour of the MBP (see figure 2). Heterogeneity between studies was estimated to be low (I 2=0, p=0.820, 95% CI 0 to 93, τ 2=0).
Stress
Five studies measured stress among 153 male and female athletes from different sports (mean age range: 18.5–34.1 years). Four used self-report measures,59 61 64 66 and one used salivary α-amylase, a commonly used biomarker of stress.63 A large significant ES (g=−0.91, k=5, p=0.012, 95% CI −0.20 to −1.61) was associated with MBPs reducing stress (see figure 2). Moderate heterogeneity was estimated between studies (I 2=74, p<0.001, 95% CI 0 to 93, τ 2=0.47). Removing the physiological measure produced a similar ES (g=−0.89, k=4, p=0.051, 95% CI −1.78 to −0.01 (I 2=80, p=0.002, 95% CI 31 to 98, τ 2=0.60)), with significance approximated to the alpha level.
Psychological well-being
Five studies measured psychological well-being among 237 male and female athletes from different sports (mean age range: 19.8 to 34.1 years).59 62 66–68 A large significant ES (g=0.96, k=5, p=0.039, 95% CI 0.05 to 1.86) was associated with MBPs increasing psychological well-being (see figure 2). High heterogeneity was estimated (I 2=89%, p<0.001, 95% CI 72 to 99, τ 2=0.93). Removing a potential outlier66 resulted in a non-significant moderate ES in favour of MBPs (g=0.49, k=4, p=0.084, 95% CI −0.06 to 1.04)
Mindfulness
Ten studies measured mindfulness among 458 male and female athletes from different sports (mean age range: 17.1–32.5 years).57–65 We observed a significant moderate increase in mindfulness in the MBP group (g=0.62, k=10, p=0.003, 95% CI 0.22 to 1.03; see figure 2). Heterogeneity between studies was likely to be moderate (I 2=73, p<0.001, 95% CI 29 to 92, τ 2=0.28).
Publication bias
On inspection of the funnel plots, publication bias was not suspected for anxiety, psychological well-being and stress. Missing studies were filled in for depression, psychological distress and mindfulness, highlighting potential publication bias as shown in figure 3. Using the trim-and-fill method, we estimated two studies to be missing for depression, revising the estimated ES to g=−0.02 (95% CI −1.14 to 1.10) and one study each for psychological distress ( g =−0.38, 95% CI −0.59 to −0.17) and mindfulness (g=0.53, 95% CI 0.13 to 0.93). Begg and Mazumdar’s rank correlation was not significant for depression (T=−0.33, p=1), psychological distress (T=−0.33, p=0.751) or mindfulness (T=−0.06, p=0.920). Eggers’s regression was not significant for depression (Z=0.9, p=0.358), psychological distress (Z=0.24, p=0.811) or mindfulness (Z=0.81, p=0.418). The fail-safe N for depression was 1, that for psychological distress was 4; and that for mindfulness was 6, indicating the number of unpublished null studies that would be required to nullify the results of these outcomes.

{kind=link}
{kind=link}
{kind=link}
Duval and Tweedie’s trim-and-fill funnel plots for each outcome. Solid circles represent the studies included in the meta-analysis, and hollow circles indicate 'filled-in' studies based on suspected publication bias.
Subgroup analysis
Exploratory subgroup analysis was conducted using the overall mental health outcome ES. As shown in table 2, differences in the level of competition suggested that MBPs may be more effective in senior and retired athletes compared with junior and para-athletes. MAC was indicated to be the most effective MBP, with no differences between the other variations. Studies that scored high for intervention quality had larger ES, as did studies with high researcher allegiance and those with a non-active control group.
Subgroup and metaregression analyses on the overall effects of potentially moderating variables
Metaregression
Using the overall mental health ES, four variables (age, MBP type, researcher allegiance and control type) significantly predicted ES in the univariate analysis. Age was substituted for level of competition due to considerable co-linearity. Multivariable analysis found that age predicted an increase in ES magnitude of 0.08 for each additional year (β=−0.08, p=0.012). High researcher allegiance (β=−0.55, p≤0.010) and studies without an active control (β=−0.91, p=0.021) each predicted an increase in ES magnitude. MAC appeared to be the most effective programme overall (β=−0.29, p≤0.001). The total variance explained by the model was 64% (R 2=0.642, p=0.002). For further details, see table 2.
Discussion
Summary of findings
This review reports on the effects that MBPs had on elite athlete mental health. The primary results suggest that overall, MBPs improve mental health-related outcomes. Significant large ESs were found for reduced anxiety and stress and increased psychological well-being, and moderate ESs for reduced psychological distress and improved mindfulness. Large but non-significant ESs were found for reduced depression. While these results are encouraging and lend weight to the potential benefits that MBPs offer to elite athletes, the outcomes were subject to high heterogeneity or suspected publication bias. Therefore, the evidence can be framed as promising and provisional.
Interpretation and comparison with previous research
Previous reviews of MBPs in sport have reported reduced stress,71 burnout72 and improvements in performance in mixed-level athletes23 73 74 and have criticised the quality of evidence from studies with low methodological rigour.71–73 This systematic review and meta-analysis of MBPs is the first that (1) concentrated exclusively on elite athletes, (2) evaluated RCTs only and (3) focused only on mental health outcomes. This review, therefore, offers considerable potential to meaningfully inform clinical practice and future research.
Elite athletes are exposed to cultural, environmental and personal stressors that can increase the risk of experiencing mental health symptoms and disorders.5 75 These stressors may be compounded by stigma and low help-seeking behaviour,47 but athletes have been shown to better engage with interventions that are designed to fit the sporting culture and support performance.76 77 We observed a lower relative risk of dropout reported in the mindfulness group compared with the controls, suggesting MBPs are an acceptable form of mental health intervention for elite sport settings. This is supported by reductions in competition anxiety as well as general anxiety, highlighting the potential of MBPs to positively influence performance alongside mental health.78 Exploratory subgroup analysis suggested that age may be a moderator for the effectiveness of MBPs, with larger ESs found in trials with a higher mean age. MBPs also appeared to be particularly effective for retired athletes, which in part accounted for the finding that older athletes may benefit more from MBPs. Further research investigating the effectiveness of MBPs at different stages of the athletic career is required.
A notable result from this review is the non-significant ES for depression. Only three studies measured depression. Two reported large significant ESs for MBPs reducing symptoms of depression,59 66 and one reported a negligibly small ES.67 Interestingly, all three studies used MBSR. The two studies that reported large significant results followed the recommended MBSR protocol more closely, with eight sessions of 75–90 min, whereas the study that reported small, non-significant results employed a substantially reduced protocol, consisting of four sessions of 45 min. It may be that losing fundamental components of the programme reduced its effectiveness, as core elements of an MBPs curriculum should be maintained.20 High-fidelity MBPs are effective in treating symptoms of depression in the general population and in clinical samples.16 17 More research is required to determine whether low-fidelity adaptations of MBSR or MBCT and programmes such as MAC are effective in reducing symptoms of depression in elite athletes. In general, MBPs teach foundational skills that support mental health and well-being across the spectrum, from those experiencing clinical disorders to those who are free of mental health symptoms and are flourishing.8 18 19 The group-based delivery format of MBPs means they can be offered widely to elite athletes and may, therefore, bypass some of the stigma associated with interventions focused on treating mental health disorders. Furthermore, as a group-based programme, they are potentially more accessible and scalable.79 Universal prevention strategies for physical injuries are commonplace in elite sport.80 81 In the same way, MBPs have potential as a psychological intervention to treat and prevent mental health symptoms while also supporting performance.23
Successful implementation of MBPs requires careful consideration of the social context, which is particularly important in elite sport settings.82 Peer influence and coach endorsement have considerable influence in an environment where displays of vulnerability are often discouraged.83 It is unclear whether the prevalence of mental health symptoms differs between athletes who compete individually or in a team,47 84 but athletes involved in individual sports may engage more positively with psychological interventions.85 Regardless, all elite athletes operate within a team of support staff. MBPs for elite coaches have been shown to reduce stress and burnout,86 87 so it is possible that MBPs could have indirect positive effects on athletes’ mental health through an improved social climate, cultivated by coaches who model skills that support mental health.25 83
Trials of MBPs in clinical settings typically prioritise internal validity by ensuring fidelity in terms of the curricula and teachers.88 The ability of the teacher is necessary to facilitate learning new skills and group discussions, ensure skills are practised and applied in everyday life, and reduce the potential for harm.20 A variety of teaching methods were employed across the included studies, but incomplete reporting meant it can only be postulated, based on previous research, that this variable affected outcomes.13 32 89 Controlling the quality of teaching more carefully in future research may reduce the variability of results and allow clearer recommendations to be made.
Limitations
This review is subject to several limitations. The overall sample was weighted towards male athletes (75%) and contained only 3% para-athletes, so the results may not be generalisable to all elite athletes. Data were generally unavailable for ethnicity, gender identity, sexuality, socioeconomic status and other variables that may have been useful for determining how effective MBPs were for subpopulations of elite athletes. A relatively small number of RCTs and generally small sample sizes within these studies, plus inconsistent follow-up data, are further limitations of the included studies and, therefore, this review. The systematic appraisal of study quality suggested that the overall risk of bias was moderate, but significant heterogeneity between studies was present. Potential sources of heterogeneity were the different measures used to evaluate mental health outcomes, variations in the MBPs used and the comparison conditions. Mental health symptoms and disorders are broad in scope, with various definitions and methods of assessing and measuring outcomes. The data used in the analysis were primarily self-reported, with no data available from clinical assessments; therefore, the results were dependent on the individual’s own perception of symptoms, as well as potentially being subject to bias.90 Considering the broad scope of possible mental health outcomes and the complexities of MBPs, researcher judgement and simplification were necessary in this regard, as is common in quantitative syntheses of complex interventions.91 Variations between interventions and the methods with which they are taught are known to influence outcomes, and many of these variables were not evaluated.82 92 It was not possible to analyse individual data, to assess individual moderators or to identify the effects MBPs had on clinical versus versus subclinical symptoms of mental health disorders. Additionally, it was not possible to determine if low-fidelity MBP adaptations and programmes such as MAC were effective in reducing depression. Depression was not measured as an outcome in the five RCTs that used MAC. Furthermore, the subgroup and metaregression analysis was conducted post hoc, with a small number of studies/participants in some subgroups and thus underpowered in statistical terms for some comparisons, meaning the results from the analysis are exploratory and suitable for hypothesis forming but not making casual inferences.56 These limitations highlight the need to continue developing this field of research with higher-quality studies and adequate follow-up to evaluate the durability of results.
Implications for practice and future research
To increase the effectiveness of MBPs in practice, high-fidelity programmes such as MBSR or MBCT should be adapted to suit the social setting and incorporate elements of practice relevant to the sport, while retaining core components of the curriculum. Collaboration with key individuals such as coaches and senior team members to endorse the MBP is likely to improve acceptability,83 and importantly, teaching should be delivered by a qualified mindfulness teacher.13 24 32
Future research investigating the effect of MBPs on clinically relevant symptoms of mental health disorders, for example, depression, would help further guide practice. Research that investigates the cost-effectiveness and scalability of MBPs in elite sport settings, and research building on the single study that investigated how MBPs can support retiring athletes during their transition from elite sport would also be welcome.93 Once effectiveness is established, a further phase of research could investigate what works for whom, with attention paid to the diversity of participants, collection of data on ethnicity, gender, sexuality94 and common personality characteristics of elite athletes, for example, perfectionism, which may be functional in an elite sport context but considered maladaptive in general life.38 95
As a final note, mindfulness is not proposed as a solution to issues that exist within sport such as racism,96 97 sexual harassment, discrimination or bullying.75 98 Rather, it aims to teach foundational skills that help those in sport manage their thoughts, feelings and behaviour, alongside the need to address systemic problems within elite sport.99
Conclusion
MBPs have been shown to improve several mental health outcomes in elite athletes. Significant benefits to mental health can be derived from engaging in sustained mindfulness practice through a variety of methods, ranging from intensive in-person programmes to remote guidance via a recording. The potential to reduce both general symptoms of anxiety and competition-specific anxiety highlights the value of MBPs to support performance alongside improving mental health. Future research should concentrate on using high-quality MBPs that are adapted for elite sport settings and implemented with careful consideration of the requirements each unique environment has. Mindfulness is essentially a skill that is first learnt, then regularly practised, so the benefits accrue accumulatively over time. If MBPs are to gain credibility as an empirically validated method of improving the mental health of elite athletes, a shift away from uncoordinated informal practice towards high-quality, systematically implemented programmes, followed by consistent individual practice is required.
Key messages
What is already known?
Mindfulness-based programmes (MBPs) are comparable to other interventions to treat mental health symptoms and disorders in the general population.
MBPs are associated with improvements in athletic performance.
Athlete engagement with psychological interventions to improve mental health might be greater with interventions that also support performance.
What are the new findings?
This is the first systematic review and meta-analysis of MBPs that focused on mental health outcomes exclusively in elite athletes, evaluating evidence from randomised controlled trials only.
MBPs are an acceptable form of intervention in elite sport settings and show promise in improving several mental health outcomes including stress, anxiety and psychological well-being.
Adapted MBPs that teach mindfulness in a sport-specific manner may be more effective for treating mental health symptoms in elite athletes.
MBPs may facilitate performance alongside mental health.
How might this study impact clinical practice in the future?
MBPs should be adapted to the sporting and social context.
Core elements of a high-fidelity MBP should be retained, particularly when targeting specific mental health symptoms or disorders.
Framing the MBP as performance support may decrease the stigma associated with help seeking for mental health symptoms and increase engagement with the programme.
MBPs may reduce symptoms of anxiety and competition anxiety, highlighting the value of MBPs to support performance alongside mental health.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @kearnanmyall
Contributors All authors have made substantial contributions to planning, conducting, reporting and critical revision. KM is responsible for the overall content as guarantor.
Funding This work was supported by the Wellcome Trust (grant reference numbers 104908/Z/14/Z and WT104908MA) and the Rugby Players Association. JM-M has a Miguel Servet research contract from the ISCIII (CP21/00080).
Competing interests KM and NK are PhD researchers at the Oxford Mindfulness Centre. JM-M is associated with the Oxford Mindfulness Centre. WK is the director of the Oxford Mindfulness Centre.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.