Article Text

Abstract
Background: Soccer heading has been proposed as a potential cause of cerebral dysfunction.
Objective: To examine the acute effects of two types of soccer heading on postural control.
Methods: Collegiate soccer players were randomly assigned to one of four groups: control, linear heading, simulated rotational heading, or rotational heading. Each subject completed a baseline postural stability assessment on day 1. On day 2 the same assessment was completed for the control subjects. The simulated rotational heading group completed a simulated heading drill before postural stability testing. The linear and rotational heading groups performed a heading drill with 20 balls at 88.71 km/h (55 mph), before postural stability testing. Separate one between (group), three within (surface, eyes, and day), mixed model, repeated measures analyses of variance were conducted on values for total sway and mean centre of pressure.
Results: The mixed model analysis of variance of results showed no significant differences (p>0.05) for the interactions of interest for either variable. Results suggest no acute changes in measures of postural control in soccer players completing either a linear or rotational soccer heading drill of 20 balls at a fixed speed.
Conclusion: Non-significant interactions between surface, eyes, day, and group indicate that sensory interaction of the balance mechanism components are not be compromised by the heading drill. This research supports previous studies suggesting that there are no acute risks associated with routine soccer heading. A direct comparison between these findings and those suggesting long term chronic deficits, however, cannot be made. Other studies that report chronic cerebral deficits in soccer players may have resulted from factors other than soccer heading and warrant further examination.
- COP, centre of pressure
- football
- soccer heading
- concussion
- postural control
- sensory integration
Statistics from Altmetric.com
Soccer is the most popular team sport in the world with nearly 200 million players.1 Unique among sports, soccer rules allow the players to stop and redirect the ball with the unprotected head. Heading is often linear with the player returning the ball from the direction it came. This is common in the midfield when a player returns a flighted ball. Rotational heading is also common, but occurs primarily within the penalty box. The player rotates his/her head to redirect a corner kick into the goal.
Heading in soccer has been criticised, as it has been suggested to result in chronic cerebral deficits.2–4 The long term effects of heading are speculated to be similar to punches to the head in boxing.5,6 There is opposing evidence from similar studies, however, that no cognitive deficits result from repeated exposure to heading.5,7
The long term consequences of boxing are well reported. Various studies using computed tomography, electroencephalography, and neuropsychological analysis have shown a variety of defects in boxers.8–10 Cerebral defects resulting from repeated blows to the head are commonly reported as dementia pugilistica or punch drunk syndrome. This condition appears to result from tissue alterations in several areas of the brain which may contribute to cognitive deficits such as decreased memory function.11
Clinicians commonly assess dementia pugilistica with a battery of neurocognitive tests that evaluate different aspects of cognitive function. A similar battery of tests is also used to assess concussed athletes.12–15 Although these tests have proved effective, researchers have combined them with assessment of postural control to gain a broader perspective of brain dysfunction after injury.13,16–18 Guskiewicz et al13 reported that a postural control assessment may offer greater sensitivity than pen and paper tests to evaluate brain dysfunction after sports related head injury.13
The purposes of this project were to (a) examine the effect of linear heading on postural control as measured by total sway and mean centre of pressure (COP), and (b) determine if rotation of the head alone or the combination of soccer heading and head rotation has a deleterious effect on measures of postural control.
METHODS
Forty collegiate soccer players (18 men, 22 women) volunteered for the study. Each subject read and signed the consent form approved by university’s institutional review board. They completed a brief questionnaire on age, height, weight, total number of soccer seasons played, and total number of previously diagnosed concussions. They were then randomly assigned to one of the four groups and followed the testing protocol outlined in table 1. Twenty four hours separated day 1 and day 2 testing sessions, and all day 2 testing was completed immediately after the heading drill or simulated heading drill.
Subject groups and testing order
An athlete was considered ineligible for participation if they were currently receiving treatment for a lower extremity injury or concussion. Subjects were tested during the offseason to avoid concurrent heading from practice sessions. Each subject was asked to refrain from physical activity before testing.
The heading simulation group performed simulated rotational heading. This consisted of jumping and rotating the head about 90° as if redirecting a corner kick into the goal. At no time did the subject’s head contact a soccer ball. This drill was completed 20 times over a 20 minute period.
For the linear and rotational heading, a JUGS soccer machine (JUGS International, Tualatin, Oregon, USA; fig 1) propelled each ball at an exit velocity from the machine of 88.71 km/h (55 mph) as indicated by the speed dials. The speed selected was the mean recorded from corner kicks of both the men’s and women’s varsity teams with a Stalker PRO (Applied Concepts Inc, Plano, Texas, USA) radar gun during pilot testing. This speed appears to be consistent with those previously reported.19

JUGS soccer machine and Adidas soccer balls.
The linear heading group linearly headed 20 balls over 20 minutes. For each header, the subject stood in the middle of the penalty box while one of five size 5 Adidas Gamarada Club Pro soccer balls (Adidas America, Portland, Oregon, USA) was launched from the mid-width of the soccer field (24.38 m (80 feet)). The subject was instructed to jump and contract the neck musculature isometrically as the ball approached. The ball was struck with the frontal bone just below the hairline and directed straight back to the machine. The instruction was to perform linear headers only.
The rotational heading group rotationally headed 20 balls over 20 minutes. To perform this manoeuvre, the subject stood in the same position on the field as the linear heading group and accepted balls from the soccer machine at the same speed. A rotational header involved jumping and rotating the head 90° at the moment of ball impact. The purpose of this action was to redirect the ball perpendicular to the trajectory and into a soccer goal. Subjects selected the direction in which they hit the ball (to the left or right), but were required to hit all 20 balls in the same direction.
We inflated soccer balls to the manufacturer’s guidelines of 0.70 bars of pressure. Each ball was checked before each testing session and adjusted to the appropriate pressure as necessary. More headers were performed in this study than is usual in a soccer match,20 but this volume appears to be consistent with previous work.21
We evaluated postural control using the “foam and dome” protocol initially reported by Shumway-Cook and Horak22 and implemented by Ingersoll and Armstrong16 for concussion evaluation. A Kistler type 9286A force platform (Kistler Instruments, Inc Winterthur, Switzerland), Airex Balance Pad (Airex, Sins, Switzerland), and a visual conflict dome were used. We constructed the conflict dome from a Chinese lantern and a sweatband with an “X” placed on the inside surface for the athlete to focus on during testing. Before testing, the athletes removed their shoes and socks and were instructed to remain as still as possible with their hands on their hips and their feet shoulder width apart. Each subject completed three trials of each of the six conditions that altered the visual and somatosensory inputs (fig 2).16 The order of the test conditions was randomised. Previous work with similar protocols reported an intrarater reliability of 0.92 and interrater reliability of 0.90.23
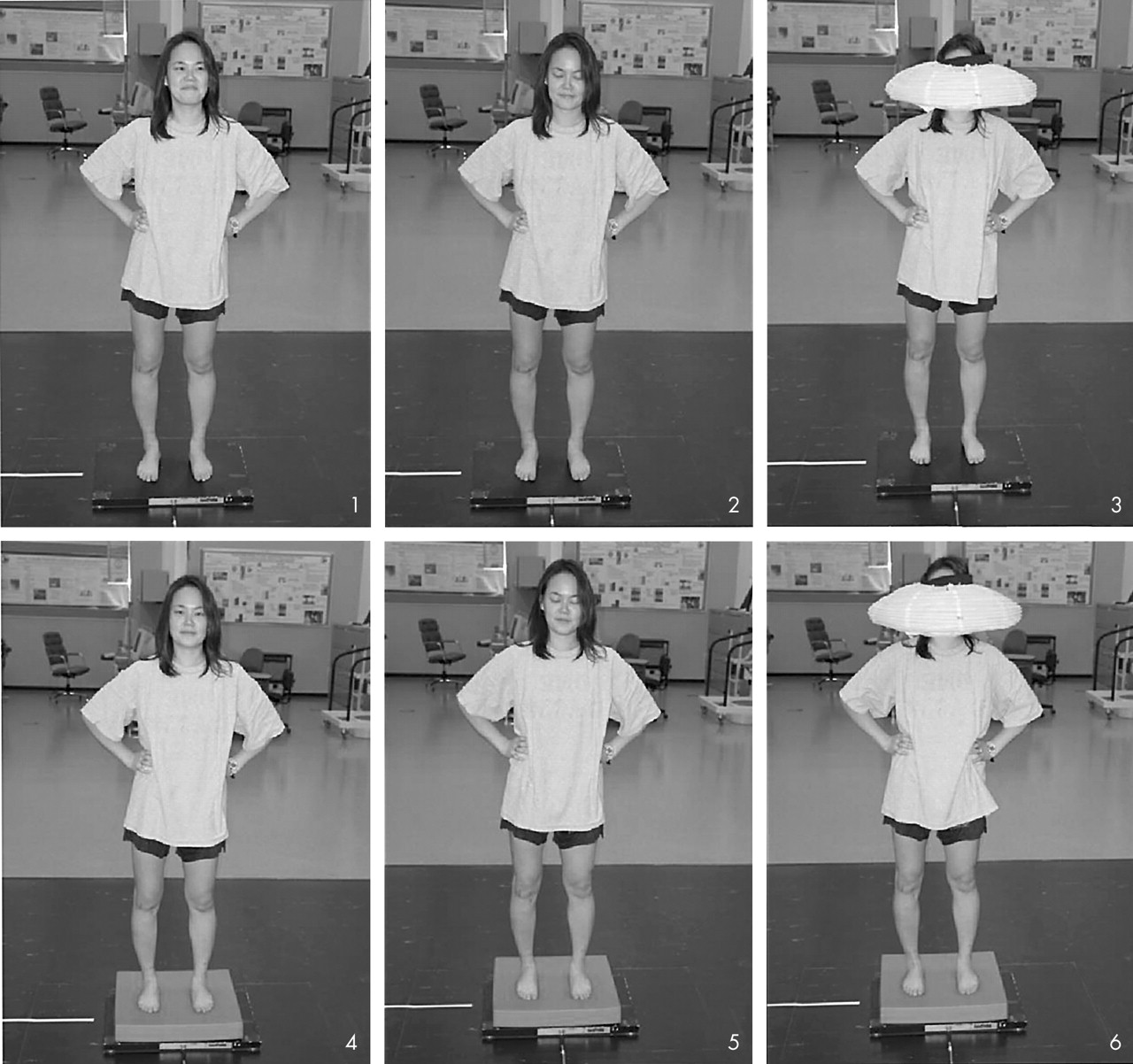
The six balance conditions. Conditions 1–3 are on a firm surface (force platform) with the eyes open, closed, and conflict dome respectfully. Conditions 4–6 are on a foam surface (Airex balance pad) with the eyes open, closed, and conflict dome respectfully.
Each trial lasted 20 seconds, with data collected at 100 Hz using the Bioware version 3.20 software (Kistler Instruments). A computer based spreadsheet program (Excel2000; Microsoft, Seattle, Washington, USA) calculated total sway and COP from the raw coordinates recorded by the Bioware software. We defined total sway as the sum of the COP movements occurring during the trial. COP was the mean distance the subject maintained their centre of pressure from the x = 0, y = 0 coordinate as previously used.17
Data analysis
Two separate two between (group, sex), three within (surface condition, eye condition, and day), mixed model, and repeated measures analyses of variance for total sway and COP were tested for significant interactions. The sex interactions of interest were non-significant, therefore the subjects were combined by group. Sex was removed as a between subject factor, and two separate one between (group), three within (surface condition, eye condition, and day), mixed model, and repeated measures analyses of variance for total sway and COP were tested for significant interactions. We implemented Pillai’s Trace criterion for data analysis interpretation as recommended by Keselman for robustness to test assumption violations.24 We conducted separate one way analyses of variance on the test group for age, height, weight, number of seasons played, and total number of previous concussions. Finally, partial η2 was calculated for the total sway and the COP interaction data. The level of significance was set at p<0.05 for all calculations, and all statistical analyses were conducted using SPSS (Chicago, Illinois, USA) version 11.0.
RESULTS
Table 2 gives basic data on the subjects in the test groups. Analysis of variance showed no significant differences (p>0.05) among the subject groups for age, height, weight, number of seasons played, and total number of previously diagnosed concussions.
Basic information on the test groups
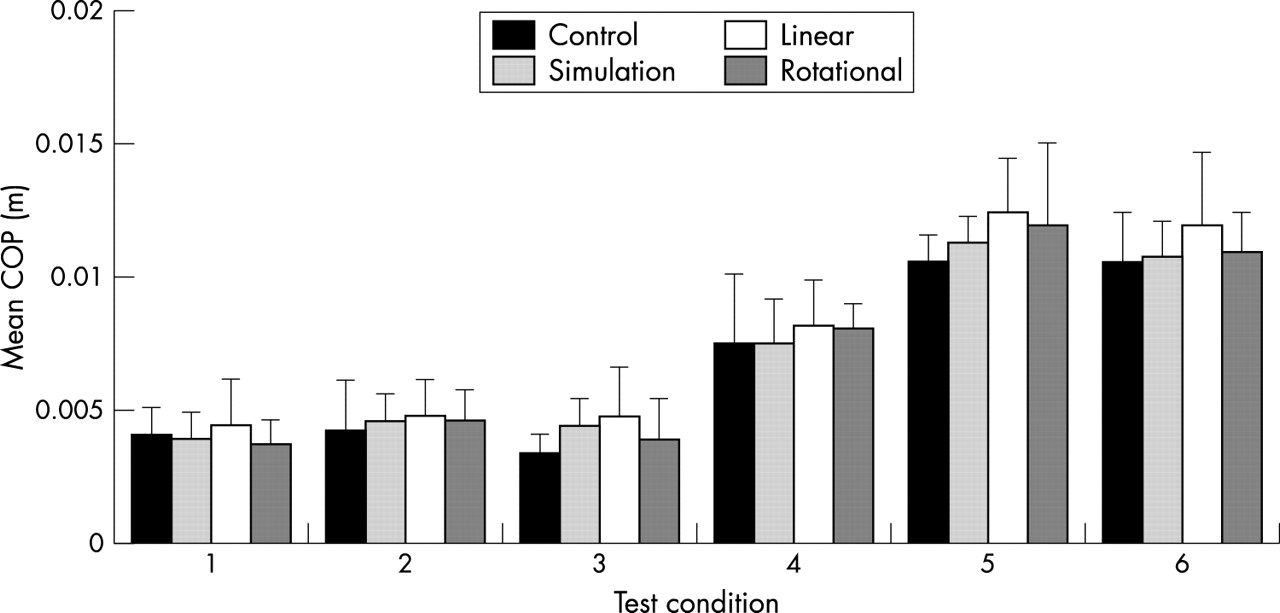
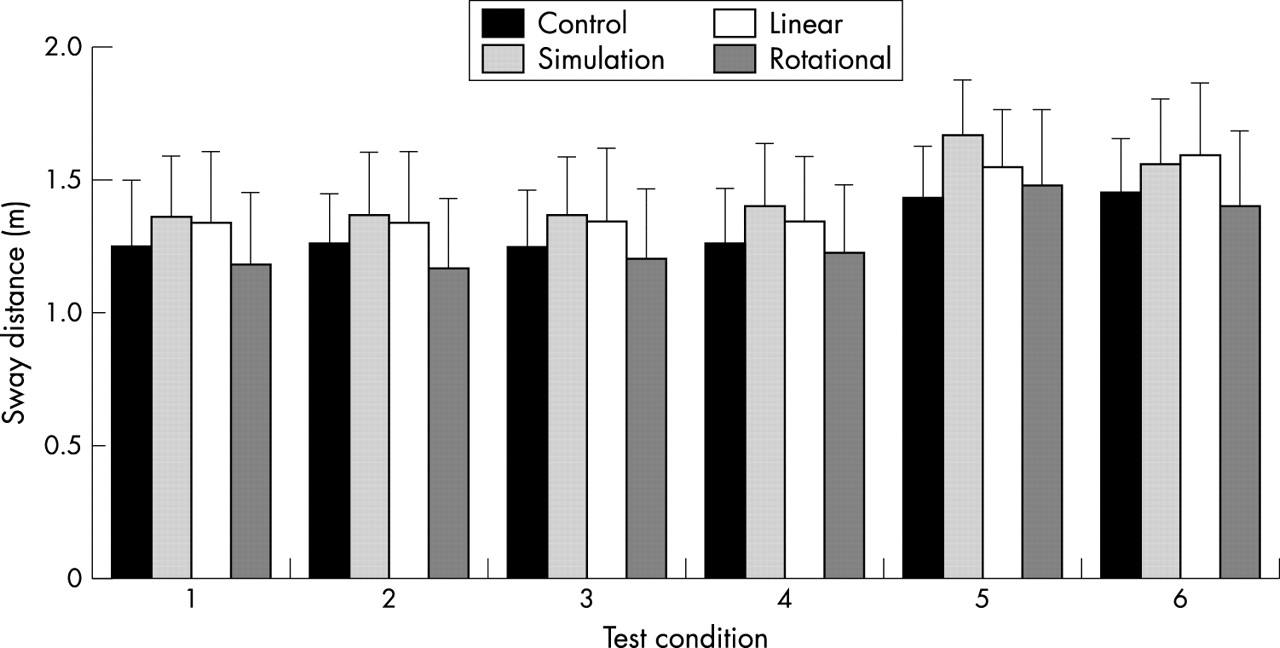
Figures 3–6 show means (SD) for total sway and COP. We examined the group × eye, group × surface, group × eye × surface, group × eye × day, group × surface × day, and group ×eye × surface × day interactions reported by SPSS. Analysis of variance conducted on total sway and the COP variables showed no significant main effect (p>0.05) for the interactions of interest (tables 3 and 4).
Mixed model analysis of variance for total sway
Mixed model analysis of variance for mean centre of pressure

Total sway on day 1 in the four test groups (controls, heading simulation, linear heading, rotational heading). Values are mean (SD).

Total sway on day 2 in the four test groups (controls, heading simulation, linear heading, rotational heading). Values are mean (SD).

Mean centre of pressure (COP) on day 1 in the four test groups (controls, heading simulation, linear heading, rotational heading). Values are mean (SD).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean centre of pressure (COP) on day 2 in the four test groups (controls, heading simulation, linear heading, rotational heading). Values are mean (SD).
DISCUSSION
Soccer heading has drawn criticism for potentially exposing the player to subconcussive forces that may result in chronic deficits similar to those seen in boxers. These deficiencies are similar to the acute deficits seen in concussed athletes. The most substantial finding in this study is the lack of significance supporting acute changes in postural control after a heading drill. A finding of no difference in measures of postural control between test groups suggests that soccer heading has no acute effect on balance-sensory interaction. Previous studies on both acute and subacute sufferers of head injury indicate that they have difficulty in processing sensory information to maintain normal balance during both quiet standing16,25 and under conditions of perturbation.13,14,17,26 We think it unlikely that 20 linearly or rotationally headed balls would have a similar effect.
Several researchers have shown that acute symptoms of concussion include deficits in postural control. These symptoms are most prominent immediately after head trauma, reportedly from decreased sensory integration capabilities, and subside within three days of injury.13,14,17,18 If the heading of 20 balls had acutely damaged the integration process, deficiencies would have become apparent with increased postural control measures of total sway and COP. It is possible that variations in movement strategy may have masked differences, making the test measure insensitive. Previous work with subjects with somatosensory or vestibular deficits has shown that measures of postural control may remain similar to those of control subjects, although the movement strategies about the ankle and hip differ.27,28 Horak et al27 suggest that appropriate movement around the ankle requires proper somatosensory input from that joint and vestibular information is necessary to maintain appropriate motion about the hip.
Previous studies of concussed patients have shown that their COP is maintained further from the centre of their base of support than in uninjured subjects.16,17 In a static stance, the maintenance of COP closer to the limits of stability means that only a small perturbation will initiate a fall, placing the person at greater risk of toppling over.16 Concussed patients also appear to show an increase in total sway, indicating greater movement of the COP within the limits of stability.17 Although such patients may wobble within their limits of stability, a greater total sway may not indicate an increased risk of falling. The location of the COP within the limits of stability may better predict equilibrium than total sway. If COP is maintained near the limits of stability with very little total sway, there is a greater risk of falling than if a large total sway is centred within the base of support.29 The increases in total sway and maintenance of COP further from the centre of the base of support observed in concussed subjects appear to result from sensory integration deficits.17
The central nervous system maintains postural control on both a conscious and subconscious level. Conscious actions (such as rising from a chair) are combined with subconscious reflexive actions that regulate muscle tension during the task. The somatosensory, vestibular, and visual senses provide environmental information to the central nervous system on limb proprioception and kinaesthesia, head acceleration, and referencing to a fixed point.30,31 Signals from these senses are processed within the basal ganglia (caudate nucleus, putamen, and globus pallidus), which initiate a response based on the current environmental conditions. The cerebellum integrates this information along with the intended actions of the motor cortex and coordinates the reflexive actions accordingly. An efferent signal is generated and passes through descending projections that influence alpha motor neurones, which innervate individual muscles acting to maintain postural stability.32 After a sports related head injury, athletes seem unable to apply visual and vestibular senses to maintain optimal balance.26 Thus, the cerebellum falsely integrates the current status of body position and erroneously signals the brain stem to activate inappropriate motor control patterns which result in non-optimal postural control strategies.
In this study, the postural control mechanism appears to be acutely unaffected by the linear and rotational heading drills. Had we seen acute deficits, we would have suspected trauma to the cerebellar or brain stem regions. Cerebellar injury would probably have occurred from a contrecoup injury. This may result from the impact of the ball moving the subject’s head in a whiplash-like motion, damaging the neural fibres of the cerebellum. Damage to the axonal fibres of the brain stem is also feasible, but less likely to occur from linear heading than rotational heading. These fibres are aligned longitudinally and provide increased resistance to tension loads33 that may result from the impact of the ball. The axonal fibres, however, do have a “selective vulnerability to rotational loading”,33 which may make them susceptible to injury during rotational heading. The heading manoeuvres performed in this project were controlled motions of the head. This allowed the neck musculature to prevent any extreme motion of the head about the neck, protecting the fibres of both the cerebellum and brain stem. Damage to these areas can and do occur in sports when an athlete cannot counter the external force to the head with the neck musculature. This is commonly seen in boxing.
The forces of impact from a boxing punch and a soccer ball have been reported to be similar. Atha et al34 reported a single punch acceleration of 53 g from a professional boxer. Peak accelerations from linearly headed balls can range from 49.3 to 54.7 g when kicked at 35–40 mph from 30 yards away.35,36 The number of blows to the head received by soccer players and boxers throughout their careers also appears to be similar. During a 50–180 match career, an amateur boxer sustains a median of eight blows to the head during a fight.10,37 This can amount to 400–1440 blows over total competition. A top level soccer player has a slightly greater total exposure, with an average of 6.66 headers per game or about 2000 headed balls over a 300 match career.20 Despite the source, a blow to the head always has the potential to cause damage.
Acceleration of the head that leads to neural damage may be more likely to occur during boxing than soccer. If the fighter does not see a punch coming or have time to tense the neck musculature, the risk of injury is increased. A soccer player will typically see the ball coming and can prepare for the impact, making neural injury unlikely during routine heading. In rare instances however, a player may unexpectedly take a blow to the head from a ball kicked at short range. The lack of preparation for a header can result in a whiplash-type injury which may lead to neural damage and concussion.19 This was unlikely in our study in which subjects were isolated from other players, allowing maximal heading technique. In matches, however, a player may be knocked by one of the opposition while attempting to head a ball, producing less than optimal heading technique. No reports could be found of routine soccer heading where the player was prepared directly resulting in concussion. However, Boden et al38 report a concussion resulting from a full force soccer ball kicked at the head of an unsuspecting player at close range. In conclusion, proper heading technique, paying attention to the game, and playing with skilful players may be the best defences against sustaining an injury from soccer heading. A variety of coaching manuals are available that discuss these topics in detail.
The postural control assessment in this study only evaluated one area of cerebral function. Neuropsychological tests would be valuable in assessing other areas of cognitive processing after head injury. We chose not to include a neuropsychological assessment, however, because similar research did not find any neuropsychological deficits after a comparable heading drill.21 The authors did state that the volume of headers may not have been sufficient to elicit detectable cognitive deficits. Other evaluations of chronic impairments in soccer players with neuropsychological tests and magnetic resonance imaging have produced similar negative results.5,7 However, neuropsychological analysis of professional soccer players suggests a risk of chronic deficits in cognitive function from repeated soccer heading.3 Other investigations using electroencephalography39 and computed tomography6 have also found chronic deficits, and therefore further investigation is warranted.
Some methodological limitations of this study should be considered. Although our results show medium to large effect sizes, a small sample size and therefore lack of power may blur our non-significant findings. An a priori power analysis to determine sample size was attempted, but deemed unfeasible because of the complex nature of the study design. Future studies should use a larger sample cohort to increase power. A bigger sample would also allow an additional analysis based on sex. In addition, the athletes used in our study were not given practice trials for the foam and dome balance assessment task which was novel to them. Therefore there is the possibility that practice effect improvements masked postural control deficits. Finally, our study only addressed one aspect of brain function. The exclusive evaluation of acute motor function in soccer players only allows a loose correlation with other studies of the chronic neuropsychological deficits of soccer players.
Conclusion
From the results of this study, soccer heading in a controlled environment does not appear to be acutely detrimental to postural control. Our findings suggest that no acute changes in postural control result from either a linear or rotational heading drill involving 20 balls at a fixed speed. No implications can be drawn about the chronic effects of soccer heading on postural control. Further studies that evaluate long term effects of soccer play after both practice and match participation are warranted.
What is already known
Results on the effect of soccer on cognitive function are mixed. European studies on professional and amateur soccer players suggest that they may be at risk of chronic neuropsychological deficits. Similar American studies have found neither acute nor chronic neuropsychological deficits.
What this study adds
Head injury evaluation requires a battery of tests to assess distinct areas of brain function. This study is the first to examine the acute effects of heading on postural control and adds to the growing evidence that heading in soccer is safe.