Article Text

Abstract
Objective A multifactorial combination of predictors may increase anterior cruciate ligament (ACL) injury risk in athletes. The objective of this twin study was to examine these risk factors to identify commonalities in risk factors that predisposed female fraternal twins to ACL injury.
Methods Female twins in high-risk sports were prospectively measured prior to an injury for neuromuscular control using three-dimensional motion analysis during landing, hamstrings and quadriceps muscular strength on a dynamometer and joint laxity using a modified Beighton–Horan index and a Compu-KT arthrometer. Intraoperative measures of femoral intercondylar notch width were recorded during ACL reconstruction.
Results Abduction angles were increased at one knee in both of the twin sister athletes relative to uninjured controls at initial contact and at maximum displacement during landing. The twin female athletes that went on to ACL injury also demonstrated decreased peak knee flexion motion at both knees than uninjured females during landing. The twin athletes also had increased joint laxity and decreased hamstrings to quadriceps (H/Q) torque ratios compared to controls. Femoral intercondylar notch widths were also below the control mean in the twin siblings.
Conclusions Prescreened mature female twins that subsequently experienced ACL injury demonstrated multiple potential risk factors including: increased knee abduction angles, decreased knee flexion angles, increased general joint laxity, decreased H/Q ratios and femoral intercondylar notch width.
Statistics from Altmetric.com
Anterior cruciate ligament (ACL) rupture is a severe ligamentous knee injury, leading to functional instability in the short term and to degenerative joint disease in the long term. Although ACL reconstructive procedures are available, they are costly and may have high morbidity. Between 100 000 and 250 000 ACL reconstructions are performed each year at a cost of US$17 000 to US$25 000 per procedure.8 12 Hence, the direct medical cost for reconstructive surgeries alone are over a billion US dollars per year. This figure does not include the initial costs of conservative treatment and rehabilitation of those injuries that are not repaired.13
The high physical, mental, emotional and economic costs of ACL injury have prompted analyses of predictive risk factors for this devastating injury.11 15 Anderson et al did not observe a difference in the prevalence of ACL injuries among family members of ACL injured and non-injured subjects.2 However, two case-control studies have reported familial history as a factor related to increased risk of ACL injury.5 20 Athletes that experience an ACL tear may be more likely to have a relative with an ACL tear compared with controls matched for age, sex and sport.5 First, Lambert et al, and more recently Flynn et al, reported a familial predisposition for ACL rupture. A third study, that of Harner et al, reported an increased prevalence of ACL rupture among family members of ACL injured subjects compared to controls. They reported that 11 of 31 patients (35%) with ACL injury had a family history of ACL tear.9 In comparison, only 1 subject out of 23 (4%) from the uninjured control group had a family history of ACL injury.9 Flynn et al reported that subjects with a history of ACL injury were twice as likely to have a first-degree relative with a history of ACL injury as a matched control group without a history of ACL injury.5 Similar, Lambert et al reported a higher prevalence of family members with a history of ACL rupture among ACL injured subjects.
Potential risk factors for an ACL injury can be classified as intrinsic (within the body) or extrinsic (outside the body).11 15 Specific intrinsic factors that have been investigated include anthropometric, biomechanical, neuromuscular, anatomic, developmental and hormonal, genetic, ligament integrity, activity level and prior injury. For example, knee abduction torque and motion during landing is a potentially strong predictor of ACL injury risk in female athletes.16 Hewett et al reported that external knee abduction torque at the knee predicted ACL injury risk with 78% sensitivity and 73% specificity in young female athletes.16
Comparison of twin siblings may provide initial delineation of genetic traits and predisposition to disease or injury. In general, neuromuscular control, osseous anatomy, ligament integrity and body type or body mass index (BMI) theories have all been proposed as potential factors or contributors in the increased risk of ACL injury.11 15 Specifically, knee abduction (valgus), knee laxity, increased quadriceps strength and relative hamstrings to quadriceps strength ratios, and intercondylar notch width have all been reported to be associated with increased risk of ACL injury in female athletes.11 15 19 23 29 However, the genetic underpinnings of these potentially important risk factors remain unreported. The potential for genetic transmittal of the biomechanics of high-risk sports movements and of neuromuscular control of these movements remains an intriguing, but unstudied phenomenon.
Bony anatomic and ligamentous integrity traits, on the contrary to biomechanics of movement and neuromuscular control, are more understandable and testable potentially genetic characteristics. For example, femoral intercondylar notch width may be an inheritable trait that may predict ACL injury risk in women.34 36 Knee laxity (hyperextension) may also be predictive of increased ACL injury risk.29 32 Women, on average, may have narrower femoral intercondylar notch widths than men, which may be indicative of either notch impingement on the ACL or lead to a smaller ACL within the narrower intercondylar notches.34 Athletes with stenosis of the intercondylar notch have been reported to be significantly more likely to injure the ACL during a non-contact sports injury.36 Other reports have found no sex difference in intercondylar notch width, but these studies used the notch width index as a measure.1 4 21 The notch width index is a ratio of intercondylar notch width divided by the femoral condyle width but may not give an accurate indication of actual ACL size, especially when normalised to body/femur size.21
The objective of this study was to compare risk factors that may have predisposed two female twins and their older sister to subsequent ACL injuries playing soccer and basketball. This study examined the concept that injury risk is increased among athletes with ACL injured first-degree family members. The first theory examined was that female sibling athletes would demonstrate biomechanical differences, such as greater knee abduction and decreased knee flexion, than uninjured athletes during landing (table 1). A second theory examined was that female sibling athletes would demonstrate different neuromuscular strength measures than the mean female athlete values. The third theory examined was that these twins would demonstrate increased generalised ligamentous and knee laxity measures than the average uninjured female athlete. The final theory examined was that female sibling athletes would demonstrate narrower intercondylar notch widths than the average woman.
Multifactorial assessment approach for potential future anterior cruciate ligament (ACL) injury risk
Methods
Subjects
Two fraternal twin sibling female high school soccer and basketball players volunteered to participate in a large cohort study of soccer and basketball athletes. Parents and participants read and signed the informed consent and assent, respectively. Height and mass were measured and leg dominance was determined by which leg the athlete stated that they would use to kick a ball the greatest distance.
Procedures
Laxity assessment
Generalised joint laxity tests consisted of: fifth-finger hyperextension greater than 90°, elbow hyperextension greater than 0°, wrist and thumb to forearm opposition, knee hyperextension greater than 0°.29 31 Anterior–posterior tibiofemoral translation was quantified using the Compu-KT knee arthrometer (Medmetric, San Diego, California, USA) to measure total anterior–posterior displacement of the tibia relative to the secured femur. During the measurement, each leg was placed on the adjustable thigh support with knee stabilised at 20° to 35° of knee flexion. The arthrometer was secured to the shank such that the patellar sensor pad was rested on the patella with the knee joint line reference mark on the Compu-KT aligned with the subject's joint line. The ankle and foot were stabilised to limit leg rotation. The tester provided a posterior and anterior (±134 N) pressure on an axis perpendicular to the tibia. Total displacement (mm) was plotted on the computer and recorded.29 Hamstring flexibility was measured at the time of neuromuscular and biomechanical testing by knee angle (degrees from full extension, with full extension designated as 0° and knee flexion angles greater than 0° designated as negative) and the hip at 90 degrees flexion using a goniometer as per the method of Knapik et al.19
Maximal jump height
A maximum vertical height was determined using a MX-1 vertical jump trainer (MXP Sports, Reading, Pennsylvania, USA) with a basketball as a target to encourage maximum jump height.7 The athlete was instructed to grab the ball with both hands as they jump as high as possible. The height of the ball was adjusted until the athlete failed to grab the ball in three consecutive trials. The greatest vertical jump height was recorded.7 This target height was then set for all drop vertical jump trials.
Three-dimensional biomechanical analysis of drop vertical jump testing
Each subject was instrumented with 19 retroreflective markers placed bilaterally on the greater trochanter, mid-thigh, medial and lateral knee (joint line), mid-shank, medial and lateral ankle (malleolus), posteriorly on the calcaneous and superiorly on the dorsal aspect of the foot (between second and third metatarsals). An additional marker on the left posterior superior iliac spine was also applied to offset the right and left side to aid the real-time identification of markers during data collection (fig 1). The motion analysis system consisted of eight digital cameras (Eagle cameras, Motion Analysis, Santa Rosa, California, USA) connected through an Ethernet hub to the data collection computer (Dell, Round Rock, Texas, USA) and sampled at 240 Hz. Two force platforms (Advanced Mechanical Technology, Watertown, Massachusetts, USA) were sampled at 1200 Hz and time was synchronised to the motion analysis system.

Locations of reflective markers during data collection. Medial knee and ankle markers (white) were removed after collection of the static trial. Sacrum, left posterior superior iliac spine, left mid-tibia and right heel markers are not visible in this view.
A static trial was collected with the subjects standing as positioned in fig 1. Kinematic measures were in relation to the static position. Each athlete was shown the drop vertical jump (DVJ) manoeuvre and was given adequate practice to be able to successfully complete the task (fig 2). The drop vertical jump consisted of dropping off the box and jumping immediately to grab the target.6 Three drop vertical jumps were performed from a box height of 31 cm (fig 2). The data were collected with EVaRT software (V. 4, Motion Analysis). The motion analysis system was calibrated to recommended specification prior to each data collection session.

Reflective marker locations collected simultaneously with two force platforms. Skeletal segments created using external marker locations. Drop vertical jump task and accompanying body models are shown.
Three-dimensional marker trajectories were calculated in EVaRT and exported to MATLAB (version 7.5, The Mathworks, Natick, Massachusetts, USA) for analysis. Marker trajectories were smoothed with a low pass Butterworth filter at a cut-off frequency of 12 Hz. Knee joint flexion–extension and abduction–adduction cardan angles were calculated within MATLAB with modified versions from the KineMat Toolbox.33
Notch width measurement
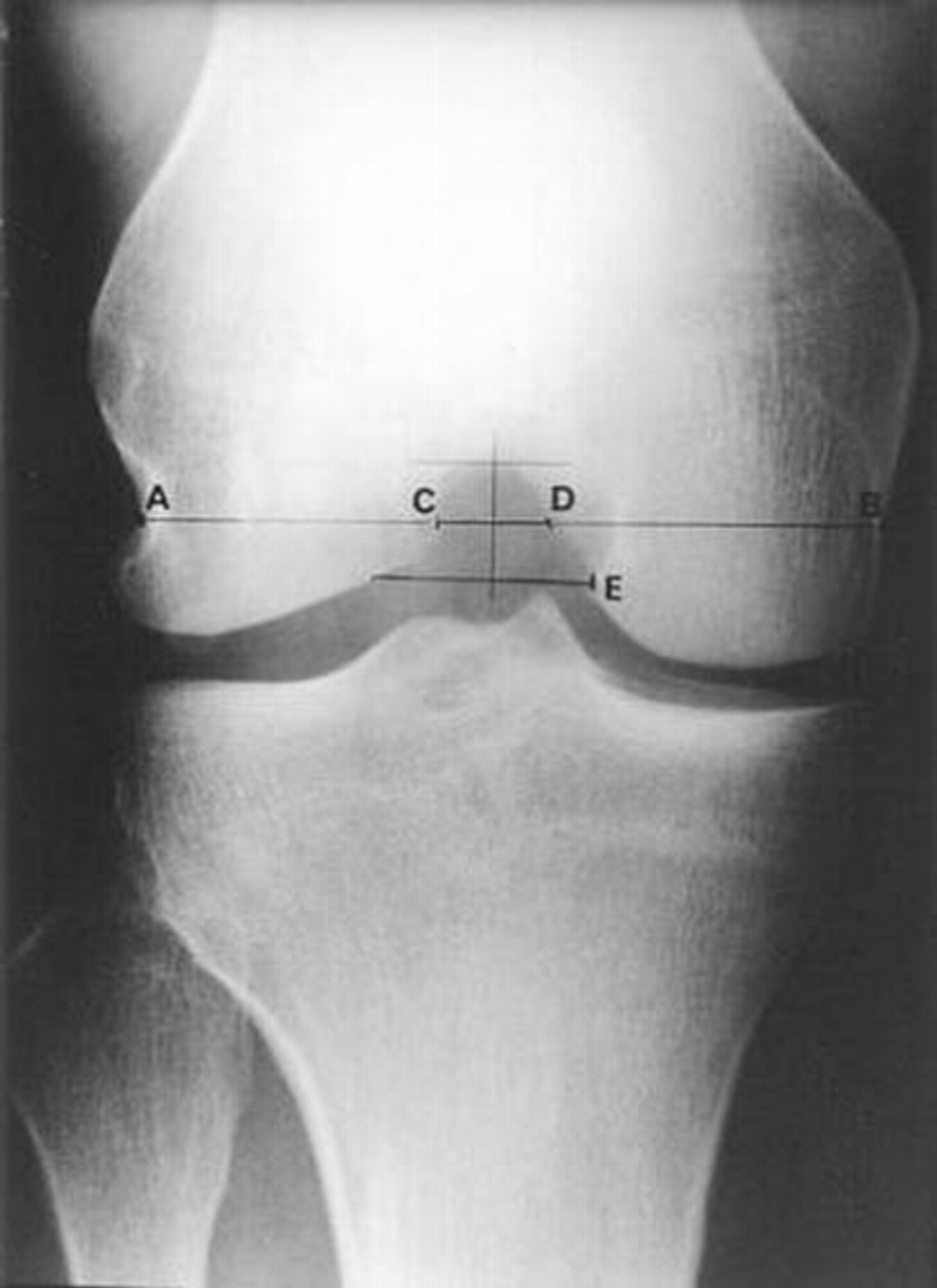
Notch width was measured intraoperatively and arthroscopically per the method of Shelbourne and Kerr.35 Measurements included femoral condylar width, femoral notch width and the widest point of notch opening. (fig 3)

Notch width measure as per Shelboune and Kerr.35 A to B is a measure of femoral condylar width, C to D is a measure of femoral notch width and E represents the widest point of notch opening.
Clinical findings and results
Injury details and anthropometric measures
Sibling 1 ruptured the ACL of her non-dominant left knee, whereas sibling 2 ruptured the ACL of her dominant right knee. Video images were obtained of the left ACL injury of sibling 1 (fig 4). Sibling 2 reported a prior knee injury, torn cartilage, at the time of testing. Sibling 1 reported prior ankle injury, but no prior knee injury, at the time of testing. The twins had a family history of ACL Injury, as their older sister experienced an ACL rupture previous to their injuries. Both of these twin siblings were physically and developmentally mature, at the time of testing. They reported beginning regular menstrual periods at ages 12 and 13, respectively. Their data were compared to 72 school-sponsored soccer and basketball players, who were teammates of the twin siblings. Age, height, mass and BMI for each twin sibling were similar to each other and to control values for the 72 non-injured female soccer and subjects (table 2, anthropometric data).

Injury sequence of sibling 1. See also supplementary material.
Characteristics for siblings 1 and 2 and controls
Biomechanical measures
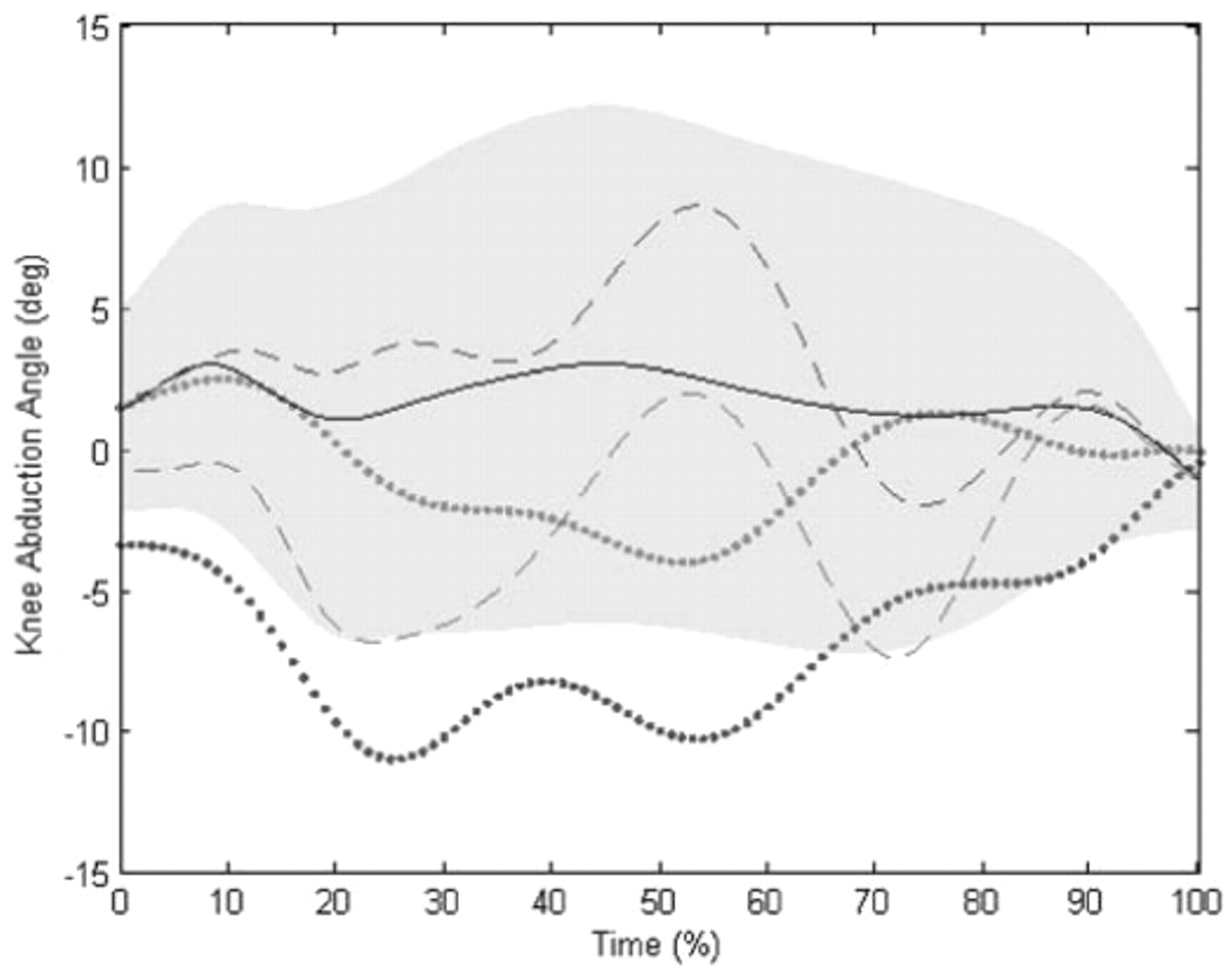
Table 3 and figs 5 and 6 show measured knee kinematic variables in the frontal and sagittal planes in the twin siblings and the means (SDs) of a large (72 female athletes) control cohort. The biomechanical assessment of landing demonstrated that peak knee abduction motion was increased compared to uninjured controls in one knee of both of these twin siblings (fig 5 and table 3). Knee abduction range of motion was observed to be higher than uninjured controls (fig 5 and table 3).
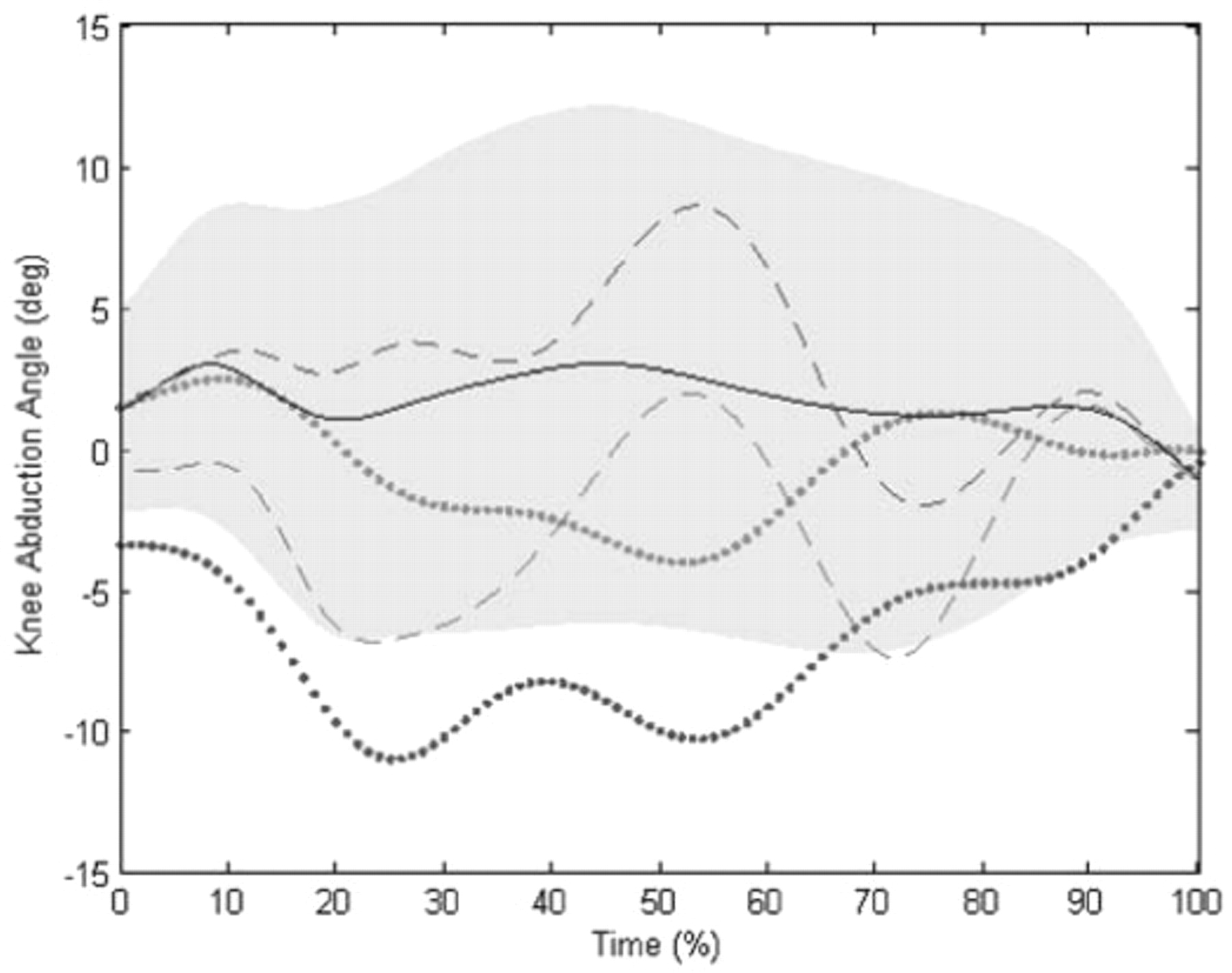
Knee abduction angle during stance phase of the drop vertical jump (DVJ). The dotted line is sibling 1 (S1) and the dashed line is sibling 2 (S2). The red line is the injured side and the blue line is uninjured side. The solid black line and grey shading represent population mean ±1 SD.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Knee flexion angle during stance phase of the drop vertical jump (DVJ). The dotted line is sibling 1 (S1) and the dashed line is sibling 2 (S2). The red line is the injured side and the blue line the uninjured side. The solid black line and grey shading represent population mean ±1 SD.
Knee flexion and abduction kinematics during landing from a drop vertical jump (DVJ) manoeuvre
Kinematic variables at the knee in the sagittal plane were observed to be different than controls at peak motion (table 3 and fig 6). The twin female athletes demonstrated decreased maximum knee flexion motion compared with the uninjured athletes. The sibling athletes demonstrated lesser peak knee flexion than other athletes. Hence, differences in knee motion were also observed in the sagittal plane. These female athletes demonstrated lesser knee flexion range of motion than uninjured athletes. In addition, fig 6 illustrates that sibling 1 demonstrated lesser peak knee flexion than uninjured athletes. However, sibling 2 did not. Hence, differences in knee motion were observed in the coronal and sagittal planes.
Neuromuscular: strength and power
The neuromuscular findings of the twin siblings followed trends similar to the neuromuscular variables of control subjects. Table 4 shows the neuromuscular variables in the sagittal plane. The hamstrings/quadriceps ratio peak torque values are shown in table 4. Sibling 1 showed decreased hamstrings to quadriceps peak torque ratios compared to controls and large side to side differences in these relative peak torques. In addition, maximal vertical jump was evaluated as a performance measure of whole body power. The twin athletes demonstrated vertical jumps that were in the control range of female athletes of similar age and sport (table 4).
Neuromuscular factors
Joint and ligament laxity and hamstring flexibility
Generalised joint laxity measurements were similar between the sibling female athletes and greater than the controls (table 5). In addition, sibling 1 had hamstring flexibility that was similar to injured subjects, while sibling 2 had greater hamstring flexibility (−5) on her later injured right dominant side that was more than 1 SD greater than the control mean (table 5). Arthrometermeasured ligament laxity at the knee in the sagittal plane was similar between twins and controls.
Joint and ligament integrity measures: general joint laxity indications and anterior–posterior knee laxity measures measured with a knee arthrometer of twins compared with large cohort of uninjured women
Notch width
Notch width was observed to be relatively low for these twin siblings relative to comparable control values from the literature (table 2).35 Femoral intercondylar notch widths were 12 and 13 mm, respectively, approximately 1 SD below the mean in the twins relative to uninjured, weight-matched women.35 Published data in the literature fromthe same doctor thatmeasured thenotchwidthof thesiblings (KDS) reportedamean(SD)notchof 15 (2.7) mm in a similar weight-matched (61 to 75 kg) athletic population. Hence, twin siblings 1 and 2 had intercondylar notch widths 3 to 2 mm lower than controls, respectively, with sibling 1 greater than 1 SD lower than the mean.35
Discussion
The theoretical basis of this sibling study was to determine if there are specific potential risk factors that underlie a familial tendency toward ACL rupture.1 The purpose of this twin sibling study was to identify potential factors, including anthropometrics, injury history, biomechanics of high-risk movement, neuromuscular performance measures, ligament integrity and notch width in twin sibling athletes with ACL injuries would differ from a large control population of similar athletes. A corollary objective was to spur further investigation into these important areas of research. Limited studies have addressed the familial tendency toward ACL rupture, with varying results. Anderson et al found no greater prevalence of ACL injuries among family members or ethnic groups.1 While Lambert et al, Harner at al, and more recently Flynn et al, concluded that there was a familial predisposition toward rupture of the ACL.5 20 In addition, in a recent 4-year cohort study, it was found that white European American athletes were 6.6 times more likely to experience an ACL tear compared with other ethnic groups, which was indicative of genetic underpinnings for ACL injury risk.
The first theory examined was that female sibling players would demonstrate differences in knee abduction and knee flexion measures compared to control athletes during a vertical drop manoeuvre. Increased knee abduction angles, knee abduction angular range of motion and decreased knee flexion were observed in the twin female siblings relative to a large control cohort from the same sports teams. In addition, side to side differences in knee abduction motion were observed. These differences have been reported to be significant predictors of future injury risk.16 A second theory examined was that female sibling athletes would demonstrate different neuromuscular strength measures than the mean female athlete values. This was observed in one of the twin athletes. Low hamstrings to quadriceps peak torque values were observed in sibling 1. The third theory examined was that these twins would demonstrate increased generalised ligamentous and knee laxity measures than the average uninjured female athlete. Increased generalised joint laxity was observed in both siblings. The final theory examined was that female sibling athletes would demonstrate a lower intercondylar notch width than the average woman. Both twins were on the low end of control values.
Uhorchak et al studied non-contact ACL injuries and associated risk factors over 4 years in 859 US military recruits.36 A predictive model was developed based on 24 non-contact ACL injuries that included the following factors: narrowed femoral notch width, increased body mass index (BMI), generalised joint laxity and increased KT-2000 scores (anterior/posterior tibiofemoral translation was quantified using the knee arthrometer (Medimetric, San Diego, California, USA)). These factors accounted for 28% of the variance in the occurrence of noncontact ACL injuries in all subjects, while it predicted 75% of the non-contact ACL injuries in women.36 Women with a BMI just 1 SD or more above average had a relative risk for noncontact ACL injury 3.5 times greater than women with a lower BMI, while high BMI men did not.36
Increased risk of ACL rupture in athletes is likely multifactorial and if genetic, is likely pleiotropic in nature. The sex disparity in ACL injury risk is clearly evident in the literature.3 However, it is unknown whether this is a sex-linked (X chromosome) trait. The risk factors of increased valgus joint loading, decreased intercondylar notch width, decreased hamstrings relative to quadriceps muscle strength and/or increased ligament laxity, especially about the knee joint, may lead to increased risk of ACL injury. These factors in combination may contribute to the final injury mechanism.
Non-contact ACL injuries typically occur with a combined mechanism of knee abduction, lower extremity valgus positioning, extension, rotation of the tibia and the foot planted away from the centre of mass, with the foot flat on the ground.30 The sports manoeuvres primarily associated with ACL injury are rapid deceleration during landing a jump or a change in direction during a pivot or cutting motion. Hewett and colleagues reported a high sensitivity and specificity for measures of dynamic valgus during landing to predict ACL injury risk,16 and adolescent women are at greater risk of a noncontact ACL injury because they land a jump with greater knee valgus than prepubertal women and men.6 10 14 18
It is difficult to address the prevention and treatment of ACL injuries in young athletes based on findings from a twin sibling study. However, what is currently known is that neuromuscular training conducted during adolescence appears to increase dynamic knee stability and to decrease knee and ACL injury risk.13 17 24,–,28 What is unknown is how to determine the high-risk population that can most benefit from neuromuscular training. Once isolated, those subjects at increased risk of ACL injury could undergo preventative neuromuscular training programs designed to reduce the risk of injury to the ACL. Questionnaires could be utilised to assess the presence of familial predisposition in a retrospective and prospective fashion. Screening tests could be used to identify athletes at high risk and target timing of intervention for injury prevention. With this information obtained, investigators may be able to determine when a subject may be at increased risk of knee injury, and additionally, if a subject's first-degree relative (ie, mother, father or sibling) may be at increased risk of knee injury.
Certain risk factors, including increased valgus joint loading and decreased intercondylar notch width, may occur in a family and may lead to the predisposition for ACL injury. There may be familial predisposition toward tearing of the ACL and therefore, there may be familial inheritance of neuromuscular and biomechanical risk factors for ACL injury. If risk factors such as increased valgus joint loading, decreased flexion, decreased intercondylar notch width and/or increased ligament laxity are present within a family, this would likely increase the likelihood of ACL injury among relatives. Clinicians may use greater information on the genetic basis of this important problem to develop methods to identify subjects with risk factors for ACL injury, including a family history, and institute appropriate interventions, or a neuromuscular training program or perhaps even notchplasty. The risk of ACL injury can be decreased in high-risk subjects with neuromuscular training.
Potential limitations
This study has numerous potential limitations. The biomechanical patterns demonstrated by sibling female athletes may not be able to be generalised to other athletes. We also examined biomechanical and neuromuscular control characteristics during landing. Though the majority of ACL injuries occur during landing, many result from cutting or pivoting manoeuvres, particularly in the sports of soccer and basketball.
Social, cultural, financial and environmental factors may account for or influence the predisposition of an athlete and their first-degree relatives to ACL injury. These influences should be studied before the relationship between the genetics of the athlete and ACL injury risk can be better understood. In addition, there is the question of how neuromuscular traits would be genetically transmitted. There would be potential environmentally inputs, for example, growth, development and prior training. Though there is some evidence for a genetic connection to ACL injury risk, other confounding and contributing factors must be considered. However, the two siblings and the uninjured controls played the same two sports on the same teams, which does control for some potentially confounding variables.5 In addition, our studies of the genetic underpinnings of ACL injury risk continue in large longitudinal cohort studies.
This study focused on the potential multifactorial nature of this important clinical problem, including the anthropometric, anatomic, biomechanical, neuromuscular, ligament integrity theories, with the assumption that other intrinsic and extrinsic factors are involved. Neuromuscular and biomechanical imbalances, intercondylar notch width and joint laxity may not be the only factors underlying the differences in knee injury rate, but they may be the greatest contributors to increased injury risk in women. However, the preponderance of data shows that neuromuscular differences affect injury rates and offer the greatest potential for intervention. The current observations support the hypothesis that there is a familial predisposition to ACL injury. In addition, it could be hypothesised from these findings that the familial predisposition is at least in part due to neuromuscular imbalance and decrease dynamic knee stability. It has been previously demonstrated that the neuromuscular imbalances can largely be altered with training, resulting in a decreased risk of ACL injury.15
Summary and conclusions
A relative paucity of literature has been published on the potential familial predisposition toward ACL injury. The purpose of this study was to determine if a familial predisposition to injury of the ACL of the knee occurs in twin siblings and what multiple, potentially heritable, factors may be related to this predisposition. Increased knee abduction angle, decreased intercondylar notch widths, increased general joint laxity and low H/Q ratios are potential traits related to the multifactorial familial predisposition to ACL injury. Quantification of these potential traits may lead to identification of athletes at increased risk of ACL injury, including those that possess a familial predisposition. The long-term objectives are to determine if a familial predisposition to ACL injury exists, and if so, to optimise the effectiveness of neuromuscular training designed to prevent knee ligament injuries in high-risk families. Determination of such a correlation may allow the investigators to achieve the long-term goal of reducing the rates of knee ligament injury in identified high-risk populations. Previous literature has elucidated several risk factors for tearing of the ACL. A number of risk factors including joint laxity, femoral intercondylar notch size and shape, hormonal influences, and ligament size which are considered to be intrinsic, or not changeable, in nature. Potentially controllable, or changeable, risk factors include knee abduction torque, neuromuscular firing patterns and proprioception. It is highly probable that many of the identified risk factors for an ACL tear are passed through families. Prevention would allow many thousands of athletes to continue the health benefits of sports participation while avoiding the long-term complications of osteoarthritis.22 Future investigations must incorporate combinations of these potential predictive variables in order to maximise the predictive potential of preparticipation assessment and the effectiveness of future interventions.
What is already known on this topic
Three published studies have reported familial history as a factor related to increased risk of anterior cruciate ligament (ACL) injury, while one study reported no such association. Athletes that experience an ACL tear demonstrate multiple factors that may predispose them to an ACL tear compared with controls matched for age, sex and sport.
What this study adds
This study supports earlier reports that family history of ACL injury may be a factor related to increased risk of ACL injury. In addition, multiple factors, including neuromuscular, biomechanical, anatomic, anthropometric and joint laxity characteristics, that may predispose athletes to an ACL tear, may be heritable in nature.
Acknowledgments
We would like to acknowledge team doctors Drs Angelo Colosimo and Jon Divine, and Donald Shelbourne for their patient records and contributions. We would also like to acknowledge Tinker Gray for her assistance with a critical reading of the manuscript.
References
Footnotes
-
Funding The authors would like to acknowledge funding support from National Institutes of Health Grant R01-AR049735 and R01 -AR055563.
-
Competing interests None.
-
Ethics approval Ethics approval was granted by the Cincinnati Children's Hospital Medical Center.